
Abstract
The objective of our study is to assess the impact of equivocal or positive positron emission tomography combined with low-dose noncontrast computed tomography (PET/CT) findings in the chest on treatment for head and neck cancer (HNC). We reviewed charts of patients presented at Augusta University’s Head and Neck Tumor Board (AUTB) between 2013 and 2016 with the following exclusion criteria: <18 years, Veterans Affairs patients, those with incomplete data, and those without a history of head and neck squamous cell carcinoma. The lung/thorax sections of the radiologists’ PET/CT reports were graded as “Positive, Equivocal, or Negative” for chest metastases. Patients who underwent workup for suspected chest metastases were assessed for treatment delays, changes in treatment plans, and complications. In addition, we evaluated the time between AUTB presentation and peri-treatment PET/CT to primary treatment initiation were calculated between groups. There was a total of 363 patients with PET/CT prior to treatment, the read was “Negative” in 71.3% (n = 259), “Equivocal” in 20.9% (n = 76), and “Positive” in 5.8% (n = 21). Of 272 patients with complete treatment data, 22 underwent workup for suspected chest metastases. Mean time from PET/CT to treatment initiation was 27.5 days without workup and 64.9 days with workup (P < .0001), and from AUTB presentation was 29.1 days without workup and 62.5 days with workup (P < .0001). Five (19.2%) patients experienced a complication from workup. Twenty (76.9%) patients had no changes in their treatment plan after workup. In conclusion, our results for potential chest metastases on PET/CT in patients with HNC are often not clear-cut. Workup of suspected chest metastasis based on PET/CT findings significantly delays primary treatment initiation and may cause serious complications.
Introduction
In the United States, head and neck malignancies account for 3.7% of all cancers, with approximately 63 000 Americans developing head and neck cancer (HNC) yearly and 13 000 dying from the disease. 1 Imaging is invaluable in evaluating primary tumors and in the detection of regional and distant metastases. Contrast-enhanced computed tomography (CT) or magnetic resonance imaging for evaluation of the primary and cervical lymph nodes, and chest CT or X-ray have been used most commonly for staging of head and neck squamous cell carcinoma (HNSCC). However, fluorodeoxyglucose (FDG) positron emission tomography combined with low-dose noncontrast CT (PET/CT) has become the preferred modality for the staging of head and neck malignancies by many practitioners due to the ability to simultaneously stage the primary, neck, and body with the added information about metabolic activity. 2 The PET/CT has a reported sensitivity of 91% to 98% and specificity of 92% to 93% for HNSCC. 3 –5 Its use has important implications for staging, prognostication, and development of treatment plans. 6,7
According to the 2017 National Comprehensive Cancer Network guidelines, indications for PET/CT in HNC include initial staging for stage III and IV disease, workup of occult primary tumors, and posttreatment surveillance. 8 Positron emission tomography/CT is useful in stage III and IV disease to assess for distant metastases or secondary primary tumors and for this purpose demonstrated a sensitivity of 89% (95% confidence interval [CI]: 0.83-0.93) and specificity of 95% (95% CI: 0.94-0.96) in a previous meta-analysis. 9 Moreover, previous studies have shown treatment plans to be altered in up to 13.7% to 30% of patients who undergo initial PET/CT imaging. 2,10 Routine utilization of PET/CT has become the mainstay of practice in pretreatment staging in locoregionally advanced (stage III/IV) HNC. 11,12 Nonetheless, PET/CT can be overwhelmed by false positives and indeterminate results and is insensitive in the evaluation of patients with glandular tumors, and those with low-volume tumors and cystic metastases. 13
The incidence of distant metastases at initial presentation of HNSCC varies from 1.5% to 16.8% and is significantly higher for stage III and IV disease. 14 –17 The presence of distant metastasis often changes the goal of treatment and typically precludes surgery as a treatment modality. Of those found to have distant metastasis, chest metastasis account for 66% to 80%. 18,19 Xi et al performed a meta-analysis evaluating PET/CT’s ability to diagnose lung malignancy in patients with HNSCC and found a sensitivity of 85% and specificity of 98%. 20 Other studies have found results of PET/CT in evaluating distant metastases are often equivocal. Radiologists use different parameters in reporting potential lesions, which is especially apparent for chest metastases. 2,10 Increased FDG uptake in the lungs or mediastinal lymph nodes can be difficult to interpret due to the high prevalence of infection and inflammation within the chest. 21 This may be especially common in patients with HNC as the prevalence of dysphagia and chronic aspiration is very high. Equivocal results put providers in a difficult position to decide which patient should proceed with a workup of a potential chest metastasis. This workup is often invasive and due to scheduling factors and recovery time likely leads to a delay in treatment initiation. Time from initial diagnosis to primary treatment initiation has been shown to be clinically significant in patients with HNC. A delay of greater than 46 to 52 days introduces an increased risk of death and is consistently detrimental beyond 60 days. 22
The primary aim of this study is to assess the impact of equivocal or positive PET/CT findings in the chest on treatment for patients with HNC.
