
Abstract
Objectives
We have attempted to characterize the clinical presentations and management of infratemporal fossa abscesses with the goal of improving awareness and promoting earlier diagnosis and treatment for this rare condition.
Methods
an extensive systematic search was performed through Pubmed/Medline, CINAHL (EBSCOhost), and Web of Science. Two authors screened out studies by abstracts, and a third resolved any conflicts. The remaining studies were assessed by full-text assessment, leaving 43 studies for data extraction.
Results
sixty-seven patients were included from the final 43 studies. The patients were predominantly male (56.7%), and the average age of patients was 44.3 years (standard deviation (SD) 19.8 years). Risk factors most commonly odontogenic, whether the etiology was through tooth extraction (n = 30, 44.8%) or infection (n = 17, 25.4%). Symptoms on presentation included pain (n = 40, 83.3%), swelling (n = 39, 81.3%), and trismus (n = 36, 75.0%). Twenty-two (32.8%) patients were managed with intraoral incision and drainage (I&D), 18 (26.9%) with extraoral I&D. After treatment, 45 of the 48 (93.8%) patients from the case reports and series were deemed to have achieved complete resolution.
Conclusions
Infratemporal fossa abscesses are rare, but they may be associated with serious neurologic and systemic complications. Although prompt diagnosis paramount in avoiding these sequelae, patients often experienced delays in diagnosis. Surgical drainage and extended antibiotic therapy is recommended.
Introduction
The infratemporal fossa (IF) is an uncommon site for abscess development, with previously reported etiologies including odontogenic or sinonasal infections. 1 Odontogenic causes of infratemporal abscesses (IFA) arise secondarily to poor dental health or recent dental procedures and have been posited to ascend to the mandible or maxilla and erode through cortical bone and periosteum. 2 Furthermore, bacteria may be seeded from injections of local anesthesia, directly contaminating the IF during mandibular nerve block. Sinonasal causes of IFA are more commonly associated with prior maxillary sinus fractures and sinusitis. 3 It has been suggested that defects arising from fracture or erosion secondary to infection in the posterior maxillary wall provide direct microbial access to the IF.
With the advent of antibiotic therapy and childhood vaccinations, deep neck space infections have become an increasingly rare phenomenon in the modern era. 4 The literature pertaining to IFA is scant and has primarily been characterized by case reports or case series. The lack of familiarity with IFA may lead to delays in diagnosis and treatment. 5,6 This becomes significant since the complications of untreated infections may lead to serious consequences including cranial nerve involvement, intracranial complications, and extension into adjacent deep neck spaces including the retropharyngeal space. 7 The objective for the present study is to develop a more complete characterization of the following 5 domains: 1) general characteristics, 2) risk factors, 3) assessment and diagnosis, 4) microbiology and antibiotics, and 5) treatment and outcomes. This is the first systematic review of previously published IFA cases.
