
Abstract
Pleomorphic liposarcomas (PLS) are the rarest subtype of liposarcomas, representing only 5–10% of liposarcomas. Pleomorphic liposarcomas are extremely aggressive and have a poor prognosis. Here, we present the case of a 66-year-old female who presented with difficulty swallowing, talking, and hearing. An extensive investigation revealed the presence of an aggressively growing parapharyngeal space mass. The patient underwent a left parapharyngeal space exploration and left deep lobe parotidectomy by the cervicoparotid approach. Histopathological evaluation of the surgical specimen further confirms the presence of pleomorphic subtype of liposarcoma. The patient received adjuvant radiotherapy following the procedure. At 6 months postop, the patient is in good health and shows no evidence of recurrence. In addition to this treatment, we discuss the radiologic and histologic findings of this current case.
Introduction
Liposarcomas are among the most prevalent malignancies with diverse type of adipocytic distinction. While liposarcomas are known to typically occur in the extremities or the abdomen, only 2–9% of liposarcomas are found in the head or neck region. 1 Among the liposarcomas, pleomorphic liposarcoma (PLS) is the rarest subtype representing only 5–10% of all the liposarcomas. Pleomorphic liposarcoma is delineated by the presence of pleomorphic lipoblasts, defined as having a distinct lipid sphere that surrounds the nucleus of the cell. 2 When conducting an examination, the mass is typically firm and fixed, as well as no evidence of regional lymphadenopathy. Pleomorphic liposarcomas of the head and neck have a high recurrence rate after treatment and an overall poor prognosis, as evidenced by a mortality rate of 50%. 3 With respect to prevalence in the head and neck, only 1% of PLS tumors have been found in the parapharyngeal space. 2 The extremely low prevalence of parapharyngeal space pleomorphic sarcoma has yielded minimal research with respect to etiology, outcomes, prognosis, and treatment in this unique and anatomically complex area of the body.