Patients and Methods
After obtaining approval from the institutional review board of Augusta University, the names and medical records of all new patients presented at Augusta University’s Multidisciplinary Head and Neck Tumor Board (AUTB) between January 1, 2013, and December 31, 2016, were collected with the respective dates each patient was presented. These were compiled together in an encrypted Excel (Microsoft, Redmond, Washington) spreadsheet. Patients treated primarily at the Charlie Norwood Veterans Affairs Medical Center, patients less than 18 years old, and patients with incomplete or inaccessible AUTB records were excluded.
Data collected included age at AUTB presentation, sex, diagnosis, TNM staging, the presence of a PET/CT scan before primary treatment of their tumor, date of AUTB presentation, modality of primary treatment, and date patients began their primary treatment. Patients who did not have PET/CT prior to treatment were excluded. The thorax and lung sections of the radiologists’ reports of the PET/CT scans were read and graded as either “Positive, Equivocal, or Negative” depending on language used to assess for the presence of chest metastases. The dates of the PET/CT scans were recorded. It was noted if a patient had a workup with pulmonology, thoracic surgery, cardiothoracic surgery, or interventional radiology performed image-guided biopsies for potential chest metastases. Patients who underwent workup for suspected chest metastases were evaluated in terms of pathology results from biopsy, changes in proposed treatment plan, and complications of workup. Finally, the date which all patients began their primary treatment were recorded. Days between AUTB presentation and primary treatment initiation were calculated as well as days between peri-treatment PET/CT and initiation of primary treatment. Unpaired t tests (GraphPad, La Jolla, California) were used to assess for statistical significance.
Results
There were 842 new patients presented at the AUTB from January 1, 2013, to December 31, 2016, with 558 patients meeting inclusion criteria and 284 patients excluded: VA patient (n = 72), less than 18 years old (n = 1), incomplete AUTB records (n = 45), and nonsquamous cell carcinoma histology (n = 166). Of the 558 patients, 363 had a PET/CT prior to initiation of primary treatment, 195 patients did not have a PET/CT prior to treatment and were excluded. Two hundred seventy-two included patients had complete treatment data, whereas 91 patients were excluded from treatment initiation analysis due to incomplete data in regard to date of treatment initiation or patients who failed to undergo treatment (see Figure 1).
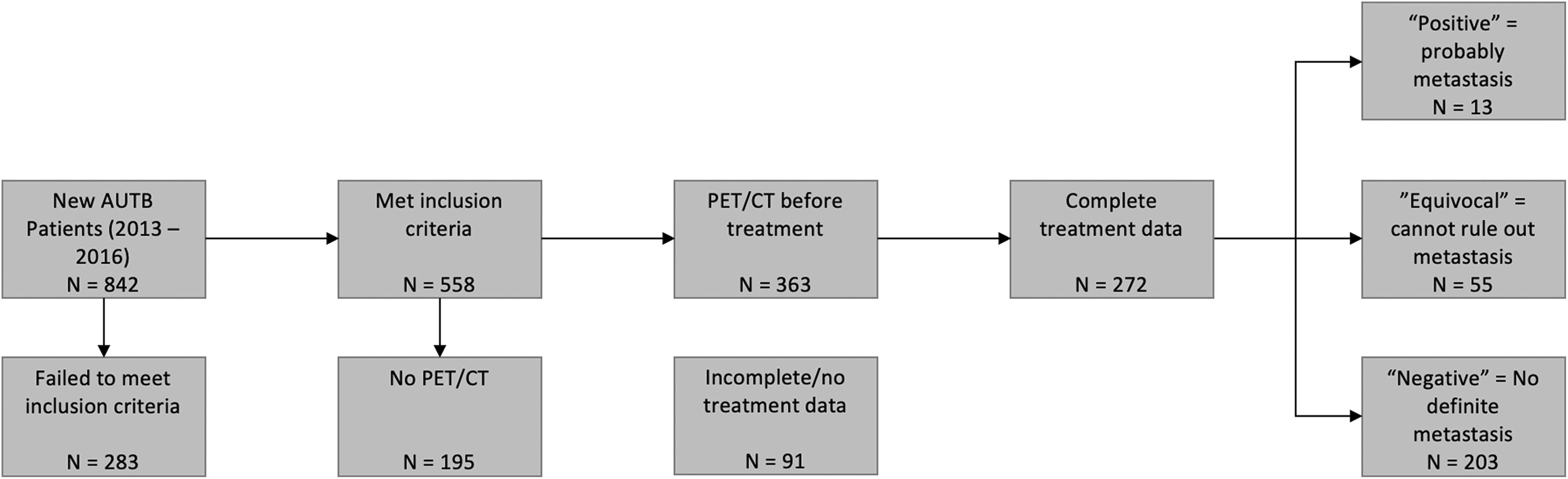
Flow chart demonstrating work flow to achieve final pool of patients from which the results are derived. AUTB indicates Augusta University Tumor Board; PET/CT, positron emission tomography/computed tomography.
