
Abstract
Background
Hypnosis was never used in sleep endoscopy assessment of obstructive sleep apnea syndrome (OSAS). The aim of the study was to assess the feasibility, safety, and patient satisfaction of hypnosis-induced sleep endoscopy (HISE).
Methods
From January to July 2021, 24 adults with moderate-to-severe OSAS at the polysomnography were included in the HISE protocol. The following outcomes were evaluated by the otolaryngologist and the hypnotherapist: safety, feasibility, and performance. The patient outcomes were assessed through a patient-reported outcome questionnaire assessing hypnosis acceptance, stress, anxiety, nasofibroscopy examination pain, and discomfort.
Results
Twenty-three patients completed the evaluations (16 males). The mean age of patients was 50.8 years. The nasofibroscopy was well-tolerated with low levels of stress during the HISE. Otolaryngologist adequately completed the VOTE scoring in 22 patients (95.7%). Hypnosis was ineffective in one patient because he felt pain during the nasofibroscopy procedure due to an important septal deviation. The hypnotherapist reported adequate satisfaction outcomes, with better results for trance compliance compared to other steps. There were no adverse effects or complications. The percentage of snoring was negatively associated with the level of consciousness during hypnosis (p = 0.012). The easiness of nasofibroscopy was positively associated with the levels of muscle relaxation (p = 0.036) and consciousness (P = 0.002).
Conclusion
HISE is an effective alternative approach for the work-up of OSAS. Future controlled studies are needed to compare HISE with drug-induced sleep endoscopy and assess the cost-effective outcomes of both approaches.
Introduction
Obstructive sleep apnea syndrome (OSAS) is a prevalent disorder affecting 2% to 7% of the adult population of the Western countries.1,2 OSAS is associated with cardiovascular, cognitive, stroke disorders, and death.2,3 The identification of the upper airway collapse site is commonly performed through drug-induced sleep endoscopy (DISE), which provides useful information for the therapeutic strategy. 1 The classical DISE method is based on the use of continuous propofol infusion and, as DISE requires anesthesia, this procedure is commonly performed in the operating room. 1 This outpatient approach is usually performed in operating room, and requires the patient monitoring after the anesthesia. The cost of DISE ranges from $2400 to $11,818 in the U.S. and is related to operating room requirement and the use of drugs. 4 In this preliminary study, we assessed the feasibility, safety, and patient satisfaction of hypnosis-induced sleep endoscopy (HISE).
Methods
Patient setting
From January to July 2021, adults with moderate-to-severe OSAS at the polysomnography (PSG) 5 were recruited from the Sleep Center of Poitiers (Poitiers, France). The severity of OSAS was defined according to the report of the American Academy of Sleep Medicine and based on the patient apnea hypopnea index (AHI): mild (5-14 events/hour); moderate (15-30 events/hour); or severe (>30 events/hour). 5 PSG results were analyzed by a board-certified otolaryngologist (FB). Patients with the following conditions were excluded: mental health disorders, smoking, alcoholism, heart or neurological severe disorders, history of head and neck cancer or radiation, chronic rhinosinusitis, and recent history of upper aerodigestive tract infection.
The institutional review board approved the study protocol (Poitiers Ethics Committee, ref. 20.11.13.75306/CPP2020-12-103a/2020-A02419-30L). The study was conducted according to the reporting guidelines for prospective studies (CONSORT Statements). The informed consent was obtained for all patients.
Hypnosis protocol
Three hypnosis sessions were proposed to patients prior the HISE. The hypnosis session was carried out in a soundproof room with softened lighting and ambient temperature according to the recommendations of the French hypnosis society. The first, second, and third hypnosis sessions were carried out in seated, half-seated and supine positions, respectively. The common steps of the conversational hypnosis protocol included induction, dissociation, hypnotic trance, relaxation, suggestion, and re-association. 6 In the last hypnosis session, otolaryngologist explained to patient the steps of the nasofibroscopy and introduced the fiberscope (Xion®, 3.7 mm, Xion inc., Germany) into the upper aerodigestive tract of patient.
