
Abstract
Cavernous hemangiomas of the external auditory canal simultaneously affecting the tympanic membrane are extremely rare. Endoscopic otosurgery has been successfully used for resecting various ear lesions because of its wider surgical field of view and minimal trauma. We report the case of a 50-year-old male patient who presented with a 6-month history of left ear congestion. Otoendoscopic examination of the left ear revealed a dark red neoplasm blocking the bony external auditory canal. After admission, surgical contraindications were eliminated, and the patient underwent otoendoscopic resection of the canal tumor. Postoperatively, the patient’s symptoms were relieved, and there was no reoccurrence during the 1-month follow-up. The tumor was successfully removed using otoendoscopy, followed by tympanoplasty.
Introduction
Hemangiomas are a subtype of benign vascular tumors with an unclear etiology; however, some researchers have linked them to infections, trauma, medications, and hormonal changes. 1 They are common in the head and neck and are usually located in the skin or mucosal areas of the nasal cavity or sinuses. Based on histopathology, hemangiomas are divided into capillary, cavernous, and mixed types. Capillary hemangiomas are composed of abnormal tiny blood vessels arranged in a capillary-like pattern and are common in infants and young children. By contrast, cavernous hemangiomas are composed of vascular channels of various sizes lined by endothelial cells with large cavernous vascular spaces and are more common in older individuals. Cavernous hemangiomas in the external auditory canal are relatively rare, and those with simultaneous involvement of the tympanic membrane are even rarer.
Herein, we present a case of cavernous hemangioma of the external auditory canal involving the tympanic membrane. Furthermore, based on a review of the literature, we provide insights into the diagnosis and treatment of cavernous hemangioma of the external auditory canal.
Case Report
A 50-year-old male presented with a 6-month history of left ear congestion. Otoendoscopic examination of the left ear revealed a dark red neoplasm that blocked the bony external auditory canal (Figure 1A). Specialist examination revealed a soft, smooth, and painless tumor, without bleeding, and with no secretions on the surface. No abnormalities were observed in the right external auditory canal. The patient was healthy with no history of vertigo or ear trauma.
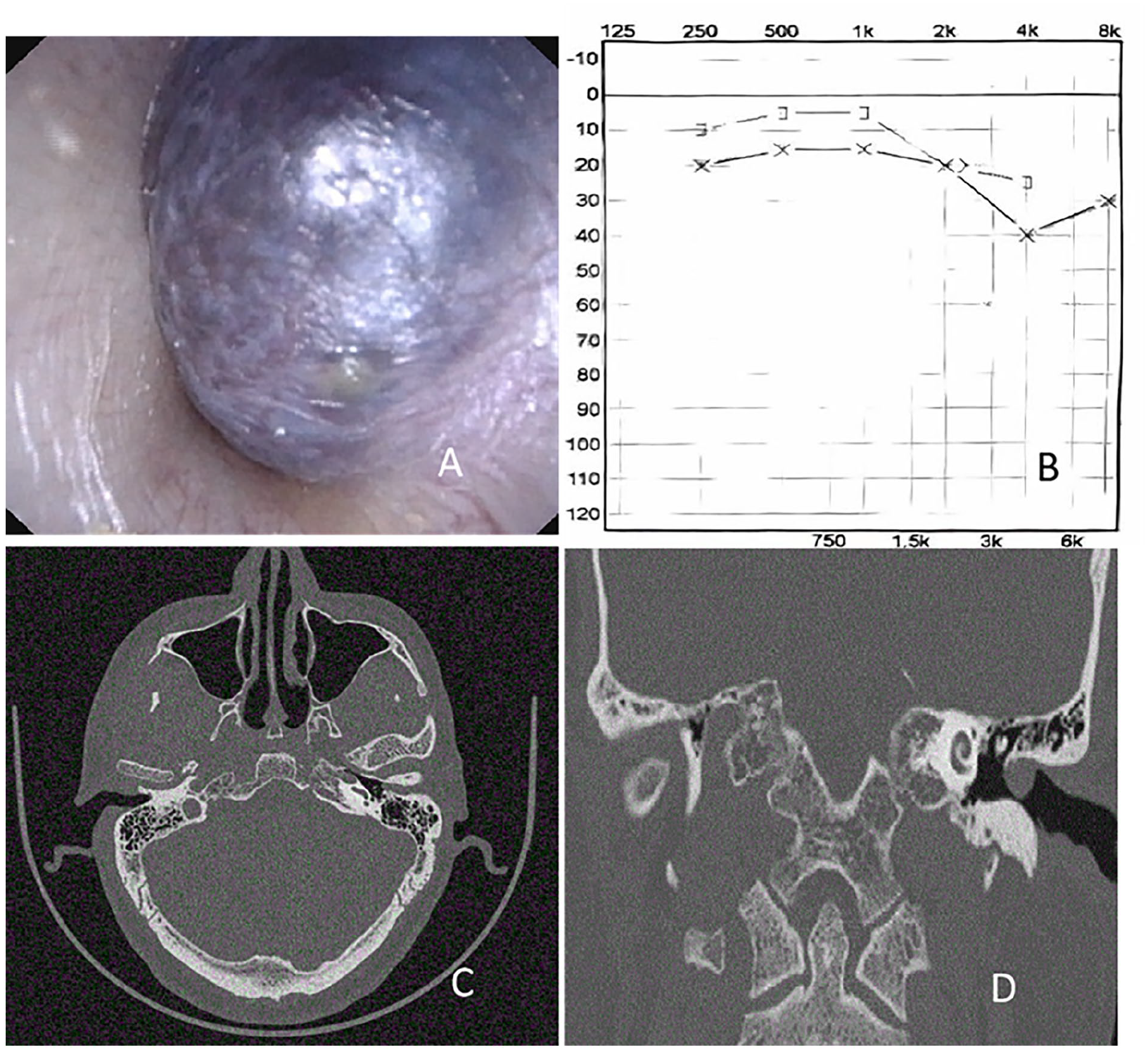
