
Abstract
Penetrating neck injuries (PNIs) can present as a simple wound or can be complicated by a disruption of the airway or associated vasculature. As such, stabilization of the vasculature and the airway is paramount. Here we present a case in which a hemodynamically stable 28-year-old female presents with a PNI involving the oropharynx and laryngopharynx.
Introduction
A penetrating neck injury (PNI) is any neck injury that pierces the platysma muscle. PNIs have been shown to occur in approximately 10% of all trauma cases 1 and while they may present as a simple wound, some studies show that up to 80% of patients have damage to major structures of the neck. 2 The management of the airway in PNIs has historically depended on the specific case, 3 and therefore no definitive method has been characterized, allowing physicians to manage difficult airways individually. This case represents a patient who maintained a stable airway despite a significant PNI. We aim to highlight our approach to airway stabilization for a patient with a PNI.
Case Report
A 28-year-old female was transported by helicopter after being stabbed in her right cheek with a throwing knife during a domestic fight with her boyfriend. She was flown in by emergency medical services awake and able to suction her own oral cavity. The otolaryngology team was paged prior to the patient’s arrival and asked to be present. On arrival to the Emergency Department, ABCs were re-assessed, and the patient was able to protect her airway and suction her mouth without assistance. She was also able to communicate by writing. Figure 