The acceptance of the procedure was assessed throughout this last step. The otolaryngologist did not use nasal/local anesthesia during the acceptance session and the HISE. The light of the fiberscope was turned on after the introduction of the fiberscope into the nasal cavity to reduce the risk of patient wake-up. The otolaryngologist stopped the fiberscope in the nasopharynx a few seconds without touching the soft palate throughout the nasofibroscopy of the last hypnosis session and the HISE. The soft palate (muscle) relaxation or its vibration (snoring) were evaluated throughout this HISE step. The next step of the procedure consisted of the assessment of the pharyngeal cavity through the velum oropharynx tongue base epiglottis (VOTE) classification system. 7
Hypnosis, sleep, and satisfaction outcomes
Otolaryngologist and hypnotherapist assessed the feasibility of the procedure through a physician-reported outcome questionnaire including patient compliance, HISE feasibility, and performance outcomes. The patient fulfilled a reported-outcome questionnaire assessing hypnosis acceptance, stress, anxiety, nasofibroscopy-related pain, or discomfort. The overall score of both questionnaires ranged from 20 (low satisfaction) to 80 (high satisfaction; Figure 1). Consort chart flow.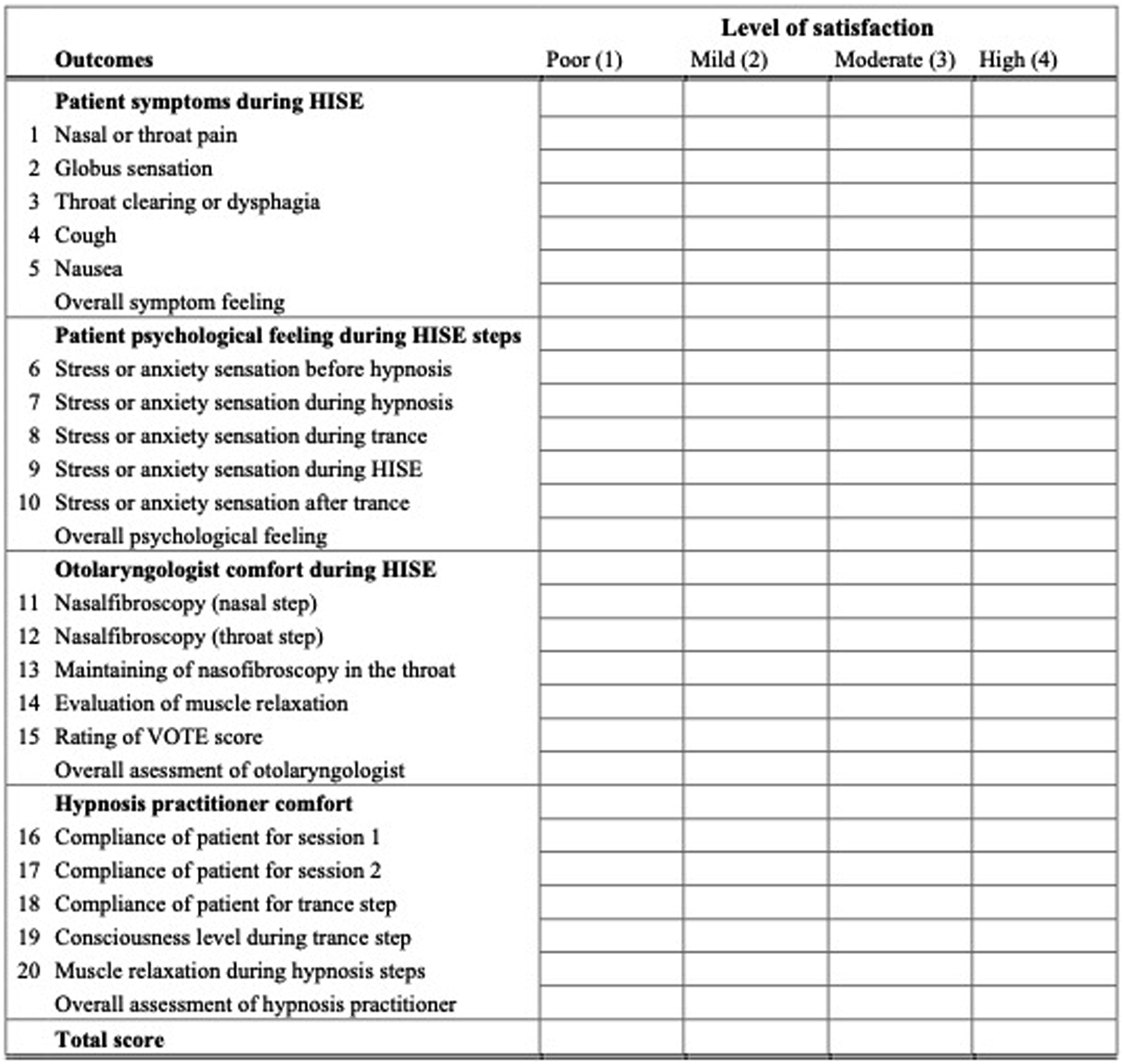