Otoendoscopy, audiometry, and CT images. (A) Otoendoscopy showed a dark red mass in the external auditory canal. (B) Hearing loss in the high-frequency region is detected in the left ear via audiometry. (C and D) Axial and coronal CT scans show soft tissue masses in the external auditory canal and near the tympanic cavity, with no involvement of the ossicles. CT, computed tomography.
Audiometry of the left ear revealed decreased hearing in the high-frequency range (Figure 1B).
Temporal bone computed tomography (CT) revealed obstruction of the left external auditory canal, with soft tissue density shadows and a CT value of approximately 60 HU. The lesion measured approximately 0.8 cm × 0.4 cm × 0.7 cm and involved the tympanic membrane but not the tympanic cavity (Figure 1C and D). Laboratory examinations revealed no abnormalities.
After admission, surgical contraindications were eliminated, and the patient underwent otoendoscopic resection of the left external auditory canal tumor, tympanic membrane repair, and auricular cartilage removal under general anesthesia. During the surgery, a dark red neoplasm that was soft to the touch was found deep in the left ear canal. The pedicle originated from the posterior, inferior, and superior walls of the ear canal. The deep ear canal and tympanic membrane were not fully visible during surgery. To reduce the tumor volume, a puncture needle was used to aspirate dark red liquid from the tumor. Then, the tumor in the ear canal was carefully re-examined and found to extend inward, reaching the posterior region of the tympanic membrane, and its deepest part was located in the handle of the malleus (Figure 2A). A small amount of epinephrine combined with 1% lidocaine was used for infiltration anesthesia in the ear canal. Subsequently, the skin of the ear canal was incised along a safe boundary around the tumor, and the skin flap was separated forward. The tumor was excised along its periphery. At the tympanic membrane, the tumor was mainly located in the epithelial layer and was completely removed. Following disinfection of the tragus, epinephrine and lidocaine were locally injected. A 0.2 cm circular incision was made inside the free edge of the tragus. A 1 × 1 cm perichondrium piece was taken from the tragus side. The perichondrium was trimmed and placed on the ear canal bone and the back and outside of the tympanic membrane. The ear canal was packed, the tragal incision was sutured, and sterile dressings were applied for fixation.
