
Abstract
Metastasis to the nasopharynx is a rare clinical entity. Breast carcinoma is one of the primary tumors that can be responsible for a nasopharyngeal metastasis, which is an extremely rare occurrence. We report the case of a 50-year-old woman with a history of a confirmed breast carcinoma under chemotherapy who presented to our department with a unilateral hearing loss and tinnitus. Nasal endoscopy revealed a small bulging mass at the posterior wall of the nasopharynx. The biopsy of the lesion showed an infiltration of the nasopharyngeal mucosa by a mammary adenocarcinoma that was positive for estrogen and progesterone receptors and negative for human epidermal growth factor receptor 2. Computed tomography scan revealed a thickening of the nasopharyngeal mucosa, a pleural and pericardial effusion and diffused secondary bone lesions. The patient received chemotherapy. Control revealed a partial regression of the nasopharyngeal mass. The patient is still under chemotherapy.
Introduction
Nasopharyngeal tumors are dominated by squamous cell carcinomas. 1 Metastasis in the nasopharynx are rather a rare occurrence. 2 The reported primitive tumors spreading to the nasopharynx included breast, pulmonary, hepatocellular, renal cell, and colorectal carcinomas.3-5 The occurrence of a nasopharyngeal metastasis from a breast carcinoma is extremely rare. This report presents an unusual case of a breast adenocarcinoma spreading to the nasopharynx that presented with a unilateral tinnitus and hearing loss. The purpose of our paper is to determine the clinical features and the different management modalities of this rare entity based on our experience and on a review of the previously reported cases in the literature of a breast carcinoma spreading to the nasopharynx.
Case Report
A 50-year-old woman presented to our department with a history of a unilateral hearing loss and tinnitus. The patient had a medical history of a breast cancer diagnosed two years ago. She initially underwent a left total mastectomy associated to an ipsilateral axillary lymph node dissection. Histological examination revealed multiple foci of invasive ductal carcinoma of no special type, grade 3 according to the modified Bloom–Richardson–Elston grading system. Numerous images of lympho-vascular invasion were present. Five regional lymph nodes were involved. Immunohistochemical analysis revealed that the tumor cells were positive for estrogen receptors (ER) and progesterone receptors (PR) and negative for human epidermal growth factor receptor 2 (HER2). The Ki-67 index was 50%. According to the TNM staging system, the tumor was staged pT3 pN2b M0. The patient received adjuvant chemotherapy.
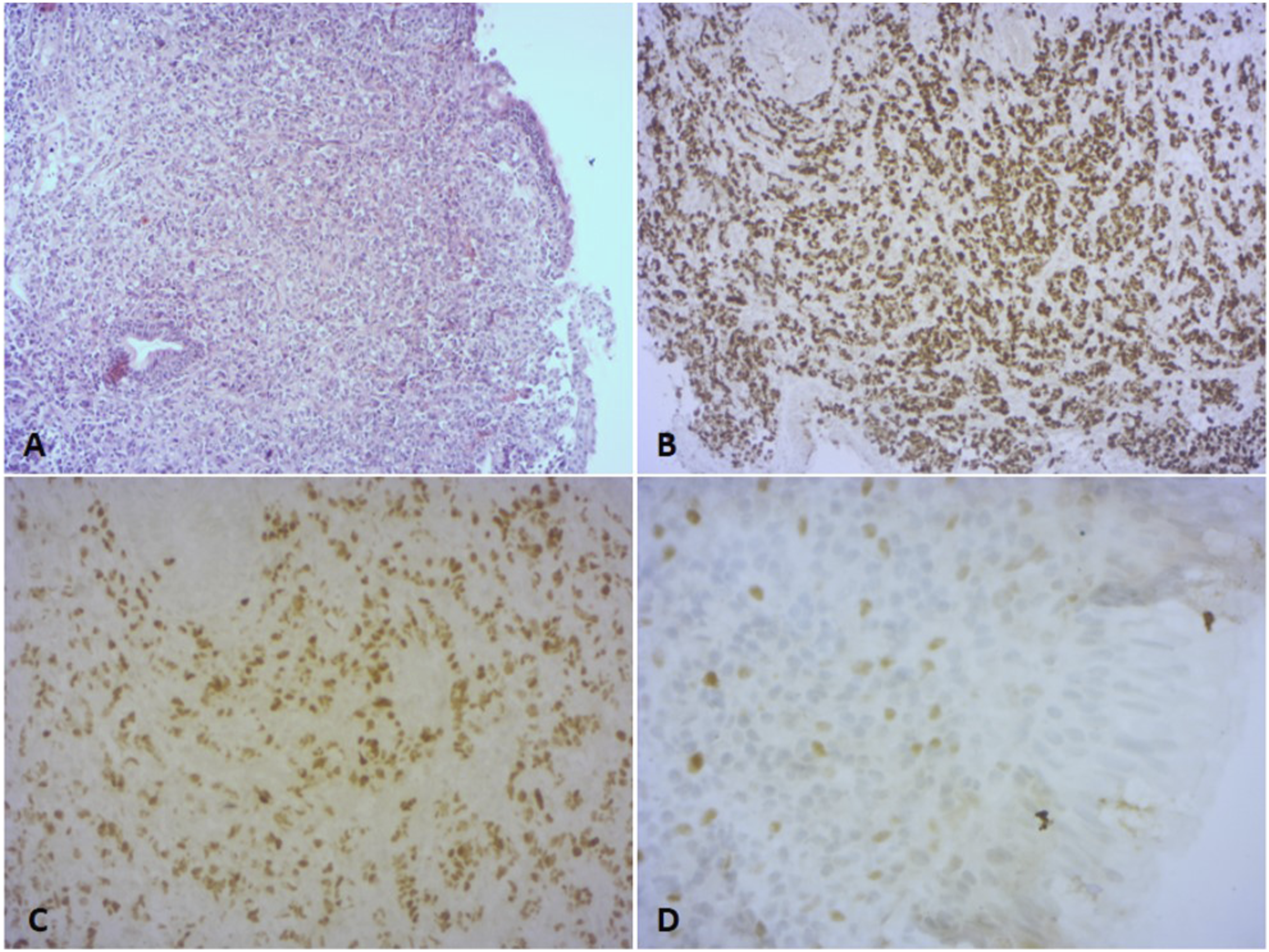