Methods
Author K.Y performed an extensive systematic search through Pubmed/Medline, CINAHL (EBSCOhost), and Web of science on September 2021. Several terms, including infratemporal, infratemporal abscess, masticator space, and abscess were utilized in these queries. The complete methodology used in the database search are more completely characterized in Figure 1 and Appendix A. The list of studies was subsequently cleaned for duplicates using the reference management software Rayyan QCRI. Authors K.Y and A.W separately reviewed all the studies identified by the initial database search, screening for relevance by article titles and abstracts. Author D.T subsequently reviewed all conflicts and finalized their resolutions. The included studies underwent a full-text assessment by the primary author before qualifying to be part of the systematic review. Inclusion criteria were that the article was either a case report, case series, or retrospective review with individual case data and that the patient must have been diagnosed with infratemporal abscess or have had imaging of an abscess involving the infratemporal space. Additionally, all non-English manuscripts were excluded if their English abstracts did not provide information on baseline demographics, clinical presentation, and management. The primary author pulled data including study ID (author names and publication year), patient demographics (age and gender), medical history (precipitating factors, microbiology, diagnosing specialty, delays from acute symptom onset, or dental procedure to diagnosis (months), method of definitive diagnosis, disease management (surgery or antibiotics), duration of post-operative antibiotic therapy, outcomes, and complications (hearing loss or cranial nerve involvement). A standardized abstraction form was negotiated by all authors prior to data extraction. The authors adhered to PRISMA guidelines for this systematic review. We calculated means and standard deviations for continuous variables and frequencies for categorical variables. PRISMA Flow Diagram for Search and Review Strategy.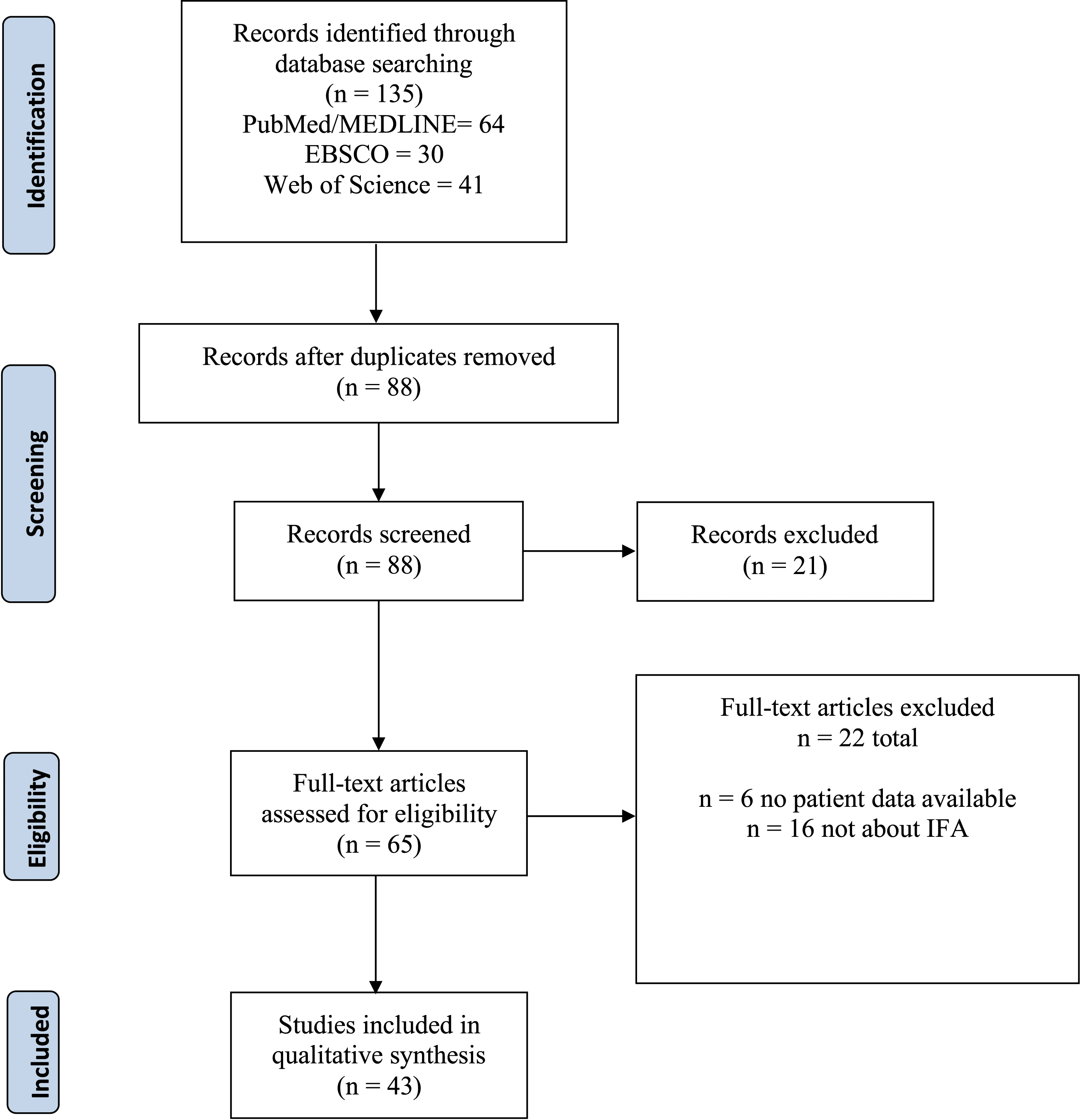
Results
The initial database search yielded 135 titles and was subsequently narrowed to 65 after the abstract screening process. Of these remaining studies, 22 studies were found to be ineligible by full-text assessment. 43 articles were included in this systematic review, with 67 corresponding cases of IFA. There were 48 patients that were featured in case reports or series and 19 patients that were pulled from a retrospective review. Studies involving the masticator space but outside the boundaries of the infratemporal fossa were excluded. 8 -12
Quality Appraisal
The overall quality of cases was deemed moderate to high, as is demonstrated in Appendix B. There were data available regarding patient demographics, risk factors, imaging modalities, and surgery type performed for 67/67 of cases. Additionally, after removing the 19 cases from the retrospective review, the majority of cases reported information regarding presenting symptoms (47/48), microbiology (32/48), antibiotic usage (45/48), and resolution (45/48).