The average age at AUTB presentation among the 363 patients with PET/CT scans performed was 62.3 years. There was a male to female ratio of 3.5:1. The neoplasm anatomic locations of these patients were noted to be 32.8% (n = 119) at the oropharynx, 26.5% (n = 96) oral cavity; these represent the 2 most common locations; the full distribution is demonstrated in Figure 2. The recommended or patient selected primary treatment modalities are shown in Figure 3; surgery was the most common recommendation at 48.6% (n = 175) followed by concurrent chemoradiation therapy at 34.1% (n = 123). Three hundred fifty-seven patients had available PET/CT reports. Of these patients, the read on the lung/thorax report was graded “Negative” in 71.4% (n = 259), “Equivocal” in 20.9% (n = 76), and “Positive” in 5.8% (n = 21). Two hundred seventy-two patients within this group had detailed treatment data available in their medical records. Among those without workup for chest metastases (n = 250), the mean time from PET/CT scan and AUTB presentation to treatment initiation was 27.5 (median = 20.5; interquartile range [IQR] = 27.3) and 29.1 (median = 20; IQR = 22.5) days, respectively. Among those with complete records who underwent a workup for possible chest metastases (n = 22), mean time from PET/CT and AUTB presentation to treatment initiation was 64.9 (median = 50; IQR = 53.3) and 62.5 days (median = 50.5; IQR = 47.3), respectively. The difference in time to treatment initiation between the 2 groups was statistically significant for time from PET/CT to treatment (P < .0001, 95% CI: 26.0-49.0) and for time from AUTB presentation to treatment (P < .0001, 95% CI: 25.3-46.0; see Table 1).
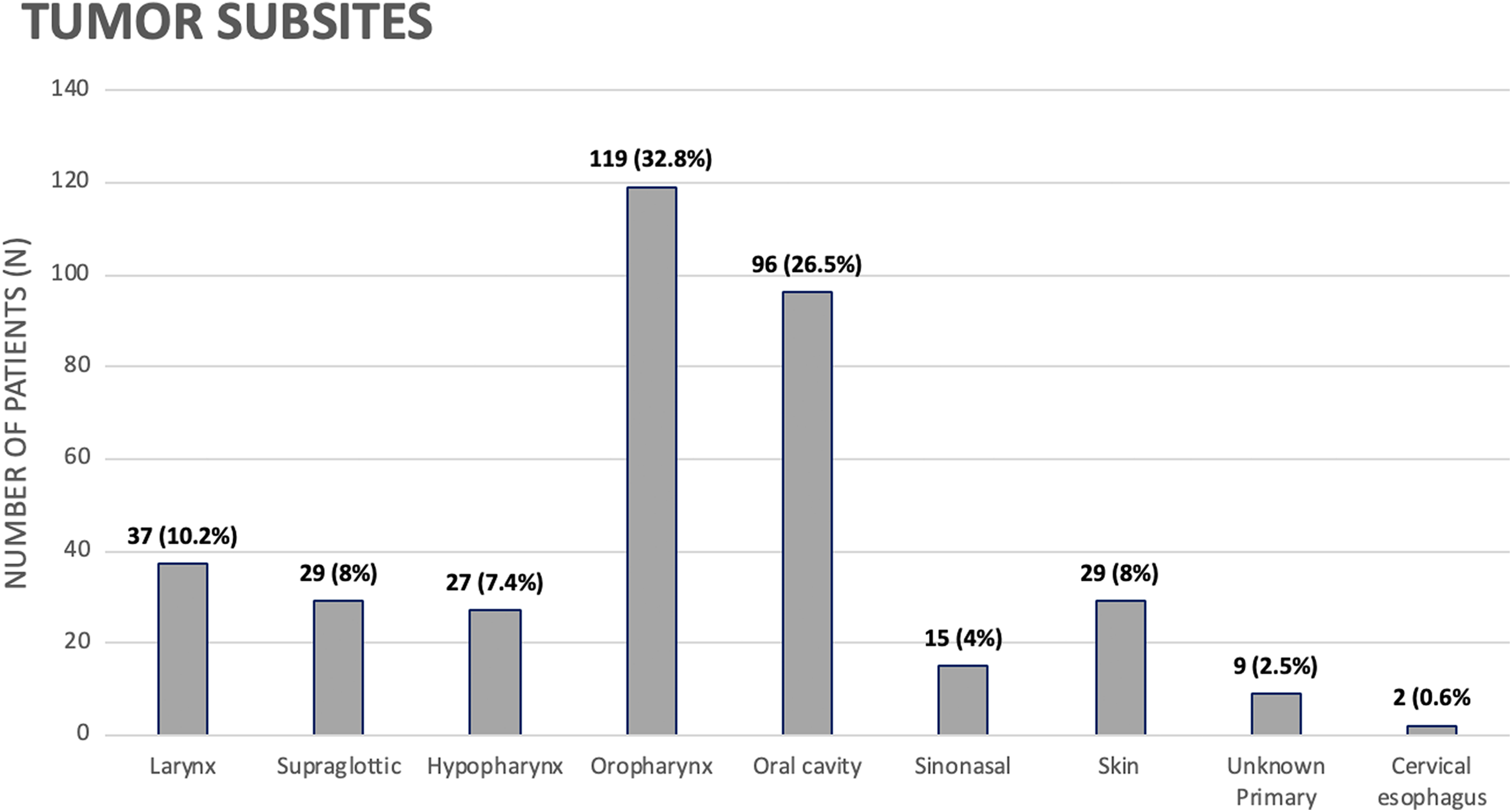
Breakdown of neoplasm subsite of the 363 patients presented at AUTB that had PET/CT scans in the peri-presentation period. AUTB indicates Augusta University Tumor Board; PET/CT, positron emission tomography/computed tomography; SCCA, squamous cell carcinoma.
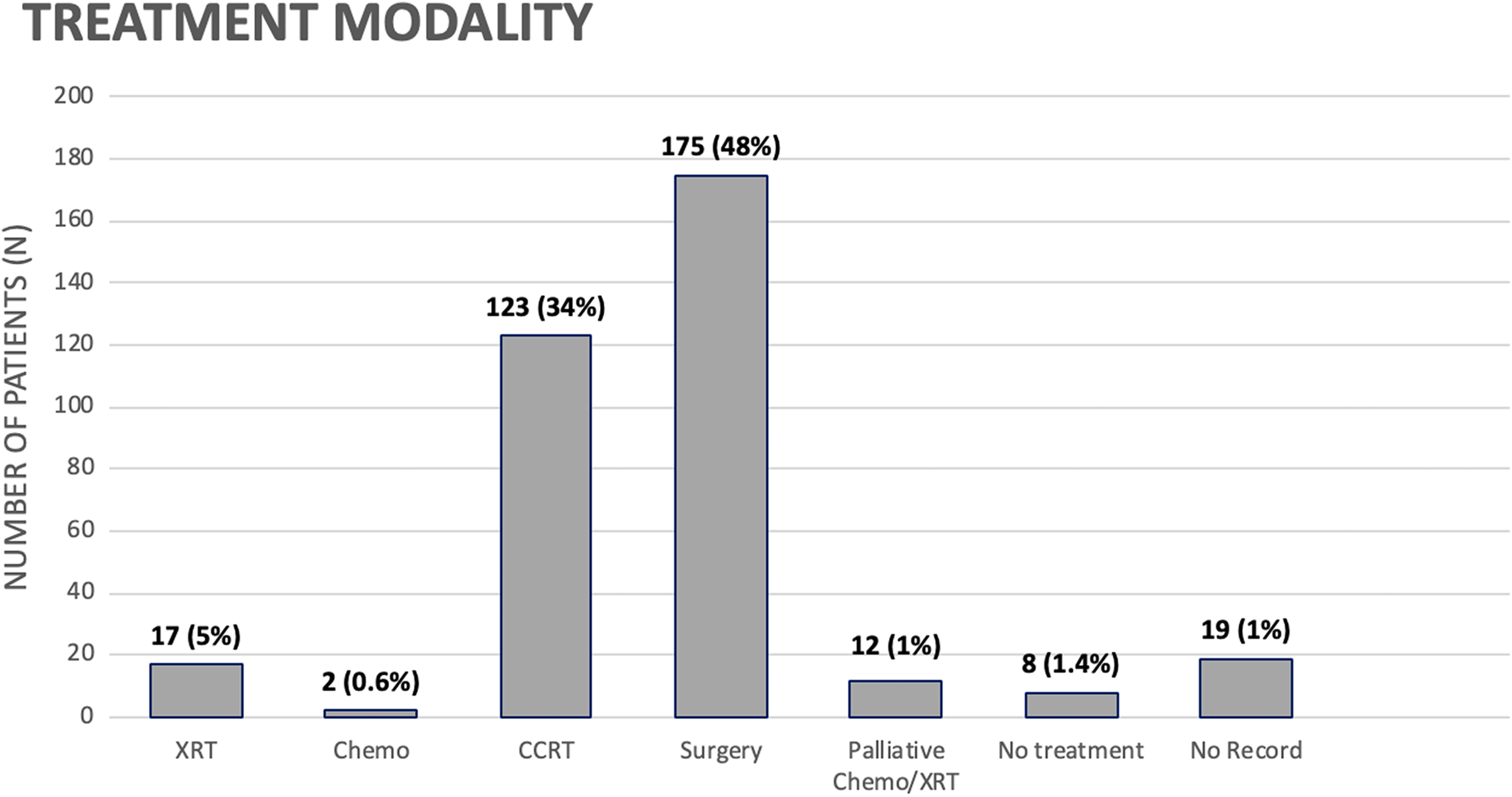
Distribution of recommended treatment modality bestowed by the AUTB on the 363 patients with PET/CT scans in the peri-presentation period. AUTB indicates Augusta University Tumor Board; chemo, chemotherapy; PET/CT, positron emission tomography/computed tomography; XRT, radiation therapy.