She presented to our otorhinolaryngology department with a recent left hearing loss, tinnitus and otalgia that had been evolving for few weeks. She reported neither nasal symptoms nor headaches. The patient was still under chemotherapy at presentation. Physical examination revealed a diminished transparence of the left tympanic membrane with a retrotympanic effusion. Nasal endoscopy revealed the presence of a small regular bulging mass at the left posterior wall of the nasopharynx that did not bleed at contact, without extension towards the Rosenmüller fossa (Figure 1). Pure-tone audiometry showed a right sensorineural hearing loss of 30 decibels and a left mixed hearing loss of 65 decibels. We performed a biopsy of the mentioned nasopharyngeal mass. Histopathological examination revealed an infiltration of the nasopharyngeal mucosa by tumor cells organized in diffuse sheets and glandular structures. The tumor cells were diffusely positive for GATA 3, which was in favor of their mammary origin. Immunohistochemical study was also positive for ER, PR and negative for HER2 and p63 (Figure 2). Nasal endoscopy revealing a small bulging mass at the left posterior wall of the nasopharynx (red arrow) not extending toward the Rosenmüller fossa. Infiltration of the nasopharyngeal mucosa by diffuse sheets of tumor cells (HEx100) (A) serial immunohistochemistry sections showing expression of GATA3 (B), Estrogen receptors (C) and Progesterone receptors (D) in tumor cells.
Computed tomography (CT) scan of the nasopharynx showed a thin and regular thickening of the nasopharyngeal mucosa. Thoracic, abdominal, and pelvic CT scan revealed a pleural and pericardial effusion and diffused secondary bone lesions. The patient completed the chemotherapy protocol she has been already receiving.
Control after 6 months revealed a total regression of the nasopharyngeal lesion with partial regression of the otalgia. The patient is still alive and under chemotherapy.
Discussion
Non keratinizing carcinoma is the most common subtype of nasopharyngeal carcinomas. 1 It mainly arises from the Rosenmüller fossa followed by the superior posterior wall. Multiple risk factors interfering with nasopharyngeal carcinomas were reported including an Epstein Bar Virus infection, a genetic predisposition and dietary and environmental factors.6,7 The nasopharynx is an uncommon site for metastases. The reported responsible primary tumors included breast, pulmonary, hepatocellular, and renal cell carcinomas.3,8 A case of a colorectal carcinoma spreading to the nasopharynx was recently reported. 5
A Summary of the Reported Cases in the English Literature of a Breast Carcinoma Associated to a Nasopharyngeal Metastasis.