General Characteristics
Demographic and Baseline Information.
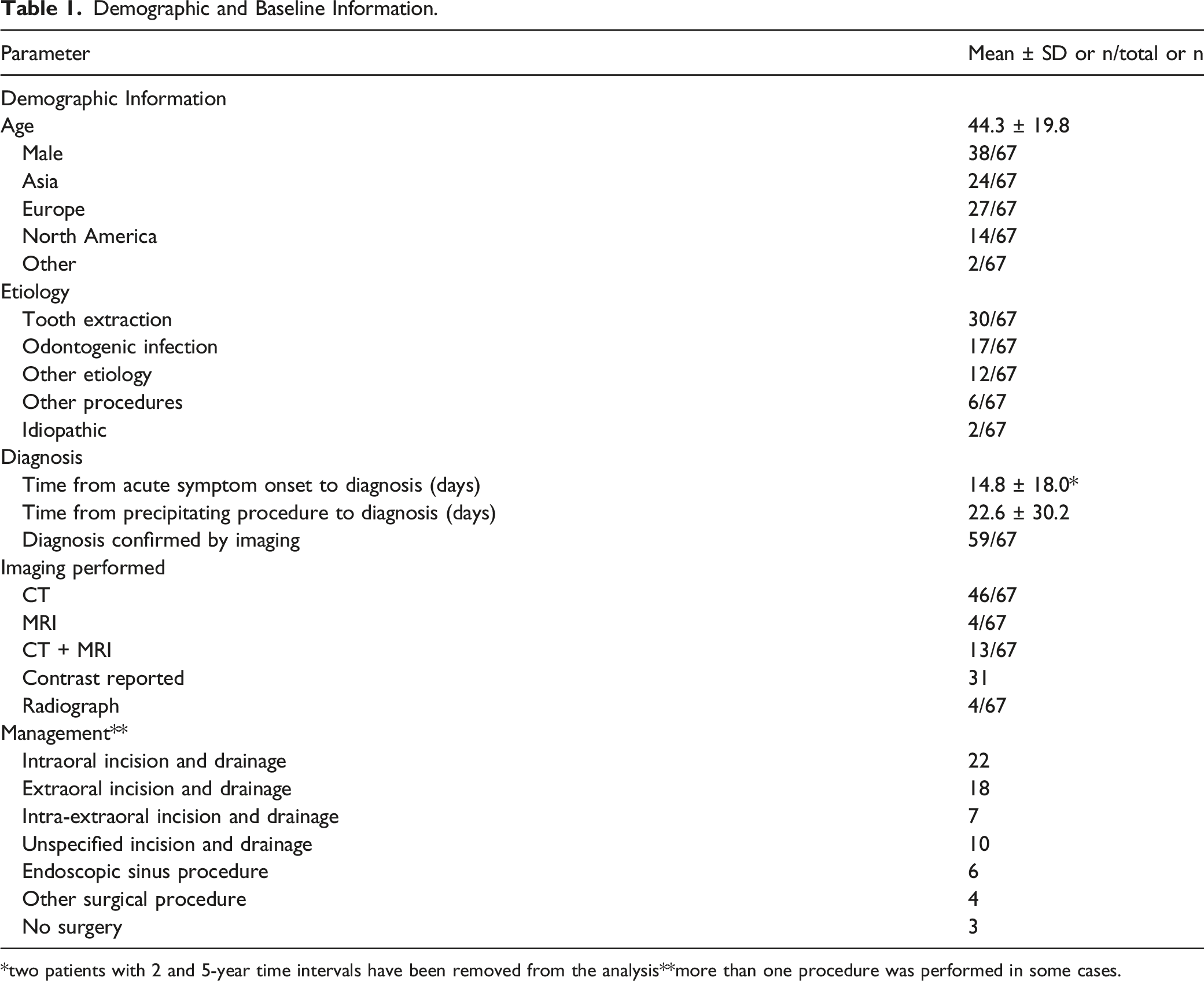
*two patients with 2 and 5-year time intervals have been removed from the analysis**more than one procedure was performed in some cases.