Time in Days to Treatment Initiation in Patients With and Without Workup for Suspected Metastases After PET/CT Imaging.
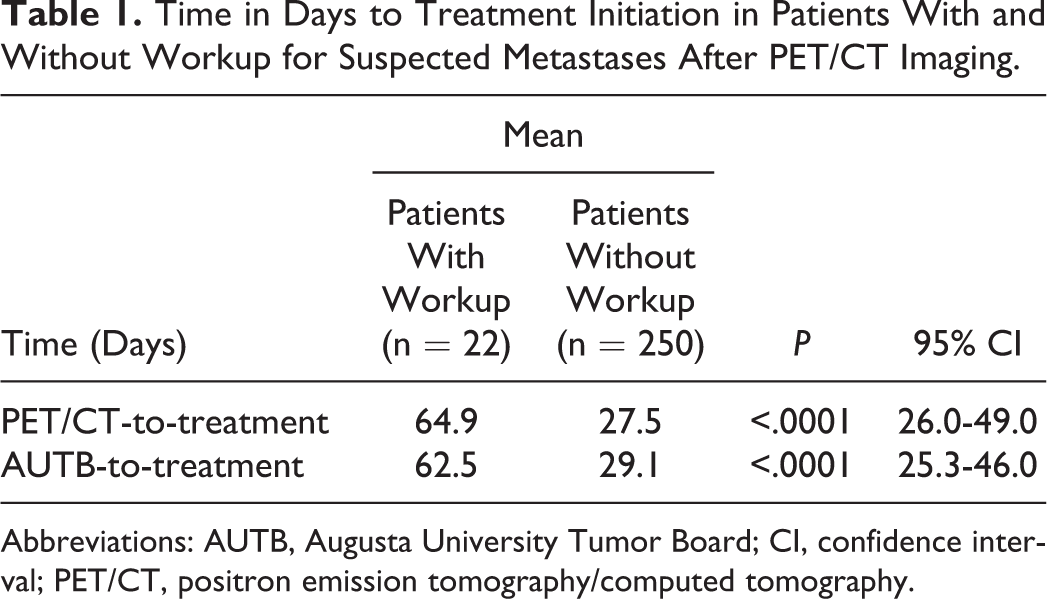
Abbreviations: AUTB, Augusta University Tumor Board; CI, confidence interval; PET/CT, positron emission tomography/computed tomography.
Workup of suspected chest metastases included consultation to pulmonology, thoracic surgery, cardiothoracic surgery, or interventional radiology. The consultant then proceeded with endobronchial ultrasound with biopsy, CT-guided biopsy, or mediastinoscopy with biopsy +/− wedge resection. Of the 21 patients with a PET/CT report graded as “Positive” to chest metastasis, 9 (42.9%) underwent workup and were biopsied, with 8 (38.1%) confirmed malignant, 1 (4.8%) indeterminate, and 1 (4.8%) benign. Of the 76 patients graded “Equivocal”, 16 (21.1%) underwent workup, 13 (17.1%) biopsied, with 6 (7.9%) confirmed malignant lesions, 6 (7.9%) benign, and 1 (1.3%) biopsies reported as indeterminate. One patient graded “Negative” underwent workup and biopsy which was benign (see Table 2). Of the 26 patients who underwent a biopsy, there were 5 (19.2%) complications reported. Four patients developed a pneumothorax after the procedure while in the intensive care unit (ICU) or on the surgical floor, all requiring placement of a chest tube (not placed at time of procedure). Two patients required an additional 2 inpatient hospital days, and 2 patients had an additional 3-day hospital stay. One patient died after video-assisted thoracoscopic surgery (VATS) with wedge resection after a prolonged intubation and developing ventilator-associated pneumonia.