The micro-awakenings/annoyance/pain were assessed during the procedure as well as the anatomical location(s) of collapse. The patient compliance to hypnosis was evaluated by the hypnotherapist through the practitioner-reported outcome questionnaire after the HISE.
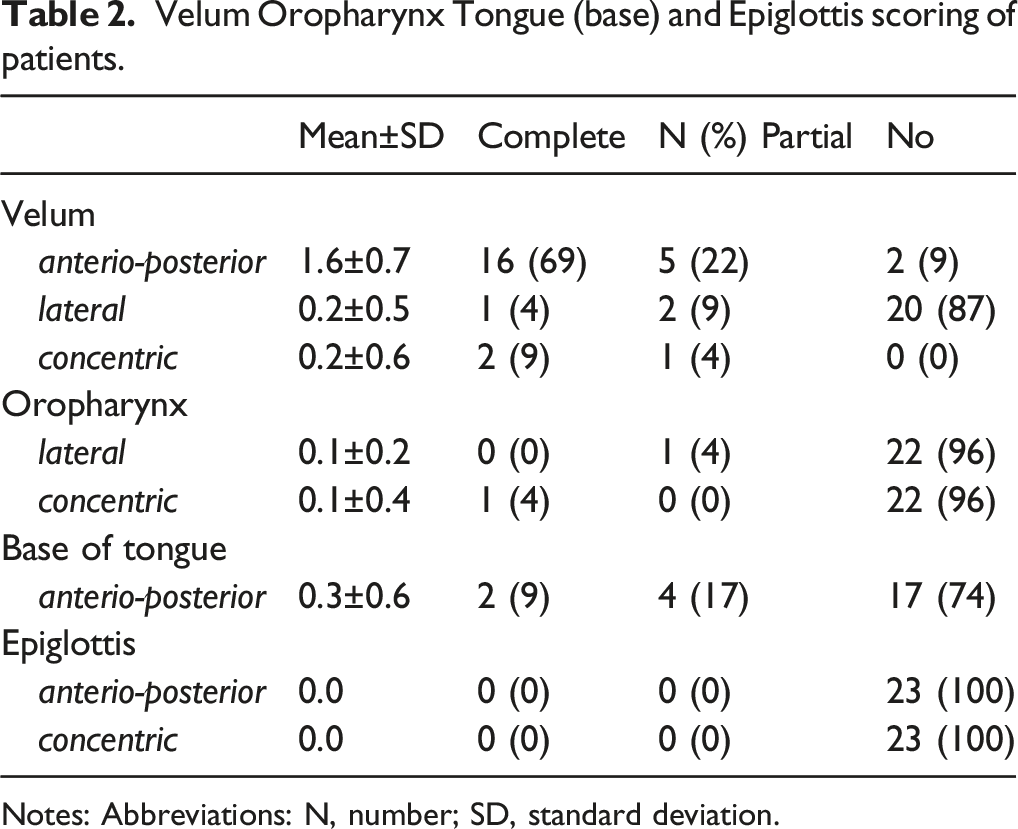
The otolaryngologist used the VOTE system for each patient. The VOTE classification assesses the degree of obstruction of anatomic structure and the configuration of the obstruction. The configuration of obstruction can be described as antero-posterior, lateral, or concentric. Antero-posterior obstruction consists of a contact between anterior and posterior (posterior pharyngeal wall) anatomical structures, while lateral obstruction is laterally located structures moving towards the center of the airway. The combination of the 2 previous obstruction types is described as concentric. 7 The score of each anatomical region ranges from 0 (no obstruction) to 2 (complete collapse). The otolaryngologist proposed a therapeutic strategy depending on the HISE findings.
