
Abstract
Metastasis to the masticator space and mandible is very rare. The most common origin in women is breast cancer. Cystic metastases may radiologically mimic abscess. Definitive diagnosis can be made histopathologically. The prognosis of these patients is very poor and early diagnosis is important. Therefore, metastasis should be considered in the differential diagnosis of oral lesions.
A 55-year-old female patient presented to our otolaryngology clinic with trismus, diffuse swelling, and pain in her face and jaw. The patient had been diagnosed with breast cancer 5 years ago at an external center. She received radiotherapy and chemotherapy as treatment. On clinical examination, no significant mass was detected in the patient who could not open her mouth fully. Multiple hard, millimetric lymph nodes were palpated in bilateral cervical regions. Hemogram results were unremarkable. Contrast-enhanced computed tomography (CT) of the neck was performed because of possible inflammation and abscess. The images obtained showed multiple number and size of cystic lesions in bilateral masticatory space. These lesions showed intense contrast enhancement through their walls. Extensive periosteal reaction and density increases within the bone were noted in bilateral mandibular condyle and angulus. Cystic lesions of similar nature were also seen in bilateral cervical areas (Figure 1). Several lesions with peripheral edema, similar to the lesions in the neck, were seen in the brain sections within the imaging area. The primary differential diagnosis was abscess with metastasis, and histopathologic examination revealed a diagnosis of breast cancer metastasis. Chemotherapy was recommended and the patient voluntarily refused the treatment and left the hospital. The patient succumbed to the disease within 4 months. Contrast-enhanced axial (A) and coronal (B) CT images of the neck in the soft tissue window show bilateral masticatory cavity filling, centrally hypodense and peripherally contrasted lesions of multiple numbers and sizes (arrows). Cystic lymphadenopathies similar to these lesions are present in the cervical areas (red curve arrows). In the bone window axial images, diffuse sclerotic lesions and periosteal reaction in the mandible (asterisk) are remarkable.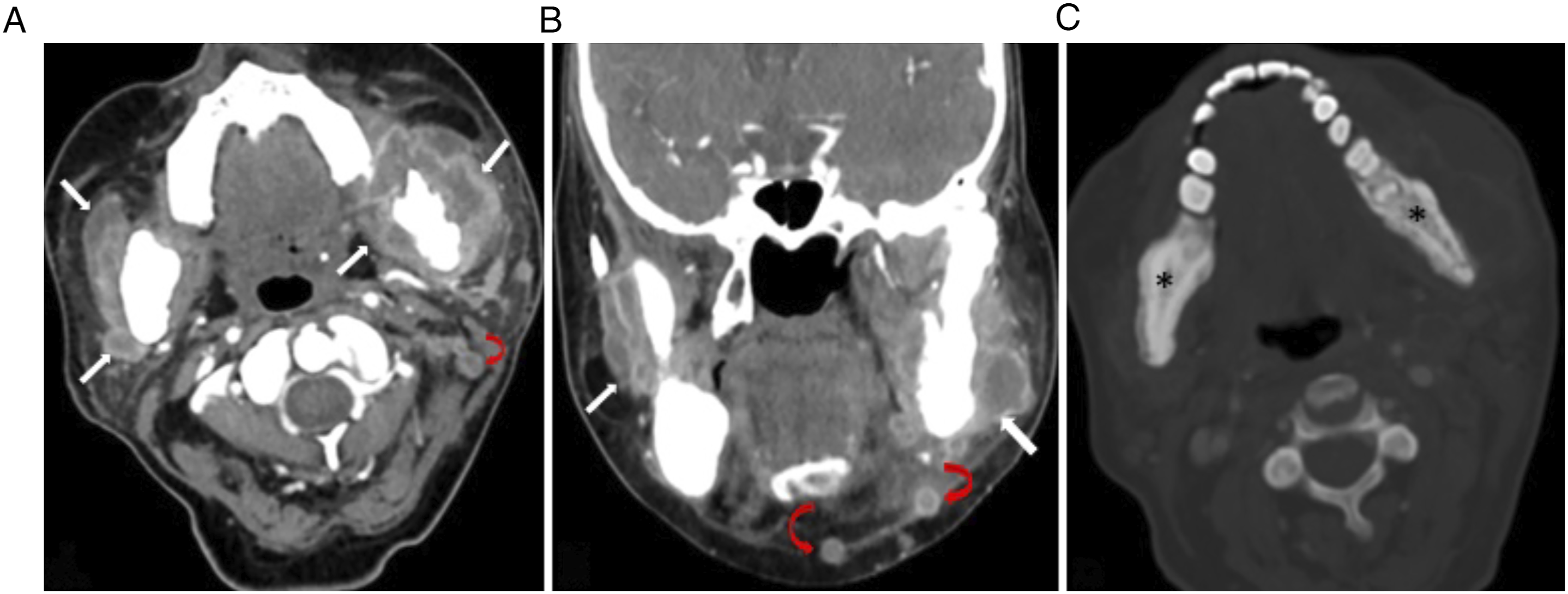
Matastasis to the oral region and jaw accounts for less than 1% of all oral malignancies. The most common origin of metastasis to the jaw is breast cancer in women and lung cancer in men. 1 The spread of metastasis occurs via lymphatic, blood, or both. The majority of oral cavity metastases of breast cancer are to the jaw bones, the mandible being the most common site (80–90%). Involvement of the molar and retromolar parts of the mandible that maintain hematopoetic function is common. Although patients are sometimes asymptomatic, the most common symptoms are paresthesia, trismus, pain, tooth loss, pathologic fracture, ulcerated, or bleeding mass in the lower lip and chin.2,3 Breast cancer can cause cystic metastases, especially to the brain. The appearance of these lesions on CT is similar to an abscess with central hypodense and peripheral dense contrast enhancement. The differential diagnosis of these lesions, which may show uptake on PET-CT, is definitively made by histopathology. Although surgery can be performed in local lesions, palliative treatment or chemotherapy is preferred.1-5
In conclusion, although masticator space metastases are rare, they are associated with poor prognosis and early diagnosis is important. As in this case, cystic metastases may mimic abscess and cause delayed diagnosis. Therefore, knowledge of the patient’s history and a multidisciplinary approach are very important when evaluating patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.