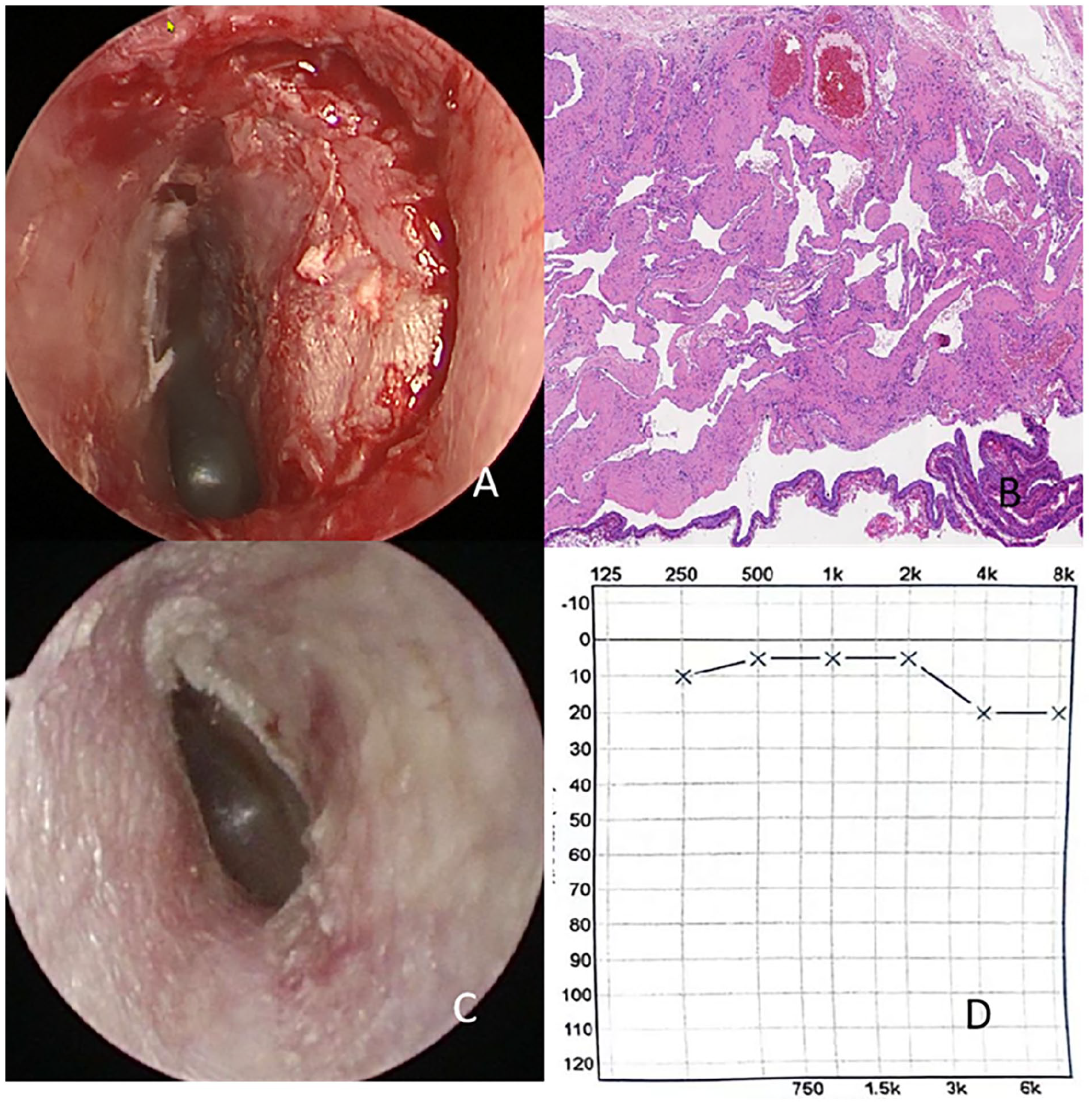
Intraoperative and postoperative otoscopy, tissue pathology, and postoperative hearing test images. (A) Otoscopy image of the tumor during surgery. (B) Histopathological image of the tumor. (C) Otoscopy 1 month after surgery showed good recovery. (D) Hearing test 1 month after surgery showed good recovery.
Histopathological examination showed that the vascular structures of the tumor were dilated, tortuous, and varied in size, tightly adherent to each other. The lumen was filled with red blood cells and lined with flat endothelial cells, consistent with the characteristics of a cavernous hemangioma (Figure 2B).