Statistical methods
Statistical analyses were performed using the Statistical Package for the Social Sciences for Windows (SPSS version 27.0; IBM Corp, Armonk, NY, USA). The association between outcomes was investigated with multivariate analysis. A level of significance of P < 0.05 was used.
Results
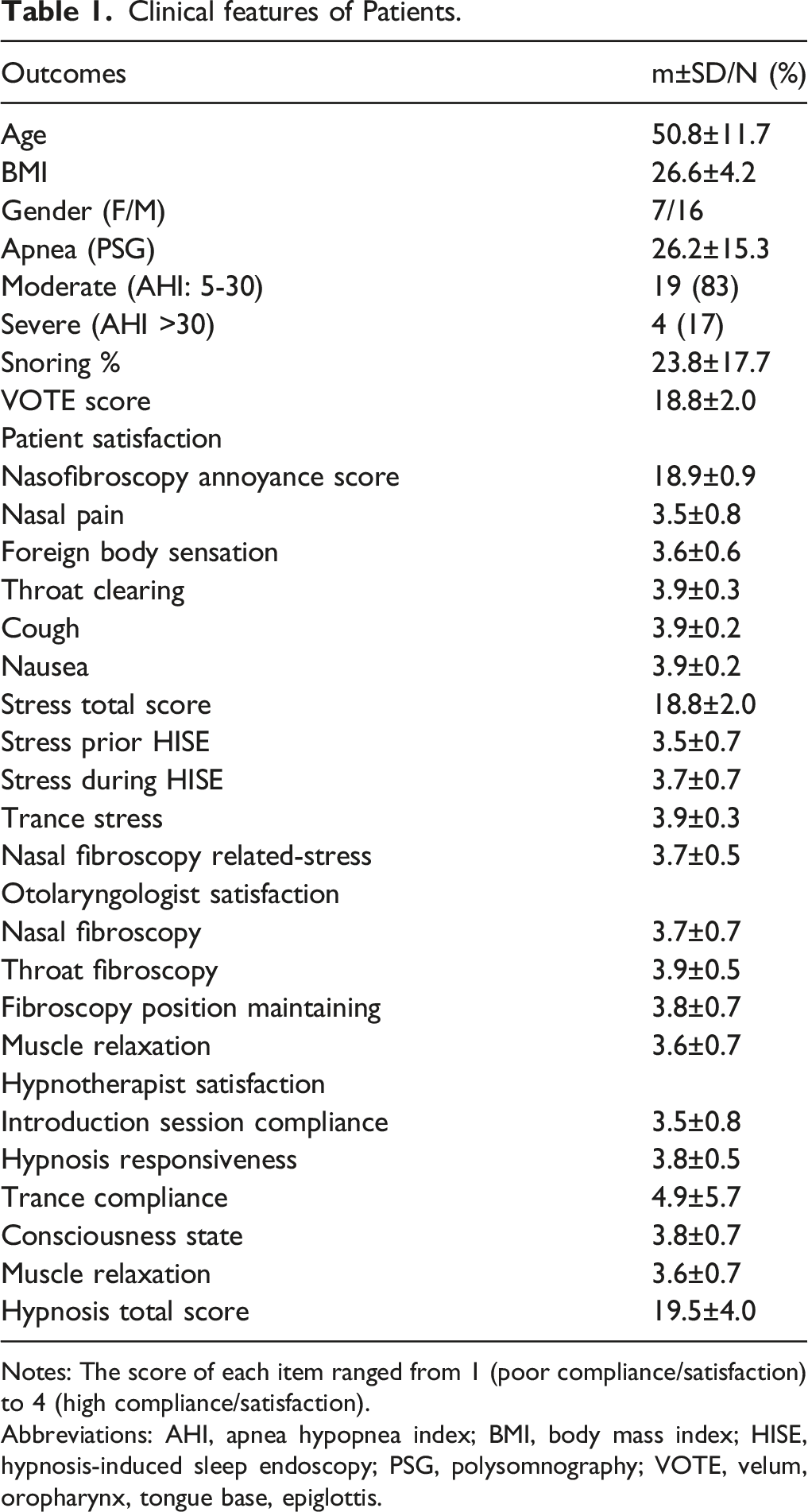
Twenty-four patients completed the evaluations (Figure 2). There were 16 males and 8 females. The mean age of patient was 50.8 years. The OSAS features of patients were described in Table 1. The mean body mass index was 26.6. The hypnosis was ineffective in one patient because he felt pain during the procedure due to a bilateral septal deviation (4.3%). Moreover, this patient reported a low susceptibility to hypnosis. Most patients had moderate OSAS considering the AHI at the PSG (Table 1). The patient satisfaction outcomes were reported in Table 1. The nasofibroscopy was well-tolerated, while the level of stress during the HISE was low. The VOTE scoring was adequately completed in 23 patients (95.7%; Table 2). The most common anatomical regions of obstruction were velum