The average age for our patients was 44.3 years (standard deviation (SD) 19.8 years). The majority of our patients were male (38/67). The studies were most often conducted in Europe (27/67), Asia (24/67), or North America (14/67). Additionally, two patients from Australia and Brazil were included in this analysis.
Risk Factors
The most common etiologies behind IFAs were secondary to tooth extractions (n = 30/67) and odontogenic infections (17/67). Extractions were specified to be primarily left-sided in 16 procedures, in contrast to being right-sided in 12 or bilateral in 1 procedure. Fifteen teeth were noted to be removed from the maxilla, and 12 and 2 were extracted from the mandible or both the maxilla and mandible, respectively. Finally, 27 of the tooth extractions involved one or more molars. The third molars (n = 18), or wisdom teeth, were extracted at a higher frequency than the first (n = 4) or second molars (n = 5).
There were 3 cases each that reported etiologies pertaining to sinus infection or trauma. Two cases each were ascribed to iatrogenic or otologic causes. Eight cases reported the cause of IFA to be either secondary to dental implants, dental fillings, pulpectomy, cholesteatoma, facial acupressure massage, parotitis, tonsillar infection, or septic pulmonary emboli. Finally, the remaining 2 cases were idiopathic in nature. After excluding the patients from the retrospective review without past medical history, 48 cases remained. Comorbid conditions reported with infratemporal abscesses included diabetes mellitus (n = 8), hypertension (n = 3), and renal disease (n = 2). Aside from these measures, there were no other risks factors identifiable from these cases. All included etiologies are further detailed and referenced in Appendix B.
Assessment and Diagnosis
The average time from acute symptom onset to diagnosis was 14.8 days (SD ± 18.0), after removing two cases with intervals of 2 and 5 years from the analysis. The time from an IFA-precipitating procedure to diagnosis was calculated to be 22.6 days (SD ± 30.2). All patients were assessed through imaging, with computed tomography (CT) (n = 46/67) being the most common modality utilized. CT and magnetic resonance imaging (MRI), MRI alone, and radiograph were utilized in 13/67, 4/67, and 4/67 cases, respectively. There were 31 cases that specified using contrast with their respective imaging modality. The diagnosis of IFA was able to be confirmed in 59/67 cases with imaging.
Symptoms on presentation were collected for all 48 cases from case reports and series. The most common symptoms include pain (n = 40), swelling (n = 39), and trismus (n = 36). Fewer patients reported fever (n = 16), and only 2 cases with dysphagia were encountered. Seven cases reported cranial nerve (CN) V involvement, and 3 patients presented with deficits in CN VII function. Otherwise, there was only 1 additional case of CN VI palsy, for a total of 11 cases with cranial nerve function impairment.
Microbiology and Antibiotic Management
Microbiology Obtained from Culture.
