
Abstract
Introduction
Obstructive sleep apnea (OSA) is a prevalent disorder with significant adverse impact on a patient’s individual health and on the healthcare system.1-6 Various treatment options, both invasive and noninvasive, exist for OSA, with varying degrees of effectiveness.7-17 While widely regarded as the gold standard therapy, continuous positive airway pressure (CPAP) is poorly tolerated by many patients, with common reasons including poor fit, nasal/oral cavity dryness, cosmesis, and claustrophobia. 11 Despite improvement in mask types, development of quieter machines, increase in behavioral interventions, and/or patient coaching in recent history, a 2016 systematic review found no significant increase in CPAP adherence rate over the past 20 years. 11 With a mean CPAP nonadherence rate of 34% in the same study, Rotenberg et al 11 questioned the effectiveness of CPAP as the gold standard therapy, given that more than a third of patients are noncompliant and/or undertreat their OSA.
Hypoglossal nerve stimulation (HGNS), using the breathing synchronized Inspire Upper Airway Stimulation device (Inspire Medical Systems, Inc), is an emerging surgical treatment option for patients with moderate to severe OSA [apnea-hypopnea index (AHI) ≥15 and ≤65 events/hour of sleep] who are unable to tolerate or have failed CPAP.10,18-21 Prior to implantation, patients are selected for HGNS first by drug-induced sleep endoscopy (DISE) demonstrating an anterior-posterior collapse pattern without complete concentric collapse. 18 HGNS, via stimulation of the hypoglossal nerve, protrudes and stiffens the genioglossus muscle during respiration, which may eliminate the obstructive site inducing apneas or hypopneas.18,20
Prior publications have demonstrated the efficacy of HGNS in reducing AHI and Epworth sleepiness scale scores, with one study reporting reduction in blood pressure (BP) following the operation as well.20-23 Given its relatively new introduction to market, the full impact of HGNS on patient health outcomes remains under investigation. Not only are HGNS outcomes limited to certain measures, but existing data are all produced by large academic centers. In this study, the authors aim to explore the effect of HGNS on AHI, BP, hemoglobin A1C (A1C), body mass index (BMI), and the number of antihypertensive and/or diabetic medications taken by patients to contribute toward contemporary understanding of this novel procedure.
Patients and Methods
A retrospective review of adult patients with OSA from a single private practice center was conducted. All patients at least 22 years of age with an AHI between 15 and 65 events/hour, a BMI ≤32 kg/m2, who were not tolerating CPAP therapy with a DISE demonstrating anterior-posterior collapse pattern of the upper airway at Specialty Physician Associates, and subsequently underwent HGNS between January 2020 and November 2022 were eligible for study inclusion. Patients who did not acquire a titration sleep study with the HGNS were excluded. This study was approved by our Institutional Review Board.
Patients’ medical records were reviewed for demographics, tobacco and/or alcohol usage history, AHI, BMI, mean arterial pressure (MAP), number of daily antihypertensive medications, A1C, and number of daily diabetic medications. MAPs were calculated by utilizing the formula MAP = diastolic BP (DBP) + 1/3 (systolic BP − DBP). The preoperative BP was extracted from the consultation visit with sleep medicine, or from the nearest primary care record if BP was not measured at the sleep medicine consultation. The postoperative BP was extracted from the most recent visit with sleep medicine after titration, or their primary care visit if not available in the sleep medicine records. The method of measurement of BP was performed at the discretion of these departments. The preoperative A1C was considered the most recent value available prior to intervention, and the postoperative A1C was the most recent value available after intervention.
Statistical analysis and data management were performed using the statistical software, R (v.4.2.1; R Core Team).24,25 A paired Student’s T test was performed to assess for postintervention differences, McNemar’s exact test was used to assess for change in patients requiring ≥3 antihypertensives, and Fisher’s exact test was used to assess the overall distribution of antihypertensive medication requirements. P values less than .05 were considered statistically significant.