and oropharynx. Otolaryngologist reported patient reaction during the hypnosis process when the fiberscope touched the soft palate in 45% of cases (N = 11), but that was not associated with a wake-up or an inability to continue the examination. The hypnotherapist reported adequate satisfaction outcomes, with highest results for trance compliance (Table 1). There were no adverse effects or complications throughout the HISE. Comfort and satisfaction scale for patient, otolaryngologist and hypnotherapist. Each item was assessed with a Likert-scale ranging from 1 (low satisfaction) to 4 (high satisfaction). For each person (patient, otolaryngologist, hypnotherapist) the score ranged from 5 to 20. The total score of scale ranged from 20 to 80. Abbreviations: HISE, hypnosis-induced sleep endoscopy; VOTE, velum, oropharynx, tongue base, epiglottis. Clinical features of Patients. Notes: The score of each item ranged from 1 (poor compliance/satisfaction) to 4 (high compliance/satisfaction). Abbreviations: AHI, apnea hypopnea index; BMI, body mass index; HISE, hypnosis-induced sleep endoscopy; PSG, polysomnography; VOTE, velum, oropharynx, tongue base, epiglottis. Velum Oropharynx Tongue (base) and Epiglottis scoring of patients. Notes: Abbreviations: N, number; SD, standard deviation.