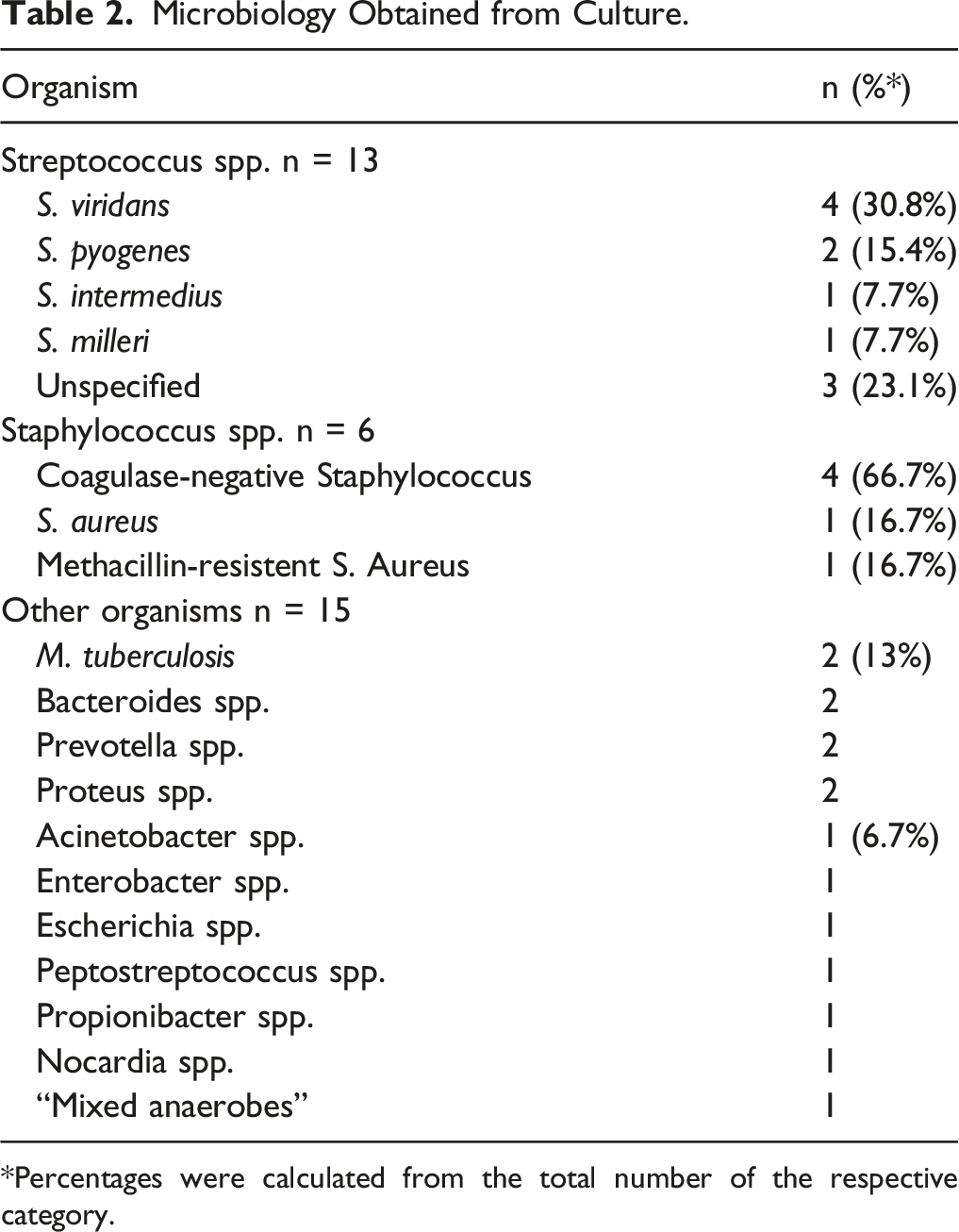
*Percentages were calculated from the total number of the respective category.
Treatment and Outcomes
The most common method of definitive treatment for IFA was through incision and drainage (I&D) of the abscess. Twenty-two patients were managed with intraoral I&D, 18 with extraoral I&D, and 7 with combined intra-extraoral I&D. Ten cases mentioned I&D but did not specify the technique or whether the procedure was intra or extraoral. Endoscopic sinus surgery was performed in 6 cases, 4 of which specified maxillary antrostomy. Three patients were exclusively treated with antibiotics. Additional procedures that were performed included a mastoidectomy, craniotomy, and facial demasking flap. The case reports and series identified otolaryngologists (n = 18) and oral and maxillofacial surgeons (n = 17) as the most frequent surgical teams involved with IFA I&D. Notably, of the 5 patients that experienced intracranial spread, one was left with the long-term sequelae of right-sided limb hemiplegia and another developed a general disorientation that did not resolve. Finally, 45 of the 48 patients from the case reports and series were deemed to have achieved complete resolution, but this data was not available from the abstracts of 3 studies written in non-English language.