Results
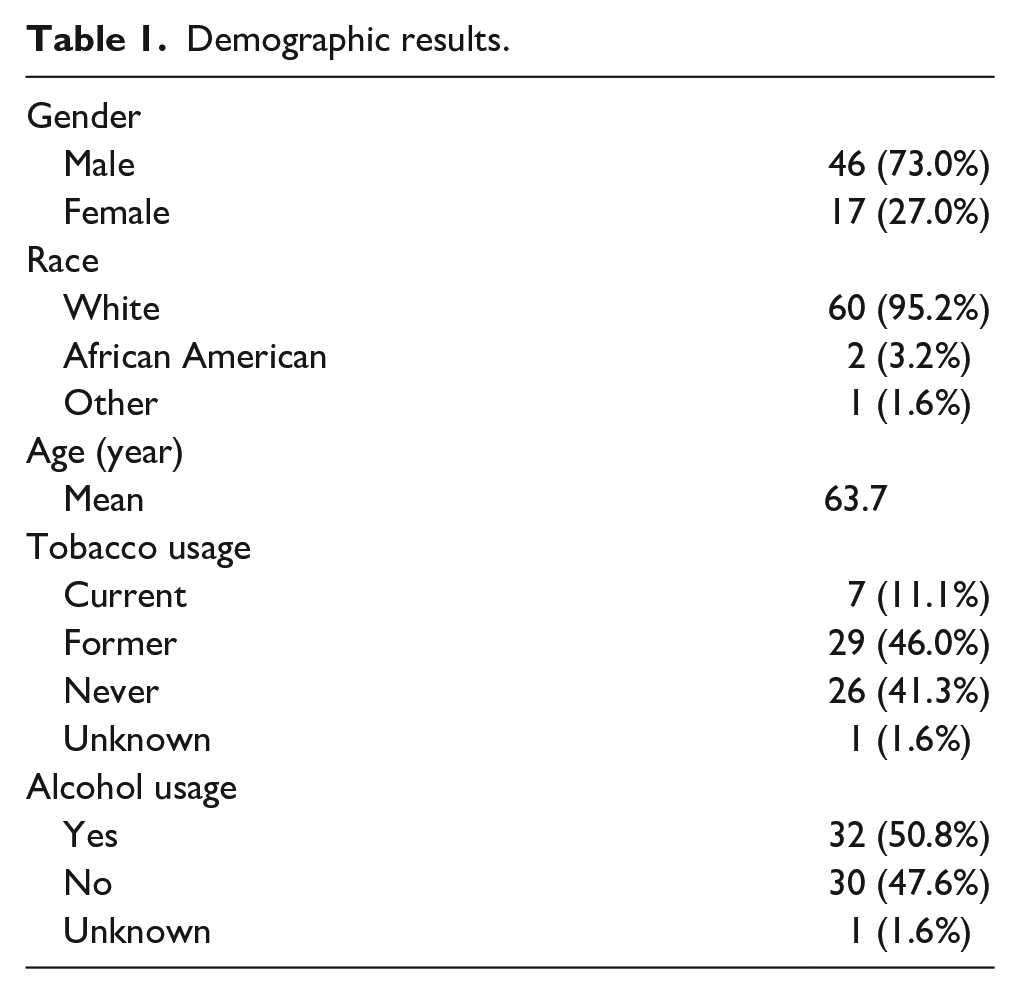
Among 91 charts reviewed, 63 met the inclusion/exclusion criteria for this study and were included. The demographics of our population are summarized in Table 1. The patient population for our study was predominantly male (73.0%), white/Caucasian (95.2%), with a mean age of 63.7. Only 11.1% were current smokers and 50.8% reported current alcohol usage before HGNS. A total of 22.2% of patients carried a diagnosis of diabetes mellitus.
Demographic results.
The mean preintervention AHI was 33.17 compared with 5 postintervention for a mean change of −28.16, P < .0001, 95% confidence interval (CI) 22.7-32.1. The mean number of days from implantation to post-titration sleep study was 169.8 with a standard deviation of 77.9. There was no significant change in BMI (SD) following the intervention, with the mean remaining essentially unchanged from 29.4 (3.2) to 29.84 (3.6) post intervention. We observed a statistically significant change in MAP, decreasing from 99.4 mmHg to 90.99 mmHg representing a mean change of −8.4, P < .0001, 95% CI 5.8-11.4.
The overall distribution of BP medication requirements also significantly changed following the intervention with Fisher’s exact test yielding P < .0005. Prior to intervention, 22.3% of patients required 3 or more BP medications, and following intervention, only 12.7% of patients required the same level of medication with McNemar’s exact test yielding P = .03. The distribution of antihypertensive medications taken by patients and the total number of medications taken pre- and postintervention by patients are recorded in Tables 2 and 3, respectively. The mean A1C (SD) decreased from 6.67 (1.06) to 6.16 (0.68), for which the change did not meet significance. Of the 2 patients on diabetes medications, 1 had lower requirements following implantation. Combined pre- and postintervention data illustrating the changes in health outcome measures mentioned above are summarized in Table 4 and graphically in Figure 1.