Sugery of the parapharyngeal space is very complex due to the challenging anatomy and orientation of the space, with the complication rate being as high as 55-57%. 4 The parapharyngeal space is a region in the suprahyoid neck that is shaped like an inverted pyramid. Stambuk et al. describe that the rearrangement of the fat in the parapharyngeal space assists in confirming the diagnosis radiologically. 5 The parapharyngeal space is a rare location for neoplasms to occur, as indicated by 0.5–1% of head and neck tumors found there. 4 In this study, we present a rare case of pleomorphic liposarcoma in parapharyngeal space who underwent surgery and adjuvant radiotherapy.
Case Report
The patient is a 66-year-old female who presented to our hospital with complaints of difficulty swallowing, talking, and hearing. On examination, we noticed a left-sided, dumbbell-shaped parotid mass. A head and neck MRI scan revealed interval growth of the tumor with possible carotid artery encasement and displayed a potential increase in the tumor dimension by 30% compared to the MRI which was taken 2 months prior. Examination redemonstrates previously identified lobulated T1 hypointense, and T2 hyperintense solidly enhancing mass lesions with internal septations (Figure 1A). On presentation, the patient displayed facial and hypoglossal nerve weakness. A subsequent balloon occlusion study was performed which showed collateral perfusion from the branches of the left superior thyroid, lingual, and facial arteries. The patient underwent surgery, consisting of left parapharyngeal space exploration and left deep lobe parotidectomy by way of the cervicoparotid approach. The case was structured with the option of performing lip-split mandibulotomy if necessary for access. Mandibulotomy was not required as the tumor was able to be delivered from under the body of the mandible and a deep lobe parotidectomy was then