1 shows the trajectory of the knife with an entry point in the right cheek and the tip of the knife palpated subcutaneously in the contralateral left neck. Crepitus was present, but there was no palpable expanding hematoma. Her facial nerves were also intact.
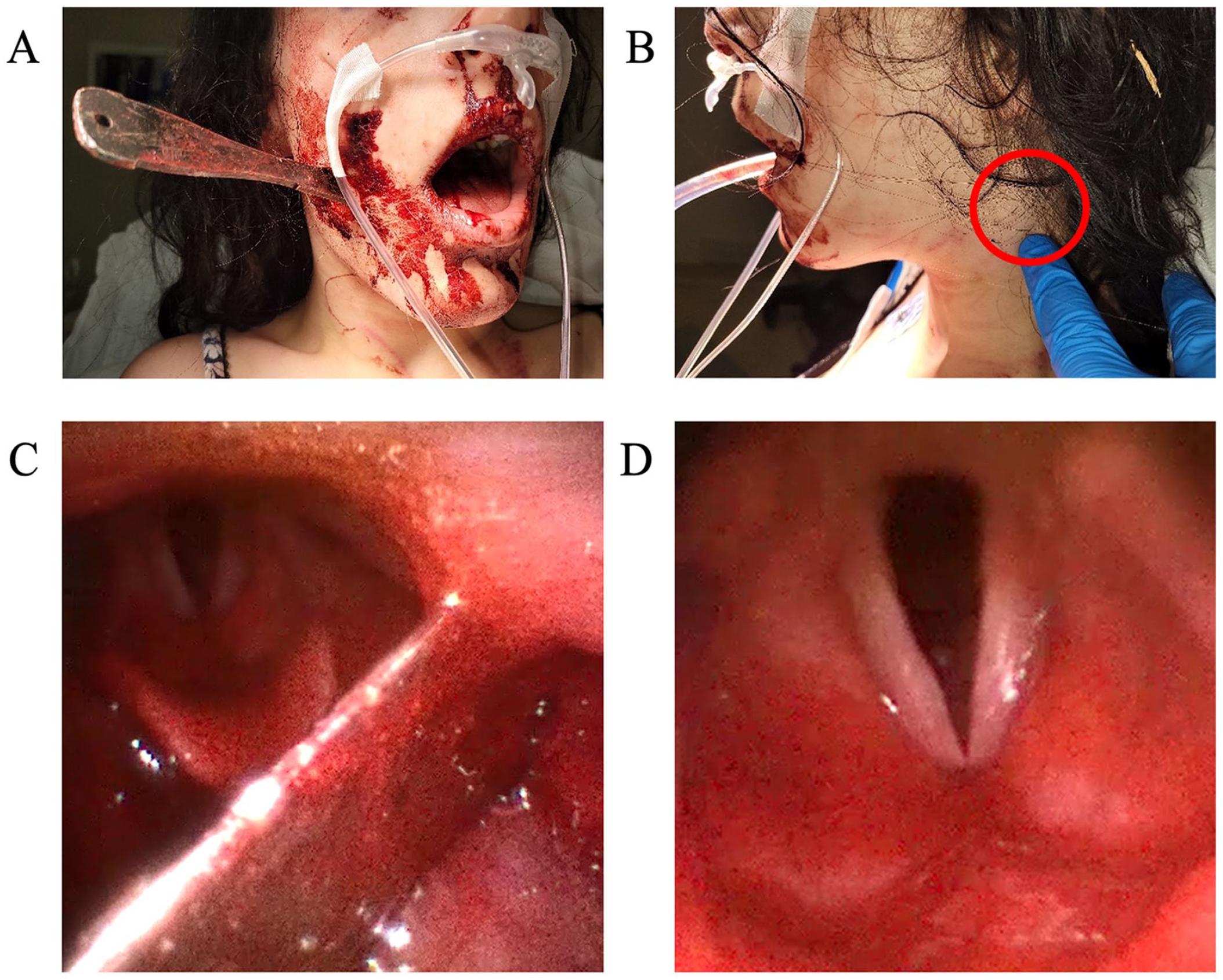
(A) Entry point of the knife in the right cheek. (B) Tip of the knife located subcutaneously in the contralateral neck. (C) Trajectory of the knife in the oropharynx. (D) A more distal view of the patent protected glottis with normal functioning vocal cords bilaterally.
Since the patient was stable, flexible laryngoscopy was performed showing the trajectory of the knife entering the right oropharynx anteriorly with posterolateral projection to the left lateral pharyngeal wall, just anterior to the epiglottis and superior to the base of the tongue (Figure 1). There was pooled blood in the supraglottis and laryngopharynx, but the glottis was patent, and the cords were functioning normally bilaterally.
We also assessed for the presence of a large vessel injury. While the patient was hemodynamically stable and her airway was relatively stable, she would not have tolerated lying supine for a computed tomography angiography (CTA). Therefore, our next step was to secure the airway in the operating room with the anesthesia team. We reviewed the laryngoscopy video with the anesthesia providers and made decision for awake nasal fiberoptic intubation through the right nostril, as it had a more accommodating anterio-posterior dimension to accommodate the nasotracheal tube. A tracheostomy set was open and ready with an otolaryngology resident scrubbed in should a surgical airway be required. Anesthesia performed an awake nasal fiberoptic intubation.