Discussion
The IF has been well-described as a wedge-shaped area along the skull base, but its exact limits according to the literature are controversial. 13 -15 In the present study, the boundaries of the IF described as following: 1) anteriorly by the posterior wall of the maxillary sinus, 2) posteriorly by the tympanic segments of the temporal bone and the mastoid process, 3) superiorly by the inferior surfaces of the squamous segment of the temporal bone and the greater wing of the sphenoid, 4) inferiorly by the medial pterygoid muscle attachment to the mandible, 5) medially by the tensor veli palatini and medial pterygoid muscles, and 6) laterally by the medial surfaces of the mandible and zygomatic arch. The IF communicates with other deep neck spaces including the masticator and parapharyngeal spaces, yet it is important to remember that these spaces are distinct and do not overlap completely. For instance, the masticator space extends past the medial surface of the mandible to incorporate the masseter muscle and also ascends to the temporalis muscle. In the present study, patients with abscesses arising within the masticator space outside of the boundaries of the IF, including isolated submasseteric or temporalis muscle abscesses, were excluded. Additionally, deep neck abscesses arising from the erosion of the mastoid tip, also known as Bezold’s abscesses, may also spread anteromedially to the IF. However, these abscesses always involve the mastoid tip and extend from that point between the digastric ridge and the insertion of the sternocleidomastoid. Our initial review did include “Bezold” as a search term, but we found that the vast majority of these case series or reports did not clearly define the extent or location of the abscess. Therefore, we determined that the inclusion of Bezold’s abscesses was not within the scope of this investigation.
The IF is a constricted, deep-seated space housing several vital anatomical structures, and abscess formation may lead to the development of cranial nerve, intracranial, or mediastinal complications. Several neurovascular structures pass through or near the IF to reach their destinations. These include the maxillary (CN V2) and mandibular (CN V3) nerves which cross the superior boundary of the IF after exiting foramen rotundum and ovale, respectively. 15 Therefore, any mass or pressure exerted within the IF may compress these nerves, whether through iatrogenic causes, tumors, or abscesses. In the present study, several patients reported hypesthesia along a CN V3 distribution, likely as a result of compression of the mandibular nerve. 1,16 -18 Additionally, one patient continued to experience paresthesia and tenderness along a CN V2 distribution even after 2 years post-operatively. The presence of the aforementioned foramina also provides a path for pathogens to traverse intracranially, as noted in five of the cases in the current study. 18 -22 Four of these patients developed intracranial abscesses, whereas another developed a subdural empyema. Furthermore, the IF communicates with the parapharyngeal space, which can lead to the direct spread of infection to the thorax. One patient was reported to develop a mediastinal abscess secondary to an odontogenic IFA. 23 The presence of such vital structures in such a constricted, and difficult to access region reinforces the caution that otolaryngologists and other surgeons should exercise when exploring or operating nearby the IF.
The pathogenesis of IFA has been proposed by Yonetsu et al. to odontogenically arise from the mandible and maxilla and contiguously expand through the parotideomasseteric fascia and into the masticator space. 24 The authors have found that the masseter and medial pterygoid muscles are the most commonly involved. It is important to note that involvement of the medial pterygoid muscles allow for direct extension into the IF since the masticator space and IF share the same medial boundary. As for cases with sinus etiology, it has been suggested that local invasion of the IFA is attributed to translocation across the maxillary sinus wall, providing direct access to the IF. 25 Prior cases involving significant facial fractures may create posterior maxillary wall defects, facilitating this same pattern of bacterial invasion. 3 One case of infratemporal abscess secondary to sphenoid sinusitis proposed that the infection spread through the sphenoid emissary foramen, granting exposure to the cavernous sinus. 19 From there, the pathogens would be in relatively close proximity to the IFA as well as have a direct path intracranially. One case involved a cholesteatoma with the complete erosion of the anterior-medial external auditory canal, forming a direct communication with the temporomandibular joint (TMJ). 26 This allowed for the adjacent spread of bacteria into the IF, leading to the development of IFA. The two otologic cases were similar, with one affecting the TMJ and the other eroding through the temporal bone directly into the IF. 27,28
The rarity and non-specificity of symptoms associated with IFA may lead to delays in diagnosis. A study performed in France examining 408 patients over 6 years diagnosed 7 patients with IFA, yielding an incidence rate of 1.7%. 29 Additionally, the presenting symptoms of IFA are non-specific and include fever, pain, and swelling. Trismus, although non-specific, should alert any physician that IFA should be included within the differential diagnosis. The infrequency and non-specific presentation of IFA may partly explain the delays from symptom onset to diagnosis. The prior series with 7 patients found an average interval from acute symptom onset to diagnosis to be 8.4 days, but our findings were relatively higher at 14.8 days. 29 We found the SD for this interval to be quite large at 18.0, highlighting the significant variability between patients. In addition, this delay is greater when examining the interval between the tooth extraction and precipitating procedure to diagnosis at 22.6 days (SD ± 30.2). Although several patients reported symptoms of chronic infection prior to tooth extraction, exposing an intraoral wound to various pathogens is likely why acute symptom worsening occurred afterward. The high variation in time before diagnosis underscores how some patients will experience untimely diagnoses, and these delays may lead to severe consequences when considering the aforementioned sequelae of IFA.