Blood pressure medications.
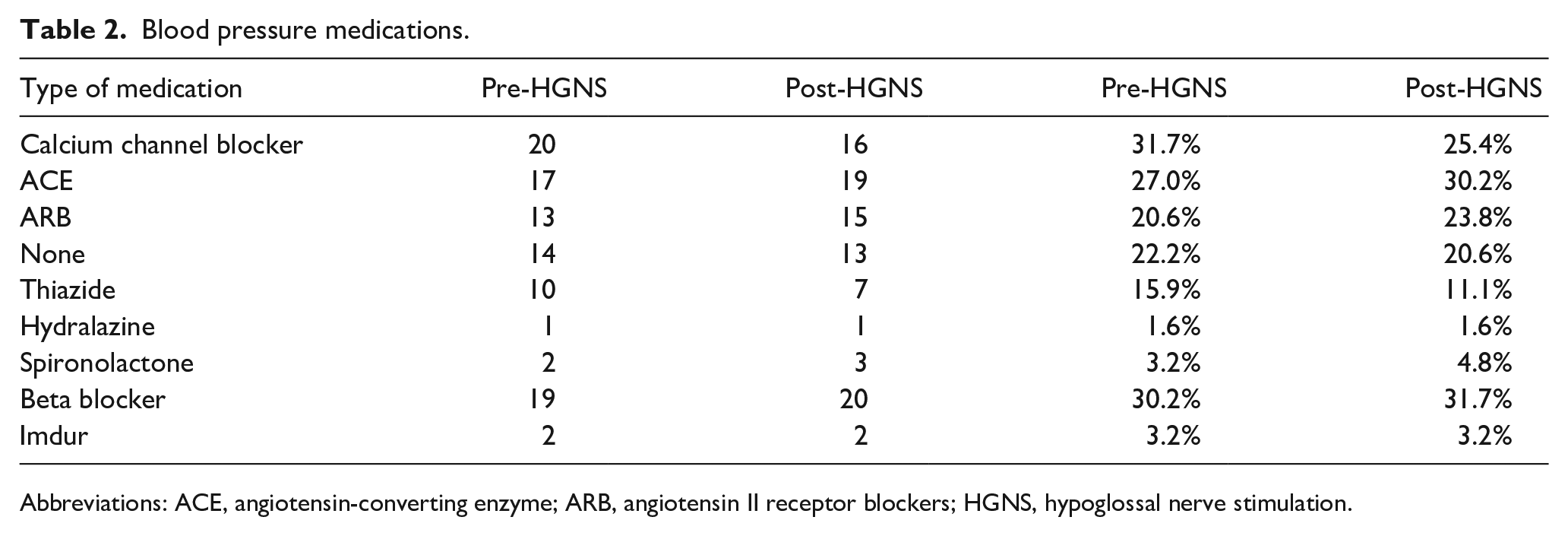
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blockers; HGNS, hypoglossal nerve stimulation.
Number of blood pressure medications.
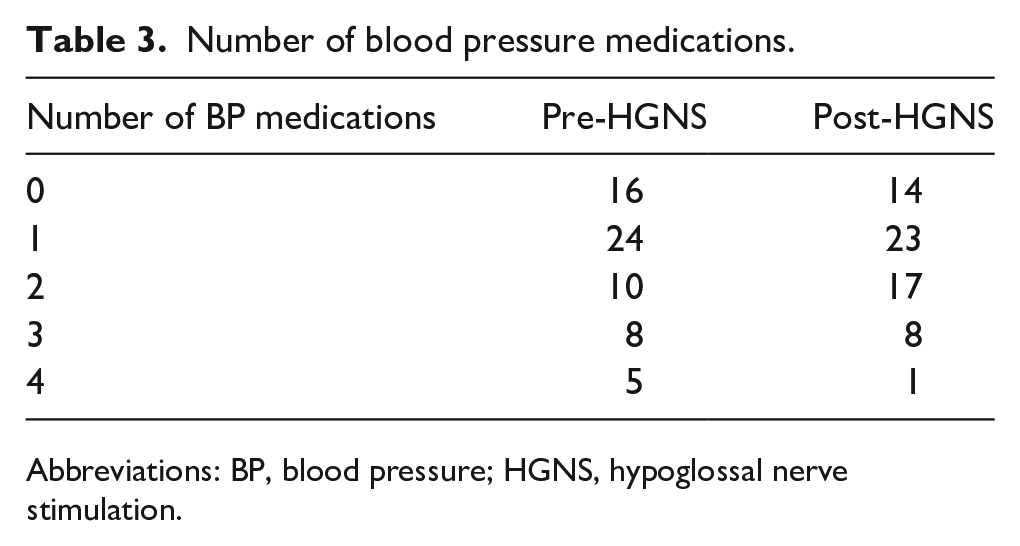
Abbreviations: BP, blood pressure; HGNS, hypoglossal nerve stimulation.