With the airway secure, we then took the patient to the CT scanner and performed a CTA of the head and neck (Figure 2). The artifact from the knife limited the examination but there was question of left external carotid injury without obvious extravasation or transection. The internal carotid arteries and vertebral arteries appeared intact bilaterally. We took the patient back to the operating room where we performed a left neck exploration over the palpable knife tip (Figure 3). The carotid sheath was identified and found to be intact and the knife was carefully removed. The wound bed was further evaluated with no significant bleeding. The pharyngeal defect was then identified through the neck and repaired with sutures. The wound was irrigated and closed and a closed suction drain was left in place.
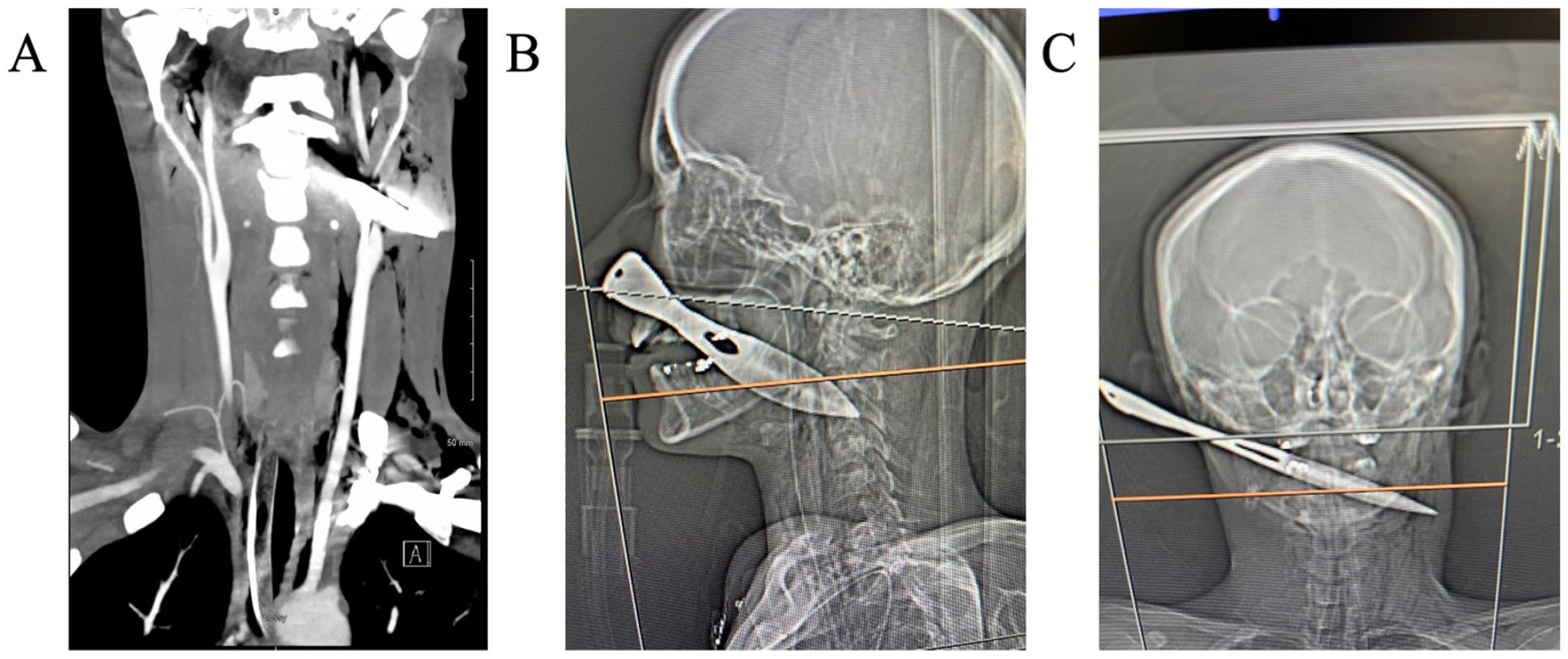
(A) Coronal computed tomography angiography (CTA) showing artifact around the left internal and external carotids with intact distal runoff without obvious extravasation. (B) Sagittal computed tomography (CT) scout image showing the anterior to posterior trajectory of the knife. (C) Coronal CT scout image showing the right to left trajectory.
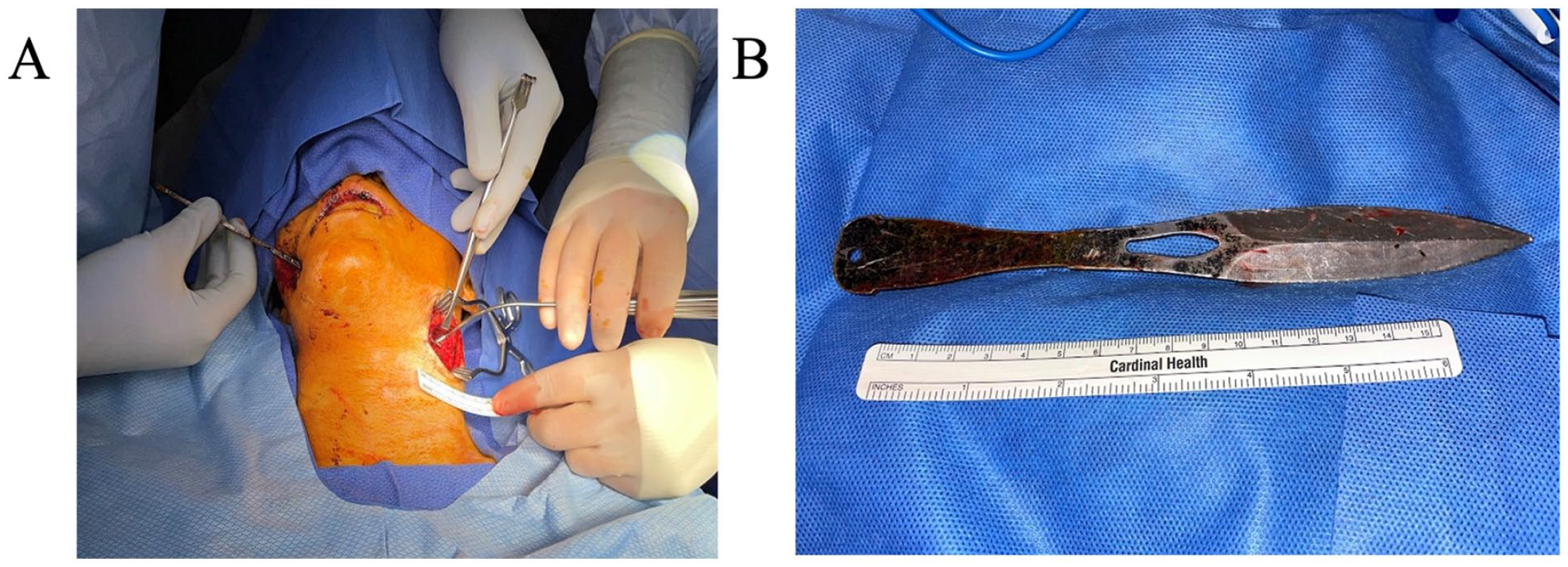
(A) Intraoperative image of the left neck exploration with the tip of the knife exposed without obvious bleeding from surrounding structure. (B) The extracted knife measuring approximately 20 cm.