Qualitative Radiology Read of Lung and Thorax on PET/CT With Workup and Biopsy Results
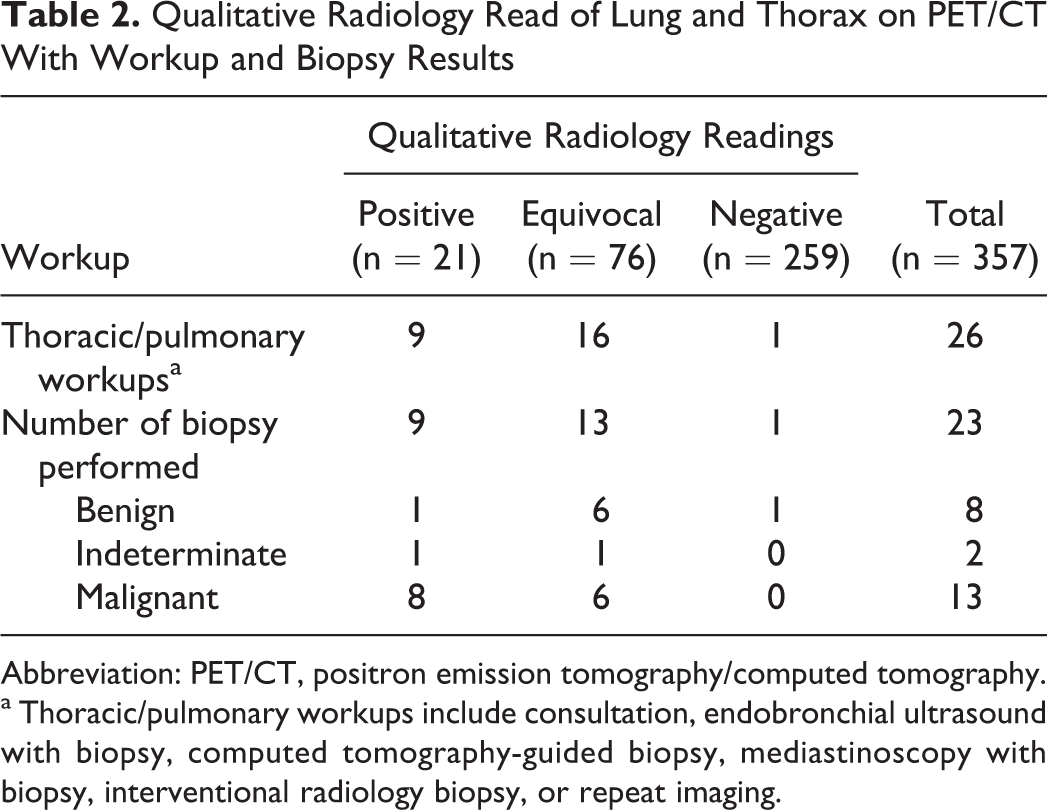
Abbreviation: PET/CT, positron emission tomography/computed tomography.
a Thoracic/pulmonary workups include consultation, endobronchial ultrasound with biopsy, computed tomography-guided biopsy, mediastinoscopy with biopsy, interventional radiology biopsy, or repeat imaging.
Twenty (76.9%) patients who underwent a workup had no changes in their primary treatment. Of the 6 with changes in treatment modality: 1 patient was found to have a second primary, 4 had confirmed chest metastases changing their treatment plan to palliative chemotherapy or palliative radiation therapy, and 1 patient died before treatment could be initiated. See Table 3 for details regarding changes in treatment modalities.
Breakdown of Changes in Primary Treatment Modality After Workup for Chest Metastases.