Primary results.
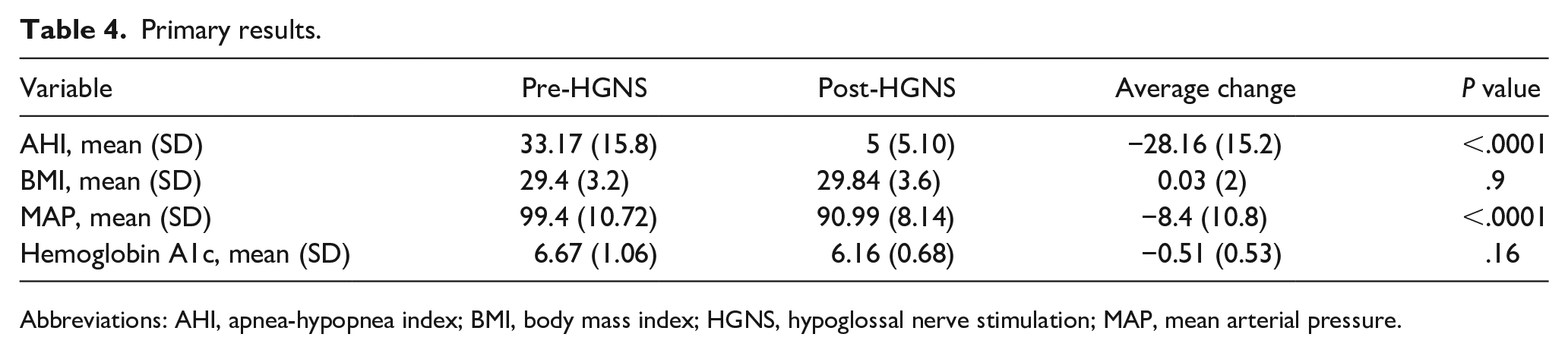
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; HGNS, hypoglossal nerve stimulation; MAP, mean arterial pressure.
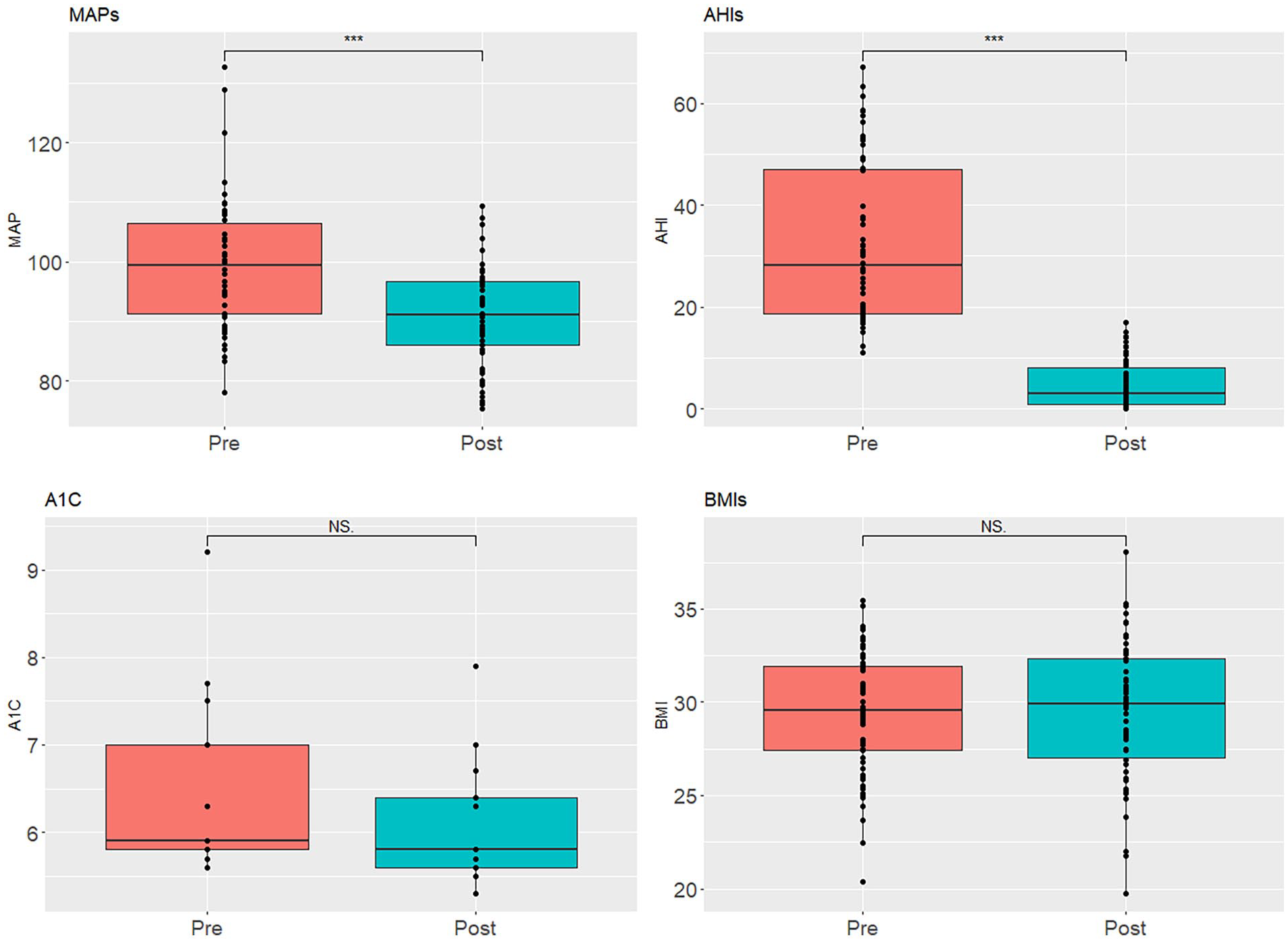
Box plots of pre- versus postoperative changes in apnea-hypopnea index, blood pressure, hemoglobin A1C, and body mass index following hypoglossal nerve stimulation operation. ***, P < .0001. NS, P > .05.
Discussion
OSA is a prevalent disorder in both adult and pediatric populations, affecting men more commonly than women. 7 A study in Switzerland found that 49.7% of men and 23.4% of women have moderate to severe OSA (AHI ≥15 events/hour). 7 When mild OSA (AHI ≥5 events/hour) is also considered, the prevalence of OSA approaches 50% for the general population.8,9
The burden of OSA is felt on both individual and healthcare system levels. Patients with OSA have increased rates of hypertension, obesity, diabetes, cardiovascular diseases, and stroke.1-4 In addition, patients with OSA may experience excessive daytime sleepiness, mood disorders, decreased overall quality of life, and loss of productivity. 6 The American Academy of Sleep Medicine estimates that more than $150 billion dollars are spent annually in the United States treating conditions developed due to untreated OSA. 5
Adverse structural and functional aspects of the upper airway both contribute to a pattern of repetitive airway collapse in OSA. 26 Unfavorable anatomic characteristics increase the likelihood of OSA, in addition, during sleep, there is a decrease of tonic input to the upper airway dilator muscles, which diminishes airway patency. 26 Repetitive cycles of the apnea/hypopnea episodes result in poor sleep quality and negative downstream health outcomes.26,27
CPAP is the gold standard treatment option for all severities of OSA; however, it is often poorly tolerated by patients with suboptimal adherence rates.10-14,18 The Inspire® device is the first and only HGNS to receive Food and Drug Administration approval since 2020, offering an alternative procedure for treatment of moderate to severe OSA.10,28,29 To date, more than 40,000 Inspire® devices have been implanted in over 900 medical centers worldwide. 29 Multiple studies have demonstrated the effectiveness of HGNS, with greater than a 70% reduction in postoperative AHI reported.22,30
Similarly, our data support the effectiveness of the Inspire® device, with a significant improvement in mean AHI from 33.17 events/hour to 5 events/hour, just at the threshold of mild sleep apnea representing near complete resolution of OSA P < .0001 (Figure 1).