We then proceeded with an exploration of the right facial entrance wound, which was irrigated and closed externally and intraorally. Direct laryngoscopy was performed showing the repaired pharyngeal defects and a superficial base of tongue laceration. The patient tolerated the procedure well. A Dobhoff tube was placed, and she was then extubated without difficulty.
The patient was kept wihout oral intake with all medications and nutrition via a Dobhoff tube to allow healing of the oropharyngeal defect. She was also placed on prophylactic Unasyn throughout her admission. A modified barium swallow study was performed on postoperative day 5 which was passed with no evidence of extravasation. The patient was started on a full liquid diet, which was well tolerated. The Dobhoff tube was removed and the patient was discharged. The patient did well after discharge except for some pain control issues. She had a prior history of narcotic dependence and received them regularly though her primary care doctor. She was seen in the clinic 1 month postoperatively and was noted to be tolerating a diet with well-healing incisions.
Discussion
Penetrating trauma can range from a shallow wound that violates only the subcutaneous tissue to the violation of the more important structures of the head and neck, such as the great vessels or airway. Vascular injuries are not uncommon given the proximity of these vital structures to the skin surface with some studies showing vascular injury of up to 30%.1,4 Although hemodynamic stability is certainly an aspect of PNI to be concerned about in the initial evaluation, airway stability is equally important. There is considerable variability in airway management with penetrating trauma and options will vary greatly from case to case. 3 In our case, the patient was hemodynamically stable and the airway was relatively stable, in part due to the patient’s good Glasgow Coma Scale (GCS) status and her ability to remain calm and collected while suctioning her own airway. This gave us the luxury of being able to perform flexible nasolaryngoscopy for a better view of the airway before proceeding. Notably, we made use of the Ambu® video flexible laryngoscopes (Ambu Inc., Columbia, MD, USA), which gave us the ability to record and review with anesthesia prior to intubation. This allowed for a strong multidisciplinary approach to secure the patient’s airway.
In the Advanced Trauma Life Support (ATLS) guidelines, if one is able to oxygenate a relatively stable airway but predict that it will be difficult, then considering an awake intubation is recommended. 5 Two additional considerations included the diameter of the narrowed oropharynx due to the presence of a foreign body and whether the endotracheal tube could be damaged by the sharp edge of the knife. Therefore, we decided to enter through the right nostril given the more flexible AP diameter between the knife and the posterior oropharynx. Furthermore, we had multiple endotracheal tubes ready in case the cuff was damaged by the knife. Finally, it is important to prepare for a surgical airway as an alternative if intubation fails. We typically inject the neck with local anesthetic and epinephrine on the patient’s arrival to the operating room. The scrub technician and a provider may also be scrubbed with an open tracheostomy set at the ready. The unique trajectory of the penetrating injury and stability of this patient at arrival helped to ensure a calm and successful securing of the airway. While the stability of the situation may give the impression that there is abundant time, securing the airway in a timely fashion is of utmost importance given the possibility of rapid deterioration with penetrating neck trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the University of Louisville Institutional Review Board (IRB Number 23.0383).
Statement of Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article, and this was documented.
Data Availability
The authors had full access to all the information in this article. Deidentified data that support the findings of this study are available from the corresponding author, upon reasonable request.