performed, with the facial nerve being preserved. There was no evidence of a breach of the pharynx. Muscular margins from the medial pterygoid, posteriorly digastric, stylohyoid, and stylopharyngeus were removed. Preoperative MRI of neck tissue with IV contrast reveals 3.4 cm AP by 7.9 cm transverse by 8.4 cm craniocaudal mass (yellow arrow). (B) MRI head and neck, axial view (post resection). Extensive soft tissue inflammatory changes in the surgical bed. (C) MRI head and neck, axial view (at 6 months postop follow-up).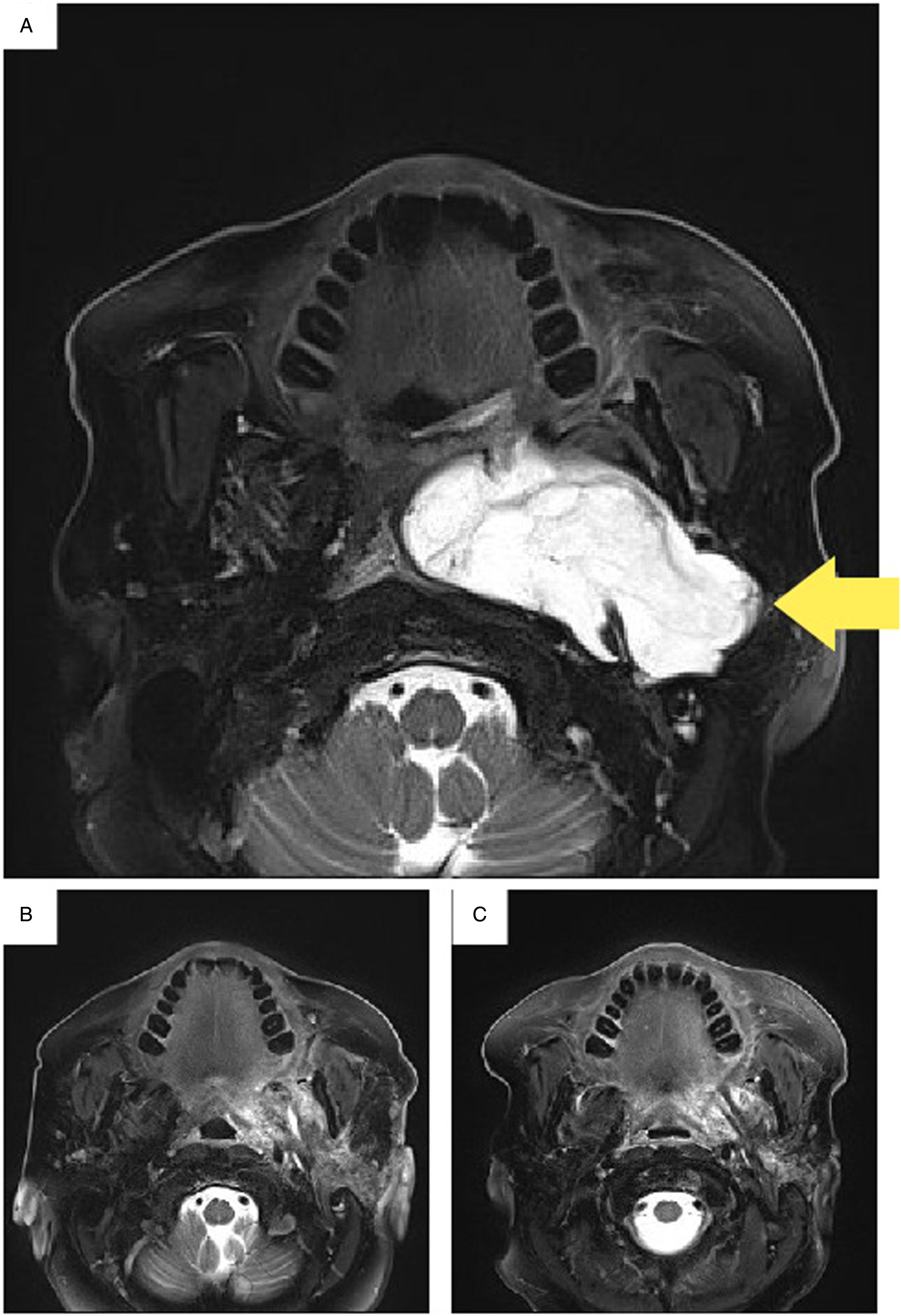
Surgical specimens measuring 12.0 × 10.0 × 3.2 cm with an additional left parapharyngeal space mass measuring 5.5 × 3.5 × 1.5 cm with additional masses in the deep parotid tissue, left submandibular gland, and left neck lymph nodes were sent for histopathological evaluation. Histopathological results revealed liposarcomatous extensive myxoid changes with consistent pleomorphic subtype (Figure 2). To confirm this further, the chromosomal microarray was done which interprets that the genome profile is consistent with either a near-haploid or a pseudohyperdiploid clone which is the usual abnormality found in pleomorphic liposarcoma. The lymph nodes were negative for invasion. Formalin-fixed paraffin-embedded sections stained with Hematoxylin and Eosin (H&E) from the initial surgery demonstrated a malignant neoplasm composed of pleomorphic lipoblasts (black arrow).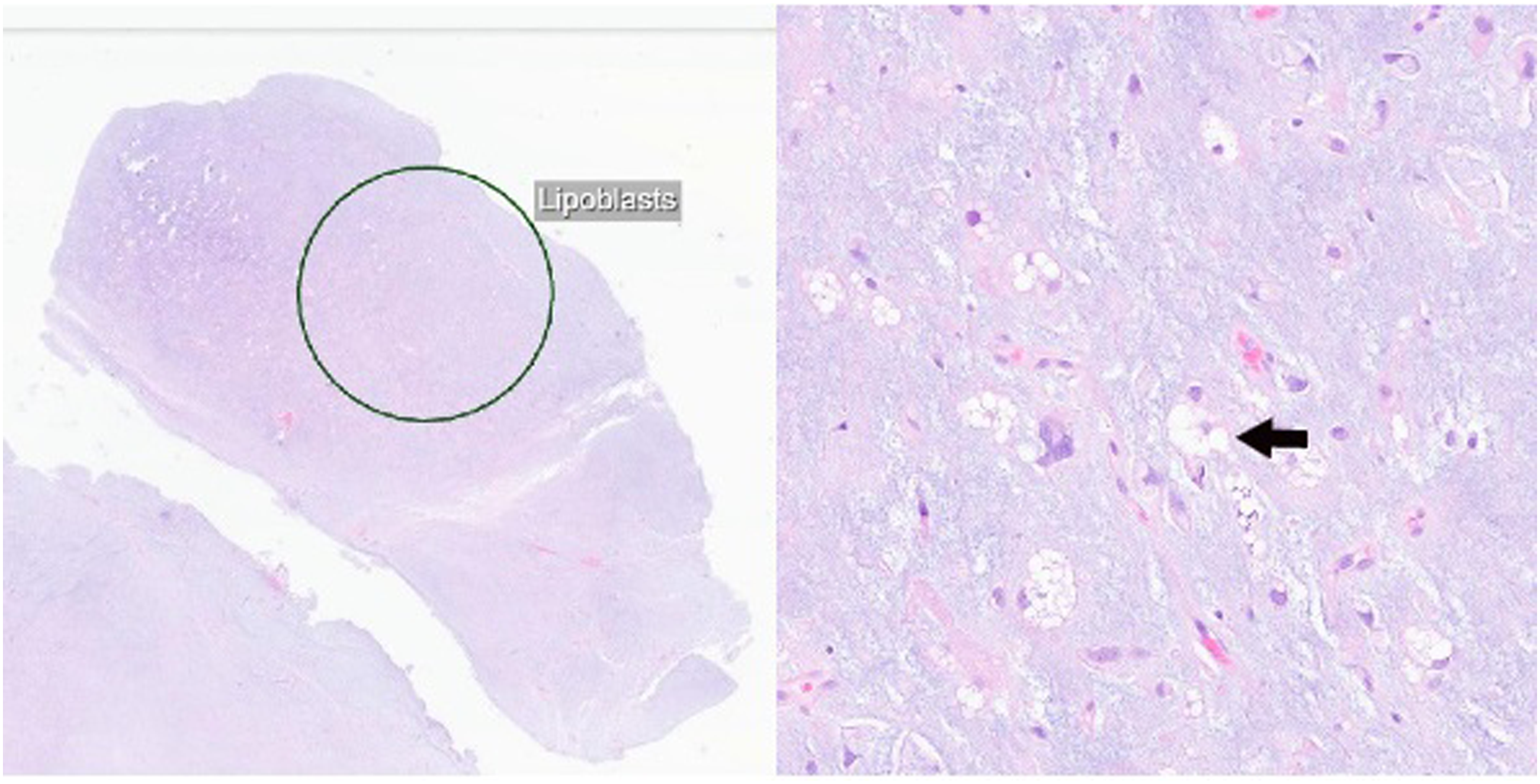
Postoperative period was uneventful. Head and neck MRI taken at 18th day postop showed evidence of gross total removal of the tumor (Figure 1B) with inflammatory changes. Subsequently, the patient was started on radiotherapy. The patient then underwent postop radiation therapy, receiving 7000 cGy for over 8 weeks of treatment. During this period, the patient did not exhibit any specific symptoms. At the 6th month of the postop period, a repeat MRI of the head and neck was taken to reveal no recurrence of the tumor (Figure 1C).