Multiple studies have found an association between OSA and poor cardiovascular health, with worsening hypertension being one of the adverse outcomes.1-4 We identified a significant decrease in mean MAP (99.4-90.99, P < .0001, 95% CI 5.80-11.4) following HGNS implantation (Figure 1). This association reinforces a recent study by McKinlay et al 23 which also demonstrated a significant reduction in DBP and MAP in 30 patients before and after HGNS implantation. 23 In the study by McKinlay et al, 23 there was a mean change in MAP of −3.7 mmHg with a mean reduction in AHI of 18.6 events/hour, compared with the mean change in MAP of −8.4 mmHg and mean reduction in AHI of 28.16 events/hour in this study. Our study’s findings of increased change in AHI and MAP relative to the study of McKinley et al may suggest a relationship between the 2, which could be the subject of future research conducted in a prospective fashion.
When looking at the antihypertensive medication requirements of patients before and after HGNS implantation, 2 interesting observations were made. First, the overall distribution following implantation significantly changed with Fisher’s exact test yielding P < .0005. Second, prior to HGNS implantation, 22.2% of patients required 3 or more antihypertensive medications, which decreased to 12.7% following the procedure with McNemar’s exact test yielding P = .03. The concurrent findings of a significant decrease in both MAP and the proportion of patients requiring ≥3 BP medications are suggestive of improvement in BP control following titration. To our knowledge, our study is the largest and only the second report to demonstrate significant changes in MAP, and the first to illustrate a significant change in antihypertensive medication requirements after HGNS.
OSA negatively affects endocrine homeostasis and has previously been found to be associated with increased rates of diabetes and metabolic syndrome.1,6 In our study cohort, 14 (22%) patients had a diagnosis of diabetes mellitus, and the mean A1C was 6.67 prior to HGNS implantation and 6.16 afterward. The 0.51 reduction rate did not reach significance with a significance value of .16. However, the overall decrease observed is an interesting signal which merits further investigation with a larger sample size. Of the 2 patients on diabetes medications prior to the intervention, 1 was able to reduce/eliminate their medication requirement.
No significant changes in BMI pre and post HGNS implantation were identified (Figure 1). Preimplantation BMI was recorded at the office visit nearest to the date of the procedure, while postimplantation BMI was recorded at the patient’s most recent office visit following the titration study. As such, a plausible reason for the lack of BMI decrease may be inadequate length of time between the HGNS implantation and BMI measurement. Sustained weight loss requires persistent lifestyle changes including dietary modification and increase in physical activity, which may not be accurately reflected in shorter periods of time. 31 In theory, a decrease in AHI and Epworth sleepiness scales after appropriate treatment of OSA should provide patients with more energy, making physical activity more feasible and appealing. Interestingly, a 2021 meta-analysis performed on weight change with CPAP use demonstrated a statistically significant increase in weight with less than 5 hours/night of compliance, for which the same was not observed in patients with greater than 5 hours/night of compliance. 32 Association between BMI reduction and HGNS has yet to be demonstrated in the literature, and studies with longer follow-up periods are warranted for further investigation.
Our study has several limitations. The retrospective nature of data collection precludes collection of subjective information essential for accurate assessment of pathologic severity and treatment effectiveness. All data collected were from a single private practice center in Pennsylvania, which limits the external validity of the findings for other practice settings and/or geographic regions. The small number of participants, predominantly older white males, restricts this study’s implications for other demographic groups. Last, 3 different operating otolaryngologists were involved in this study, each with their own surgical style, postoperative instructions, and follow-up timeline, which may lead to uncontrolled variables.
Further investigation into the effect of HGNS implantation on various outcome measures of health is necessary with larger sample sizes. In this study, the number of patients with diabetes was inadequate to identify a statistical change in A1C or any changes in diabetes medications utilized. In addition, no change in BMI was observed which could be secondary to the relatively short-term follow-up of this study. Further studies, ideally prospective in nature, evaluating these indicators of health in addition to others not discussed in this article would provide further insight into the long-term impact that HGNS may have on a patient’s overall health.
In conclusion, HGNS has a multifaceted positive impact on patients with moderate to severe OSA. Significant reduction in AHI and MAP, number of antihypertensive medications utilized daily, were observed after HGNS implantation. This is the second and largest cohort study to demonstrate the effect of HGNS on BP changes following the procedure. No significant changes in BMI or A1C were noted.
Footnotes
Data Accessibility
The data that support the findings of this study are available from the corresponding author (JAK) on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.