The present study is the first systematic review of the literature regarding IFA. Here, we have attempted to characterize five major domains pertaining to IFA including: 1) general characteristics, 2) risk factors, 3) diagnosis, 4) microbiology and antibiotics, and 5) treatment and outcomes. Important takeaways from this study include are as follows. The aforementioned risk factors of IFA and patient presentation with trismus are important to remember, particularly when creating a differential diagnosis. Although odontogenic causes are the most likely, other etiologies should be kept in mind. Patients should undergo preoperative imaging since these imaging modalities were able to confirm the diagnosis of IFA in 59 of 67 patients from this review. This proportion increases (59/63) when factoring out several studies that made use of radiographs. 3,30,31 The first-line imaging modality is contrast-enhanced CT and should be utilized when feasible. 32 Although only 31 cases reported using contrast in this review, it is likely that this number is underreported. Antimicrobial treatment should initially offer broad coverage due to the high variability of microorganisms and multiple reports of polymicrobial growth on culture. Although the majority of cultures only grew 1 organism and 10 cultures showed no growth, this may be explained by prior extensive antibacterial regimens. Antibiotic therapy may be narrowed once sensitivity and strains are acquired. Our review has found that antibiotic therapy was continued for an average of 4 weeks, which is in-line with recommendations for treating more severe infections. 31,33 Finally, the definitive treatment for IFA is incision and drainage. Although deep neck space infections have been found to recur in some individuals, all infectious foci should be eliminated to reduce the chances for recurrence. 34,35 Although intraoral and extraoral incisions were the most commonly reported surgical modalities, endoscopic sinus procedures including middle meatus antrostomy may be considered. We were unable to determine which surgical method was optimal since the data from these case reviews were not reported in systematic manner, with objective quality measures.
This study has several limitations. First, our sample size was rather limited, as IFAs are quite rare and only few reported cases exist in the literature. Second, several case reports provided vague timelines pertaining to the duration of antibiotic treatments or time from acute symptom onset to treatment. However, we made our best attempts to approximate these time intervals. Additionally, since this review was of individual case data, there is a high likelihood for reporting bias. Finally, we excluded Bezold’s abscesses from this review, even though a significant proportion of IFAs may arise from this pathology. The incorporation or individual analysis of Bezold’s abscesses should be addressed in future research. However, our study also has several strengths. Multiple reputable databases were utilized during the initial search to ensure a broad acquisition of reports. Furthermore, we adhered to the PRISMA guidelines and used multiple authors in the review process to limit bias. Finally, we were the first to attempt to systematically characterize a novel pathology that has not been well-described previously.
Conclusion
Here, we present the first systematic review of infratemporal abscesses. While this condition is a rare complication most commonly arising from odontogenic infections, the sequelae of advanced disease are severe due to the delicate nature of the neuroanatomical area involved. Therefore, identifying patients earlier in the disease process is essential in preventing complications and improving patient outcomes. It is our hope that our characterization of the general characteristics, risk factors, assessment and diagnosis, microbiology, and treatment and outcomes pertaining to IFA will help raise physician awareness and understanding of this unique pathology. Further research is necessary to expand on the findings that we highlight in the present article.
Supplemental Material
Supplemental Material - Infratemporal Fossa Abscesses: A Systematic Review of Cases
Supplemental Material for Infratemporal Fossa Abscesses: A Systematic Review of Cases by Kurtis Young, Dennis M. Tang, and Arthur W. Wu in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Arthur Wu is a speaker for Sanofi/Regeneron
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.