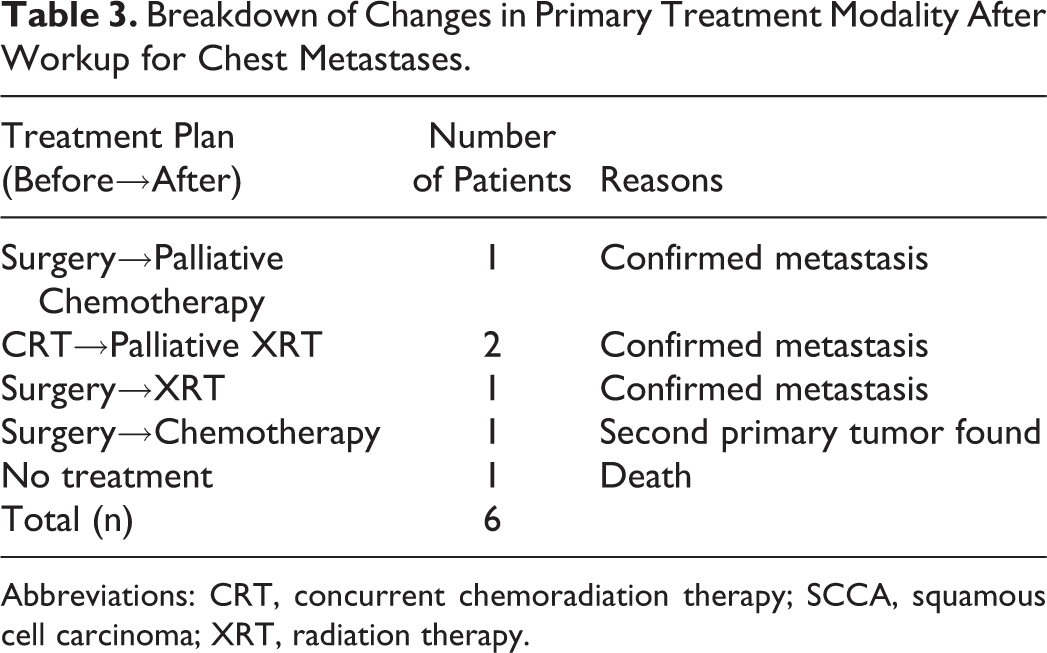
Abbreviations: CRT, concurrent chemoradiation therapy; SCCA, squamous cell carcinoma; XRT, radiation therapy.
Discussion
Positron emission tomography/CT was interpreted as equivocal in 20.9% of HNC reads at our institution. These equivocal findings may be due to subjective interpretation, scanning parameters, or other benign conditions in the lungs. Most PET/CTs are interpreted in a qualitative manner, which is a risk factor for subjective interpretation. 20 Different scanning parameters, such as patient preparation, blood glucose level, timing of imaging taken, and FDG dose, have also been shown to affect the accuracy of PET/CT. 20 In assessing the lungs, granulomatous, infective, and inflammatory processes of the lung can increase uptake of 18FDG, mimicking malignant nodules. 23 These equivocal findings often place the treatment team in a predicament of deciding when and/or if further workup should be pursued and may also lead to additional stress for patients. 24 Currently, there is no consensus as to which patient with equivocal findings should undergo further workup and biopsy versus follow-up imaging examinations. Of the 76 patients in this study with equivocal chest PET/CT finding, 16 (21.1%) patients underwent thoracic surgery or pulmonary workup, and only 6 (7.9%) patients were proven to have malignant neoplasia. The PET/CT findings for these patients with confirmed malignancy showed standardized uptake values (SUV) of lung nodules and/or chest lymph nodes from minimally active to 4.5 with some patients having single lesions versus others with multiple potential metastases. There were no clearly distinguishing features on PET/CT between those with negative and positive workup.
In current practice, there is a consensus that PET/CT is an appropriate tool in the initial staging of patients with advanced HNC suspicious of distant metastases and/or synchronous secondary tumors. 25 However, PET/CT is not indicated for stage I/II disease, where the likelihood of distant metastasis is much lower. 13 In this study, 33 PET/CT scans (9.1% of total PET/CTs in this study) were obtained on patients with stage I/II disease with 3 (9.1%) equivocal scans and 30 (90.9%) negative scans. The majority of these PET/CTs were ordered by providers practicing in the community before patients were referred to our academic medical center. None of the patients who had early-stage disease underwent further workup for distant metastasis based on the results of their PET/CT.
Time to primary treatment initiation was an average of 27.5 days from PET/CT and 29.1 days from AUTB presentation. This study showed a significant delay in treatment initiation in those who underwent workup for suspected chest metastases of 64.9 days from PET/CT and 62.5 days from AUTB presentation. Multiple studies have been conducted to investigate the effect of treatment delays in HNC. Significant signs of tumor progression were evident in most patients within an average of 28 days with a mean increase of 38% in tumor volume. 26 However, prognosis was not altered if delay was less than 40 days. Fortin et al found that treatment delay greater than 40 days is associated with increased risk of compromised control of local and neck disease and worsening survival rates in patients with early-stage (T1-2, N0-1) disease. 27 Murphy et al showed that patients with a delay in treatment of greater than 46 to 52 days have an increased risk of mortality that is greatest in patients with early-stage disease. 22 In contrast to stage I/II disease, the effect of delay of primary treatment on overall survival rate in locoregionally advanced patients with HNC is more controversial. Caudell et al showed there was no significant difference in overall survival rates between stage III/IV patients with a treatment delay less than or greater than 34 days. 28 On the contrary, an analytic cohort of 51,665 patients with HNSCC showed that treatment delay of 61 to 90 days and of greater than 90 days significantly predicted higher risk of death compared with treatment delay of less than 30 days (hazard ratios: 1.13 and 1.29, respectively). 22 Another study demonstrated that treatment delay was associated with a worse prognosis only in stage IV, but not in stage I, II, and III patients. 29 However, tumor growth leads to more extensive treatment and potentially increased morbidity and health-care expenses. 30 These increased morbidity and mortality risks incurred to workup potential chest metastases in our cohort do not outweigh the potential benefit. Rarely did the proposed treatment modality change from chest workup.