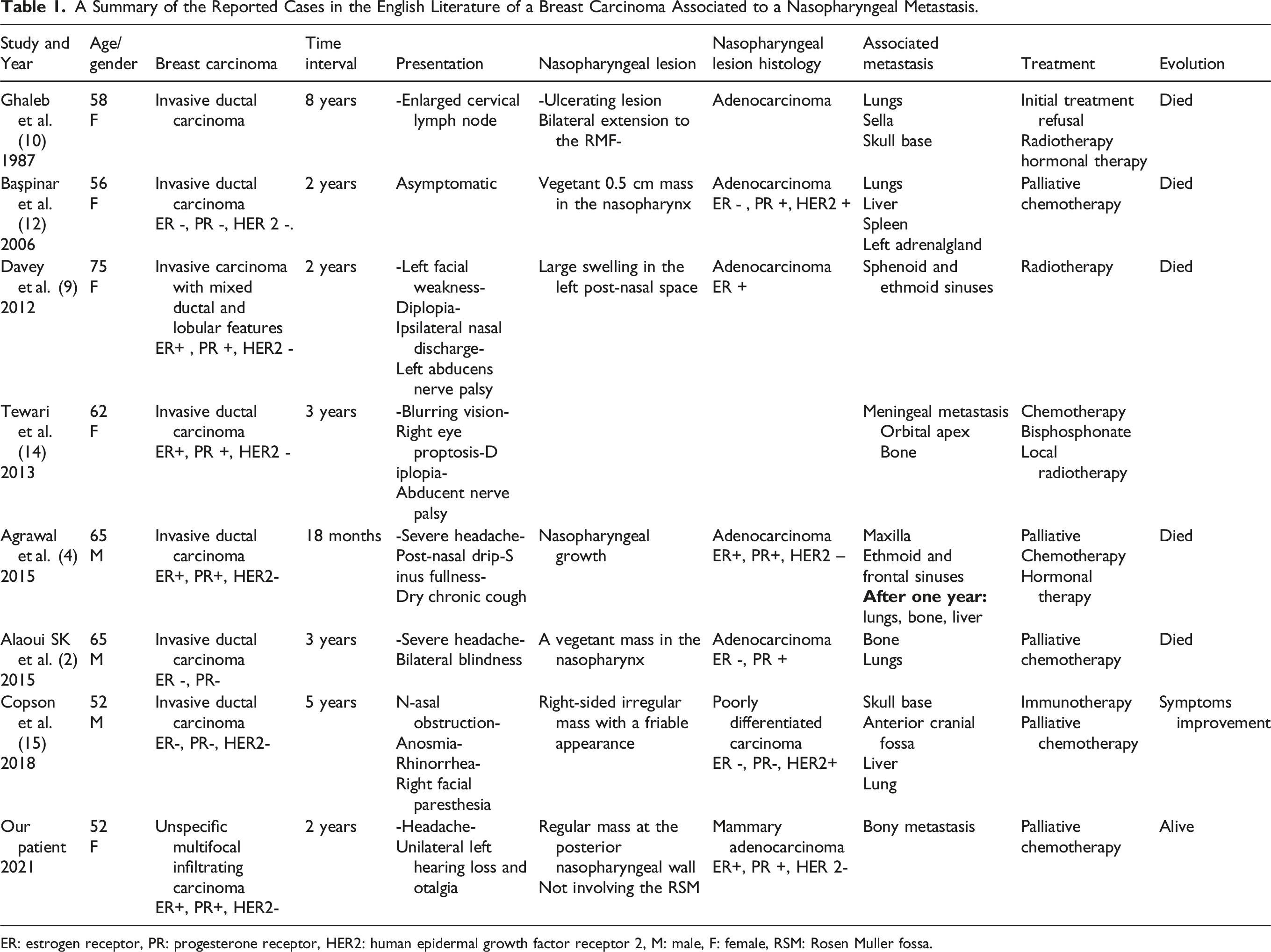
ER: estrogen receptor, PR: progesterone receptor, HER2: human epidermal growth factor receptor 2, M: male, F: female, RSM: Rosen Muller fossa.
