
Abstract
Hemangioma is a frequently observed soft tissue tumor that can be classified into cavernous, capillary, and venous subtypes. It occurs frequently in the head and neck; however, with rare reports of hemangiomas in the external auditory canal (EAC). The present study describes the case of a 57-year-old male patient who presented to our center with a subsequent diagnosis of capillary hemangioma of the EAC. The entire lesion was surgically removed, with no evidence of recurrence on the subsequent follow-up.
Introduction
Hemangiomas are benign vascular tumors that usually involve the head and neck. According to the histopathological results, they can be categorized as capillary, venous, or cavernous hemangiomas. 1 Each subtype has specific characteristics; capillary hemangioma is identified by tightly coordinated capillary-like channels, whereas venous and cavernous hemangiomas consist of wide vascular spaces. 2 Few studies have reported hemangiomas involving the external auditory canal (EAC), with most cases presenting with hearing loss, aural fullness, and tinnitus.3-5 Here, we present a case report of a male patient with a diagnosis of capillary hemangioma of the EAC and review of the literature. This study was conducted in accordance with all relevant ethics standards. The presented data were anonymous and written informed consent was obtained from the patient.
Case Presentation
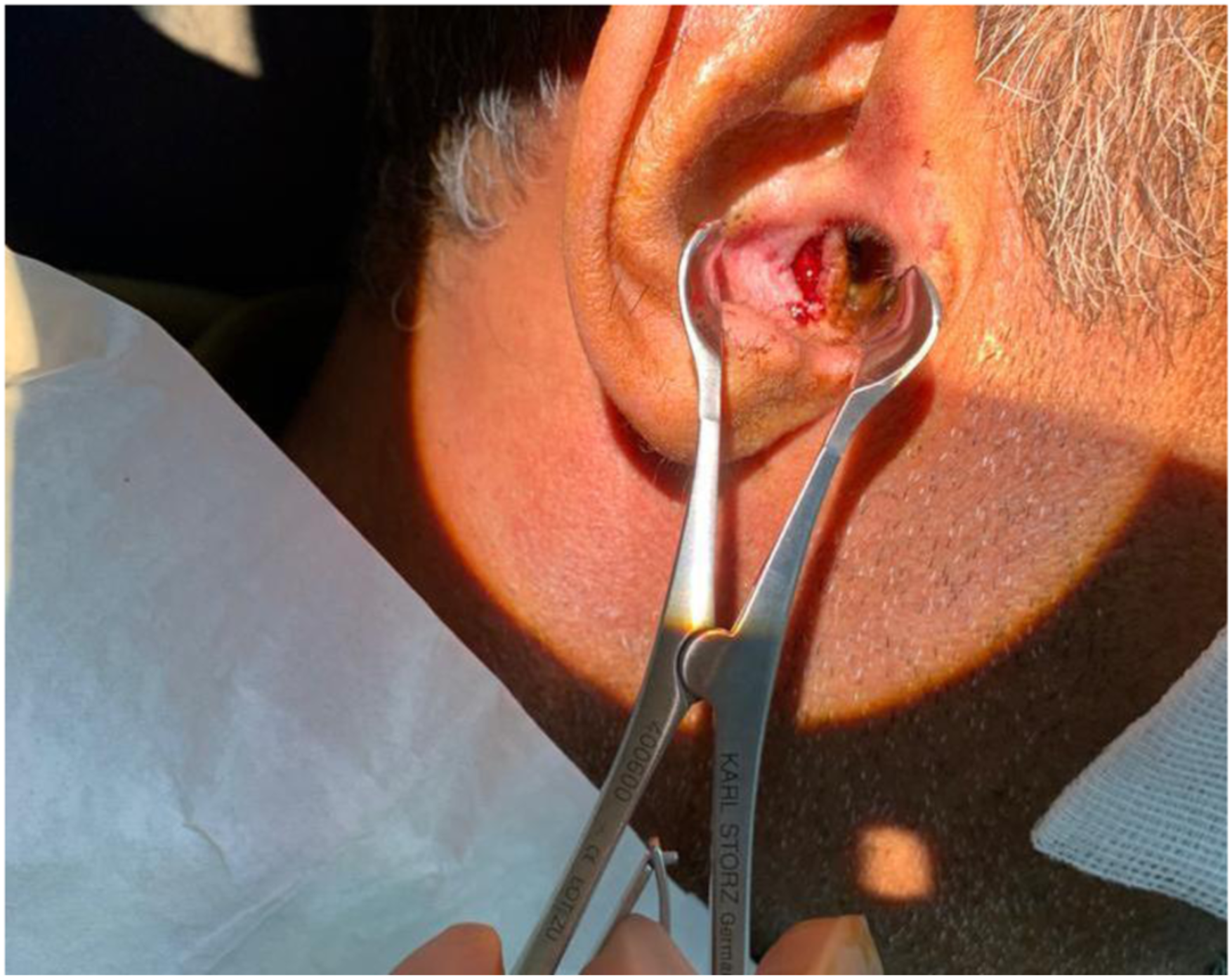
A 57-year-old male patient presented to our clinic for follow-up due to two-year history of a right concha mass. Notably, he reported no significant changes in size. The patient reported mild reduction in hearing, along with tinnitus, and pain. There was no history of trauma, ear surgery, or otorrhea, and the vital signs were within normal limits. Pure tone audiometry showed bilateral sloping to moderately severe sensorineural hearing loss (SNHL). Upon otoendoscopic examination, a bluish, well-circumscribed mass, approximately 0.8 mm, with an intact tympanic membrane was observed in the right ear (Figure 1), whereas the left ear was normal. A high-resolution computed tomography (CT) scan of the temporal bone revealed that the mass was confined to the EAC with no bony erosion or effect on the middle ear structures. Histopathological analysis of the surgically excised specimen revealed benign vascular proliferation, suggestive of capillary hemangioma; however, there was no evidence of malignancy. The entire mass was removed by surgery (Figure 2), with no evidence of recurrence at the later follow-up. A bluish, well-circumscribed mass within the external auditory canal (pre-excision). Post excision view of the mass.
Discussion
Hemangioma is a frequently observed soft tissue tumor that can be classified into cavernous, capillary, and venous subtypes. A literature search showed that hemangioma of EAC was rare. A random examination revealed that cavernous hemangioma is most frequently reported compared to capillary hemangioma.6,7 Notably, cavernous hemangiomas are often reported in adults, whereas capillary hemangiomas are more prevalent in infants. In addition, capillary hemangiomas develop in the dermis and may spontaneously regress while cavernous hemangiomas grow deeper. 