The decision to biopsy lung lesions should be made with consideration of the risk of complications from biopsy, probability of malignancy in these nodules, as well as the effect of delay in primary treatment. In this study, 26 patients underwent workup for suspicious pulmonary lesions with a total of 5 (19.2%) patients experiencing complications from the workup. Pneumothoraces occurred in 4 (15.4%) patients postprocedure, all of which required a chest tube placement while on the surgical floor or ICU. Unfortunately, 1 patient postoperatively was unable to be weaned from mechanical ventilation, acquired pneumonia, and died after a VATS/wedge resection. The malignancy rate of these pulmonary nodules was 56.5% (13 malignancy confirmed of 23 biopsies) and a nondiagnostic rate of 8.7% (2 biopsies). The complication and malignancy rates associated with lung workup in this study are in accordance with the results demonstrated by other studies. 31,32
The additional treatment delay in patients who underwent a workup was due in part to prolonged hospital courses and associated hospital deconditioning. Twenty-seven percent of patients who underwent workup had at least a 2-day hospital stay, and several patients were admitted for 5 days post procedure. Prolonged recumbency during the hospital stay is associated with acceleration of hospital deconditioning, deterioration of nutritional status, and prolonged recovery time, which further delayed receiving primary treatment for HNC. 33 Twenty (76.9%) patients with a workup for suspected chest metastases had no change in their clinical management based on their workup. Of the entire cohort, only 1.4% of patients with PET/CT for pretreatment staging prior to presentation had a change in management due to workup for potential chest metastases. One patient was found to have a second primary changing treatment from surgery to concurrent chemoradiation. Three patients had their treatment changed from either concurrent chemoradiation or surgery to palliative chemotherapy or palliative radiation. One patient had surgery canceled for primary radiation once metastasis was confirmed and another patient with confirmed metastasis still had surgery with the recommendation to add postoperative chemoradiation due to the confirmed lung metastasis.
In summary, at our institution, there was a low risk (7.9%) of metastatic disease when PET/CT was read as “equivocal,” below the traditional threshold of 15% to 20% used for elective neck dissection, and workup was associated with an average time to treatment initiation of more than 60 days. Given the risks and low likelihood of altering treatment plans, the decision to pursue further workup of suspicious pulmonary lesions in patients with HNC should only be made after the treatment team and patients have considered the risks of associated complications, the diagnostic value of the workup, and the possible detrimental effects of delaying primary treatment.
Our study was the first to investigate the treatment delay and outcome associated with pulmonary workup in patients with equivocal or positive pulmonary lesions on staging PET/CT. There are a few limitations to our study. First, due to the retrospective nature of this study, we were unable to identify how the decision in tumor board was made to further workup suspected chest metastasis for certain patients with equivocal and positive PET/CT. We did not look at specific demographic and comorbid factors which may have also contributed to the extended treatment delay and/or complications in patients who underwent a pulmonary workup, as this was outside the scope of the current study. Patients whose primary treatment included radiation therapy likely had delays due to the need for dental extractions. Patient social issues and scheduling factors may have contributed to treatment delays and are unable to be assessed given the retrospective design. However, it is unlikely these disruptions would be clustered in any one subgroup of our cohort.
In the future, it would be helpful to assess the overall survival rate and morbidity in this patient population to further identify the effect of delaying primary treatment. Future studies should work to identify specific parameters that warrant workup of equivocal lesions on PET/CT to establish a protocol to guide head and neck surgeons when to pursue workup versus when to follow with serial imaging.
Conclusion
Positron emission tomography/CT is a valuable tool in the management of patients with HNC; however, results for potential chest metastases are often not clear-cut. Workup of suspected chest metastases based on PET/CT findings significantly delays primary treatment initiation and may cause serious, and even deadly, complications. It is rare that workup of equivocal or positive PET/CT findings leads to changes in treatment plans, typically in the case that metastatic disease is confirmed. We have shown that the likelihood of confirming metastatic disease in cases of equivocal PET/CT interpretation is not particularly high. This finding should be carefully considered by the multidisciplinary team at each institution and used as part of the decision-making process regarding the necessity and timing of chest workup.
Footnotes
Authors’ Note
This article was a poster presented at the 2016 AAO-HNSF Annual Meeting and OTO EXPO; September 18-21, 2016; San Diego, CA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.