Postoperatively, the patient’s symptoms were relieved. At the 1-month follow-up, there was no reoccurrence (Figure 2C), and the hearing in the left ear was restored as confirmed by audiometry (Figure 2D).
Discussion
To the best of our knowledge, only 2 cases of cavernous hemangioma involving both the external auditory canal and the tympanic membrane2,3 and 1 case of mixed hemangioma (mixed capillary and cavernous hemangioma) 1 have been reported in the literature since 2000. This is the first reported case of cavernous hemangioma involving the external auditory canal and tympanic membrane in China.
Diagnosing cavernous hemangioma of the external auditory canal with simultaneous involvement of the tympanic membrane is based on clinical examination, otoscopy, diagnostic audiometry, imaging, and histopathological examination. Patients with cavernous hemangiomas of the external auditory canal may be asymptomatic or present with symptoms such as ear congestion, pulsatile tinnitus, ear fullness, and conductive hearing loss. In the present case, the patient presented with ear fullness, which disappeared after surgery. Cavernous hemangiomas of the external auditory canal are dark red or purple, soft to the touch, and exophytic. In most cases, temporal bone CT is sufficient for diagnosis and can be used to assess the extent, size, and presence of bone destruction by the lesion. However, in patients with lesions that invade the middle ear, MRI can reveal the nature, extent, and relationship between the lesion and the facial nerve. Pathologically, hemangioma manifests as dilated vascular sinuses ranging from capillaries to cavities, with the inner wall of the cavity lined with normal flat endothelial cells. A single layer of basement membrane is found under these endothelial cells. The lumen wall of the sinusoids has sparse smooth muscle cells, while the outer membrane exhibits fibrous degeneration.
Previous studies have shown that cavernous hemangiomas in the external auditory canal may continue to grow 4 ; therefore, most patients choose surgical treatment. The choice of surgical method is based on the size and location of the tumor and the degree of hearing loss. Small lesions can be removed using intraauricular and transauricular approaches, whereas for larger lesions, the ransmastoid or middle cranial fossa approach, or a combined approach, must be considered. In the previous cases, most external auditory canal hemangiomas were removed using the intraauricular or postauricular approach with a microscope. Magliulo et al 2 used a microscope to remove tumors via the intraauricular approach. Odat et al 3 removed a tumor by performing a canal wall mastoidectomy because the tumor had invaded the middle ear fissure. Jin and Kwak 4 for the first time used an ear endoscope to remove external auditory canal hemangioma lesions. Compared with the microscopic approach, ear endoscopes are being increasingly used because of their wider field of view, higher imaging quality, and minimally invasive nature. In our patient, the lesion was located deep in the ear canal, causing a blockage and obstructing the tympanic membrane. The lesion was limited, narrow, and difficult to operate on. According to the temporal bone CT scan, the lesion did not destroy the bone or enter the tympanic cavity. Therefore, we resected the lesion and repaired the tympanic membrane under a wide-angle field of view of an otoscope.
Early recurrence can be detected by close follow-up using an otoscope or imaging. According to a recent meta-analysis of external auditory canal hemangiomas, 5 most cases (31/38, 81.5%) did not recur, with a small number of cases 6 experiencing recurrences related to the extent of the initial lesion invasion. In the present case, no recurrence occurred during the 1-month follow-up, while hearing in the left ear was restored.
Conclusion
We presented a case of resection of an external auditory canal and tympanic membrane hemangioma followed by tympanic membrane repair using otoendoscopy. For the diagnosis of cavernous hemangiomas affecting both the external auditory canal and tympanic membrane, audiometry, CT, and tissue biopsy are essential. Treatment should be guided by the extent of the lesion, with the appropriate approach determined after adequate preoperative evaluation.
Footnotes
Author Contributions
Q.H. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis; Concept and design: H.Q., L.L., L.G., and Y.L.; Acquisition, analysis, or interpretation of data: all authors; Drafting of the manuscript: Q.H.; Critical revision of the manuscript for important intellectual content: Y.L.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This article was approved by the Ethics Committee of Liaocheng People’s Hospital ( LY2024110).
Informed Consent
Written informed consent was obtained from the patient.