6 Reviewing the literature also revealed that hemangiomas can be confined to the EAC, which is consistent with our findings.3-5 However, it can also involve other structures, including the tympanic membrane, middle ear cavity, and bone. 8 A study by Joshi and Wakode reported cavernous hemangioma involving the EAC, tympanic membrane, and bone. 9 Further, literature revealed that hemangioma of the EAC was not restricted to a particular side, and that lesions can involve both, the right4,5 and left ear.3,10 Further, the presenting symptoms of hemangioma of the EAC are inconsistent. Our patient experienced tinnitus and mild hearing loss at presentation; however, the lesion was asymptomatic for two years without increasing in size. Hearing loss, sensation of aural fullness, and tinnitus are common presenting features of EAC hemangiomas.3-5,10 Moreover, only a small mass was present in the EAC in a patient with lobular capillary hemangioma. 11 Another report revealed the presence of otalgia as the only complaint in a patient with cavernous hemangioma of the EAC. 12 Numerous lesions such as cholesteatoma, carcinoma, and glomus tumor can mimic hemangioma of the EAC, thus complicating the diagnosis. 5 Otoscopic examination may show a small sessile or pedunculated lesion in the anterior or posterior parts of the EAC. A literature search revealed that CT scan is a commonly helpful diagnostic approach in patients with capillary hemangioma of the EAC.3-5 A CT scan can assist in healthcare professionals in determining the extent of the lesion and probable bony erosion, in addition to guiding surgeons regarding an optimal surgical approach. 13 Furthermore, angiography may assist in recognizing feeding blood vessels of the hemangioma and aid in avoiding excessive bleeding. 13 However, histopathological studies are essential to confirm capillary hemangiomas and to exclude other differentials. Moreover, previous literature revealed that endaural, transcanal, or retroauricular surgical removal of EAC hemangioma is effective, with no recurrence.3-6,10,14 However, Jackson et al. reported the recurrence of the lesion following resection in a patient presenting with a mixed cavernous and capillary hemangioma of the EAC, tympanic membrane, and surrounding bone. 15 Thus, due to limited data, surgeons should consider re-evaluation of the lesion. Radiotherapy as a treatment option was described by Pavamani et al. for the management of capillary hemangioma of the EAC and middle ear; however, the size of the residual lesion remained unchanged, at the time of further follow-up. 8
Conclusion
This case report and review of the literature revealed that hemangioma of the EAC has rarely been reported in the literature, with cavernous hemangioma being the most common subtype. Hearing loss, sensation of aural fullness, and tinnitus are frequently accompanying presenting symptoms. Moreover, surgical removal of such lesions is an effective treatment strategy with good prognosis. However, subsequent follow-up is advised to investigate possible recurrence and bone erosion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Data Availability Statements
The information for this article are available online and completely open to the public.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.