The presentation of this condition was variable in the literature. All reported cases belonged to patients with an already confirmed breast carcinoma who consulted during the disease’s progression with varying symptoms suggesting a nasopharyngeal mass. (Table 1) The timing between the diagnosis of the breast cancer and the initial manifestation of the nasopharyngeal metastasis varied between 18 months and 8 years. Our patient presented with a unilateral otalgia and hearing loss that appeared during the progression of a confirmed mammary carcinoma. In the case reported by Ghaleb et al., 10 breast cancer nasopharyngeal metastasis rather manifested with an enlarged jugular-digastric lymph node. In fact, the manifestations of either a primary or secondary nasopharyngeal carcinoma depend on their location and extension to adjunct structures. They typically present with a unilateral nasal obstruction, ipsilateral epistaxis, nasal discharge, and hearing loss.3,9 Other associated symptoms are related to the spread to the skull base and to cranial nerves; they can include, headache, diplopia, abducens nerve palsy, facial pain, and dysphonia. 9
In the case of suggestive symptoms, a thorough examination of the nasopharynx is required especially in the case of a progressive extra-nasopharyngeal primary carcinoma. Secondary nasopharyngeal lesions can be located in the submucosa making their diagnosis harder. 9 Multiple biopsies were required in the case reported by Davey et al. 9 to make the diagnosis. Since a metastasis in the nasopharynx especially from breast cancer occurs seldom, differentiating between a primary and a secondary nasopharyngeal carcinoma is a challenging task; and its association to a histologically confirmed primary tumor is not sufficient to make the diagnosis of a nasopharyngeal metastasis. 11 A history of a breast cancer, the reported symptoms, a thorough histopathological examination of the nasopharyngeal lesion, a histological resemblance with the primary tumor alongside with a high index of suspicion are important to make the diagnosis.2,3,9 Immunohistochemical study is necessary to determine the etiology of metastatic lesions as the expression of GATA3, ER, and PR strongly pleads in favor of a mammary carcinoma.2,12,13 The immunohistochemical profile of the metastasis was either identical to the primary tumor or rather different. In our patient, hormonal receptors and HER2 status were similar between the primary breast carcinoma and the nasopharyngeal metastasis, while the consistency of these status was variable in the reported cases.
Computed tomography scan is the best imaging modality to evaluate the bony extension of a nasopharyngeal carcinoma. Magnetic resonance imaging (MRI) is superior to detect the extension to surrounding and distant soft tissue and to the base of the crane as well as intracranial extension.6 18F-fluorodeoxyglucose (18F-FDG) PET CT scan has also been widely used for the staging and the management of nasopharyngeal carcinoma especially to detect distant metastasis, small cervical lymph nodes, and both local residual and recurrent disease.6,14
Metastasis of a breast cancer to the head and neck are usually associated with other metastatic lesions and to an advanced stage of the disease leading to a poor prognosis.13,15 In the literature, nasopharyngeal metastasis originating from a breast carcinoma was associated to other metastatic sites in six patients while it preceded lung metastasis appearance in one patient. Davey et al. 9 suggested to stage isolated nasopharyngeal metastasis from a breast carcinoma as a primary nasopharyngeal cancer. Management of this rare condition was variable between different studies. It depended on the hormonal and HER2 status of the tumor, the local tumor extension and the presence of other metastatic lesions. However, due to the limited reported cases, there are no guidelines for their management. Their treatment remains non-consensual and case-dependent. It is based on radiotherapy, chemotherapy, immunotherapy and hormonal therapy. A multidisciplinary team approach is required for the therapeutic decision.2,9 Early recognition and treatment of the metastatic stage of the disease and the nasopharyngeal metastasis specifically is important to improve the outcome of this condition. 15
Conclusion
We reported a case of a breast cancer spreading to the nasopharynx which is an extremely rare clinical entity. Its diagnosis depends on the clinical presentation. A thorough clinical and histological examination with a high index of suspicion is needed to make an early diagnosis. Immunohistochemical analysis can help make the diagnosis. Early recognition of the metastatic disease is important. Management of these cases remains not consensual and requires a multidisciplinary team approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series since we anonymously reported clinical and imaging information concerning our patient’s case. A written informed consent was obtained from our patient for her anonymized information to be published in this article.
Informed Consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.