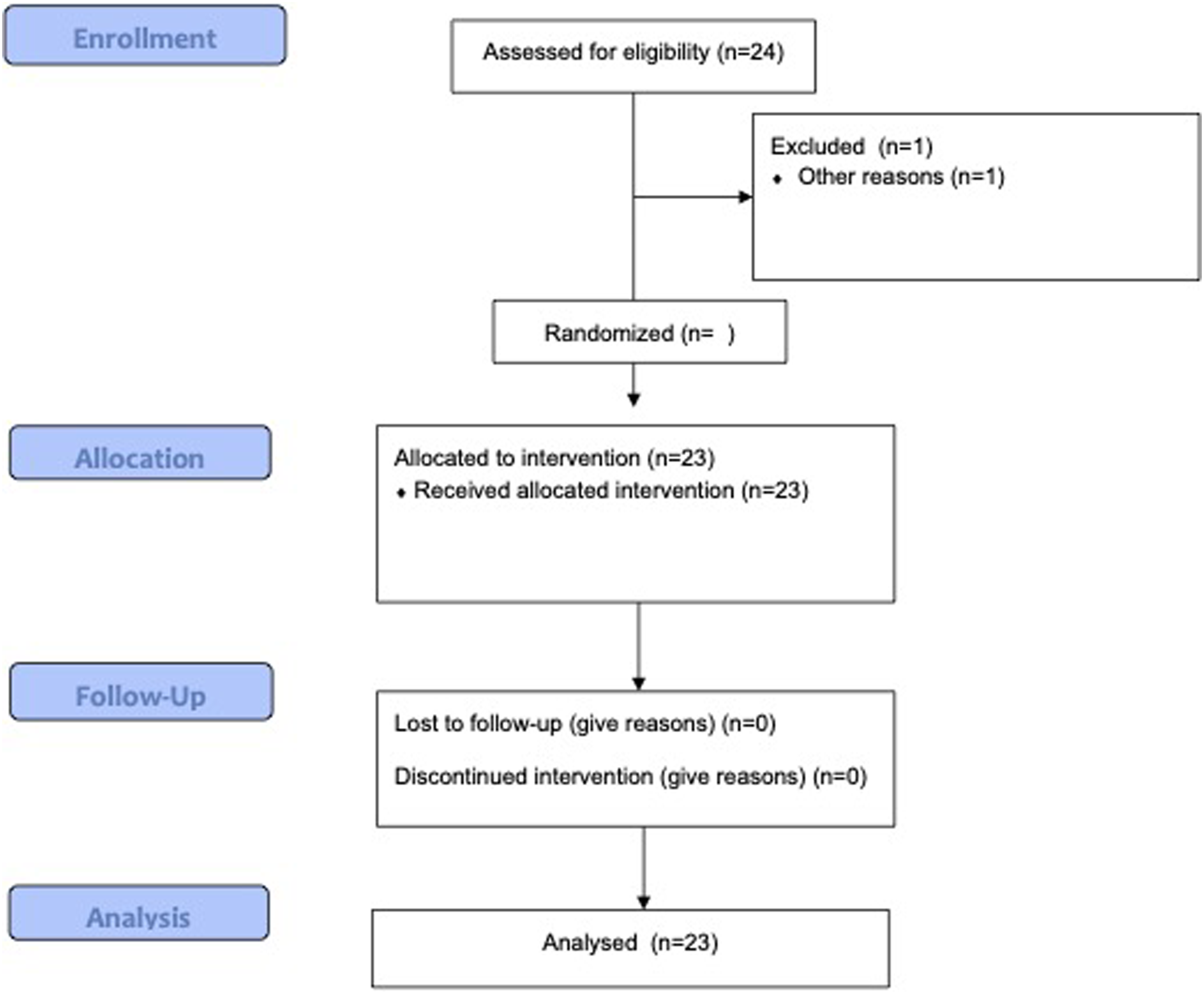
The multivariate analysis reported a negative association between the percentage of snoring and the consciousness state of hypnosis (rs = -0.527; P = 0.012). The severity of pain during the first nasofibroscopy was positively associated with the level of stress during the HISE (rs = 0.581; P = 0.004) and the severity of VOTE scoring (rs = 0.421; P = 0.046). There were negative associations between the responsiveness of the first hypnosis session (rs = -0.517; P = 0.012) and the overall satisfaction of hypnotherapist (rs = -0.675; P = 0.001). There were significant positive associations between the level of difficulty to perform the nasofibroscopy (VOTE scoring) and the levels of patient stress during HISE (rs = 0.492; P = 0.017) and trance step (rs = 0.691; P = 0.001). The easiness of nasofibroscopy was positively associated with the levels of muscle relaxation (P = 0.036) and consciousness (P = 0.002).