Discussion
We performed an exhaustive literature search and found few cases of head and neck pleomorphic liposarcomas. In one case, a 60-year-old male presented with a posterior auricular mass and no obvious mastoid entanglement. The patient underwent a resection of the mass, including the periosteum of the temporal/occipital bone and fragments of the sternocleidomastoid muscle, trapezius, and sub-occipital fat. 3 Postoperative imaging revealed no metastasis, and the patient underwent radiation. 3 In the second case, a 56-year-old male presented with an ipsilateral mass in the inferior region of the parotid gland. The patient underwent a total parotidectomy with levels II-V selective neck dissection. The patient underwent postoperative radiation. 3 At a one-year follow-up, both patients presented with no sign of recurrence. Since this neoplasm is extremely rare, there is little research explaining the pathologic and clinical presentation, especially in the head and neck region. However, a case series represented by 19 patients with pleomorphic liposarcomas in various regions of the body was reviewed. In those 19 cases, PLS tumors were identified in the quadriceps, thigh, retroperitoneum, ankle, deltoid, and upper arm. The patients underwent wide local excision of the tumor, with 10 of those patients receiving postop radiation. Survival data, with an average of 35 months postop, revealed 9 patients died from the disease, 5 patients were disease-free, 2 patients were alive, but had metastatic disease, and 2 patients were lost to follow-up. 2
Pleomorphic liposarcoma is an extremely aggressive subtype of liposarcoma that can be categorized as a pain-free growing mass that is invisible until it becomes prominent in size or begins to interfere with bodily functions. Pleomorphic liposarcoma can present in any organ, however, research has shown it to be most prevalent in lower extremities. 6 There is no typical treatment plan for PLS, however, surgery has been the observed predominant treatment and sometimes involves the removal of additional organs surrounding the tumor. 6
Conclusion
The analysis of this case is of importance in treating subsequent pleomorphic liposarcomas in the parapharyngeal space. In this case, surgical resection and adjuvant radiotherapy played important roles in preventing relapse. However, further research is needed to determine improvements for treating future pleomorphic liposarcomas in the parapharyngeal space.
Although at 6 months follow-up, the patient didn’t develop new symptoms or further findings on imaging, the patient will continue to have further clinical follow-up to include advanced imaging to ensure there is no recurrence or metastasis of the tumor considering the nature of the tumor.
Supplemental Material
Supplemental Material - Pleomorphic Liposarcoma of the Parapharyngeal Space: A Rare Case Report
Supplemental Material for Pleomorphic Liposarcoma of the Parapharyngeal Space: A Rare Case Report by Karson MacKinnley Gruber, Srivatsa Surya Vasudevan, Jeffrey R. Janus in Ear, Nose & Throat Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Internal funding (No grants).
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Data Availability
Some fields in data are available for scientific researchers upon reasonable request through the corresponding author.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.