Discussion
The DISE is one of the most frequent procedures in otolaryngology-head and neck surgery. Because DISE is carried out in operating room and associated with the use of drugs, the procedure is costly for patients and/or healthcare systems. 4 For this reason, some practitioners have tried to develop alternative approaches carrying out a modified DISE protocol outside the operating room. 8
The usefulness of hypnosis in sleep disorders was previously investigated in pediatric9,10 and adult 11 populations in the management of insomnia, acclimatization of noninvasive positive pressure ventilation or in weight loss in OSAS patients. To the best of our knowledge, this preliminary study is the first investigation reporting safety and feasibility of HISE in patients with moderate-to-severe OSAS. In this study, we described a step-by-step protocol, which is easy to apply in daily practice.
Because this study is the first investigation dedicated to HISE, the discussion of our data with the literature remains limited. According to our protocol, most patients were sensitive to hypnosis (95%). The HISE procedure failed in one patient who reported mild hypnotherapy susceptibility and nasal pain throughout the nasofibroscopy. Interestingly, the low susceptibility to hypnotherapy may be easily detected throughout the hypnosis sessions that preceded the HISE. The hypnotic susceptibility was adequate in approximately 80% to 90% of the general population, which may support our success rate. 12 The sleep endoscopy was successfully achieved in 95% of cases, leading to proposition of personalized sleep therapy. The success rate of HISE was closest from the success rate of DISE, which reaches 100% despite of the lack of significant impact of sleep endoscopy on surgical sleep outcomes. 13
According to patient, nasal pain during the nasofibroscopy and the stress related to the procedure were the most important issues, while the assessment of the muscle relaxation was the most difficult step for the otolaryngologist. The patient fear about the HISE procedure may be reduced during the 3 initial hypnosis sessions, which indicates the need to improve our hypnosis session protocol. The difficulty to assess the muscle relaxation during the HISE procedure may be related to the lack of drug used for anesthesia, which are known to facilitate the muscle relaxation, and, therefore, the detection of collapse. 14
HISE appears to be a cost-effective approach, which is its primary advantage. Indeed, the use of drugs, the occupation of the operating room, and the requirement of the anesthesiologist team are costs 8 that are avoided with HISE. Moreover, HISE may be interesting for patients with drug contraindication. Our study highlights that the selection of patients is an important point. Indeed, the responsiveness to hypnosis requires the lowest level of pain during the examination.
In our study, the easiness of nasofibroscopy was positively associated with the levels of muscle relaxation and consciousness, which indicates that it is important to prepare the patient to the procedure through 3 preliminary hypnosis sessions in which practitioners assess the hypnosis responsiveness, the stress/anxiety of patient and the nasal permeability in nasofibroscopy. The importance of the preparation to HISE was strengthened by the influence of the patient stress level on the feasibility of nasofibroscopy, and the realization of the VOTE scoring.
The primary limitation of the present study is the lack of control group. However, this is a feasibility study, which aimed to explore the feasibility and the safety of HISE before the conduction of large-cohort controlled investigations. The lack of brain monitoring is another limitation because it would highlight the effects of hypnosis steps on cerebral function. Future controlled studies need to compare the levels of sedation and consciousness between hypnosis-induced and drug-induced sleep endoscopies using the bispectral index (BIS) monitor.
Conclusion
HISE is a feasible and safe approach for the management of patients with moderate-to-severe OSAS at the PSG. Future controlled studies using bispectral index (BIS) monitor are needed to compare the effectiveness of HISE versus DISE and to investigate the cost-effectiveness of both strategies.
Footnotes
Acknowledgments
B. Johnson for the proofreading of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Elsan Care (2019).
Ethical approval
The local ethics committee approved the study protocol (Elsan Ethics Committee; 20.11.13.75306/CPP2020-12-103a/2020-A02419-30L). Patients consented to participate.