
Abstract
Background:
Deep neck infection (DNI) is a potentially life-threatening condition, most commonly arising from odontogenic sources. Dentures frequently act as reservoirs for polymicrobial biofilms, facilitating the persistence and potential transmission of oral pathogens. Despite their widespread use, the role of dentures in predisposing individuals to DNI has not been thoroughly investigated. This study seeks to elucidate the possible association between denture use and the incidence of DNI, thereby addressing a gap in the current understanding of orodental risk factors in DNIs.
Methods:
A total of 337 patients diagnosed with DNI between August 2018 and July 2024 were retrospectively enrolled in this study. Among them, 29 individuals were identified as denture wearers. Relevant clinical parameters, including demographic data, comorbidities, infection characteristics, and treatment outcomes, were systematically analyzed to assess potential associations with denture use.
Results:
Involvement of the parapharyngeal (P = .0172), submandibular (P = .0190), and parotid (P = .0213) spaces in DNI was significantly more frequent in patients with dentures compared to those without. Univariate analysis identified age ≥60 years (odds ratio [OR] 27.000; 95% confidence interval [CI], 2.5034-291.19; P = .0010), C-reactive protein (CRP) level ≥220 mg/L (OR 8.5000; 95% CI, 1.2471-57.933; P = .0201), and involvement of ≥3 deep neck spaces (OR 8.4444; 95% CI, 1.2261-58.159; P = .0258) as significant risk factors for prolonged hospitalization. However, in multivariate logistic regression analysis, only age ≥60 years remained a significant independent predictor of prolonged hospitalization (OR 18.494; 95% CI, 1.5789-216.63; P = .0201).
Conclusion:
In patients with DNI who wore dentures, univariate analysis identified age 60 years or older, CRP levels of 220 mg/L or higher, and involvement of three or more deep neck spaces as significant predictors of prolonged hospitalization. However, multivariate analysis demonstrated that only age 60 years or older remained an independent risk factor for extended hospital stay. These findings highlight the need for targeted health education and preventive measures in elderly denture users to reduce the risk of severe DNI and its complications.
Introduction
Deep neck infection (DNI) represents a life-threatening clinical entity often associated with severe complications, necessitating prompt and aggressive intervention. 1 DNIs involve the deep cervical fascial spaces and potential compartments of the neck, including the parapharyngeal, submandibular, sublingual, retropharyngeal, perivertebral, and visceral spaces. 2 Owing to the anatomical continuity of these spaces, DNIs can disseminate along fascial planes, ultimately extending to the mediastinum. 3 Common and potentially fatal complications include airway obstruction, pneumonia, cervical necrotizing fasciitis, internal jugular vein thrombosis, and descending necrotizing mediastinitis,4 -7 each of which significantly increases morbidity and mortality. DNI is typically polymicrobial in nature, with a higher prevalence among individuals with diabetes mellitus, poor oral hygiene, recent upper respiratory infections, trauma, or those who are immunocompromised.1,8
Dentures, as artificial devices designed to replace lost teeth, are integral components of the masticatory system, facilitating not only the maintenance of oral function but also contributing to facial aesthetics and phonetics. 9 Despite improvements in oral hygiene practices, the demand for dentures continues to rise, particularly among the elderly population. 10 As the number of elderly individuals increases, a deeper understanding of denture-related infections is imperative for formulating optimal treatment strategies for this demographic, especially those with comorbid conditions.
Dentures may serve as niches for the accumulation of polymicrobial biofilms, thereby enhancing the risk of mucosal barrier disruption and increasing susceptibility to DNI. 10 The diverse range of denture types, materials, and fixation methods further complicates the risk assessment. While DNI can be acute and potentially fatal, odontogenic infections are recognized as the most common etiology of DNI in both adult and elderly populations. 11 Nevertheless, the relationship between denture use and the development of DNI remains underexplored in the existing literature. In light of this gap, this article aims to systematically evaluate whether denture use is associated with an elevated risk of deep neck infections, integrating epidemiological evidence with a discussion of underlying microbiological mechanisms.
Materials and Methods
This study retrospectively analyzed the medical records of 337 patients diagnosed with DNI who were admitted to Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan, between August 2018 and July 2024. Diagnostic confirmation was primarily based on clinical manifestations, supplemented by imaging modalities such as computed tomography (CT) and ultrasonography. Data collection in this study involved both retrospective chart review and imaging reassessment. Data extraction was performed by board-certified otolaryngologists with clinical expertise in DNIs. Diagnoses were primarily established based on contrast-enhanced CT findings (Figure 1), which were reviewed and interpreted by the attending otolaryngologist at the time of patient presentation. Following CT imaging, the management of DNI encompassed a multifaceted approach, including airway protection, antimicrobial therapy, surgical intervention, and ultrasound-guided needle aspiration following institutional standards led by otolaryngology team based on the radiological findings and clinical evaluation. Traditionally, open surgical incision and drainage (I&D) under general anesthesia have been the cornerstone of DNI treatment. However, ultrasound-guided needle aspiration was employed as an alternative approach for well-defined, superficial infections. Airway protection was initially achieved through endotracheal intubation, 12 with tracheostomy being performed when deemed necessary. 13 Empirical antibiotic therapy, consisting of ceftriaxone (1 g every 12 hours) and metronidazole (500 mg every 8 hours), was administered to provide broad-spectrum coverage against both aerobic and anaerobic pathogens pending pus culture results. 14 Antibiotic regimens were subsequently adjusted in accordance with culture findings to optimize pathogen-specific treatment.
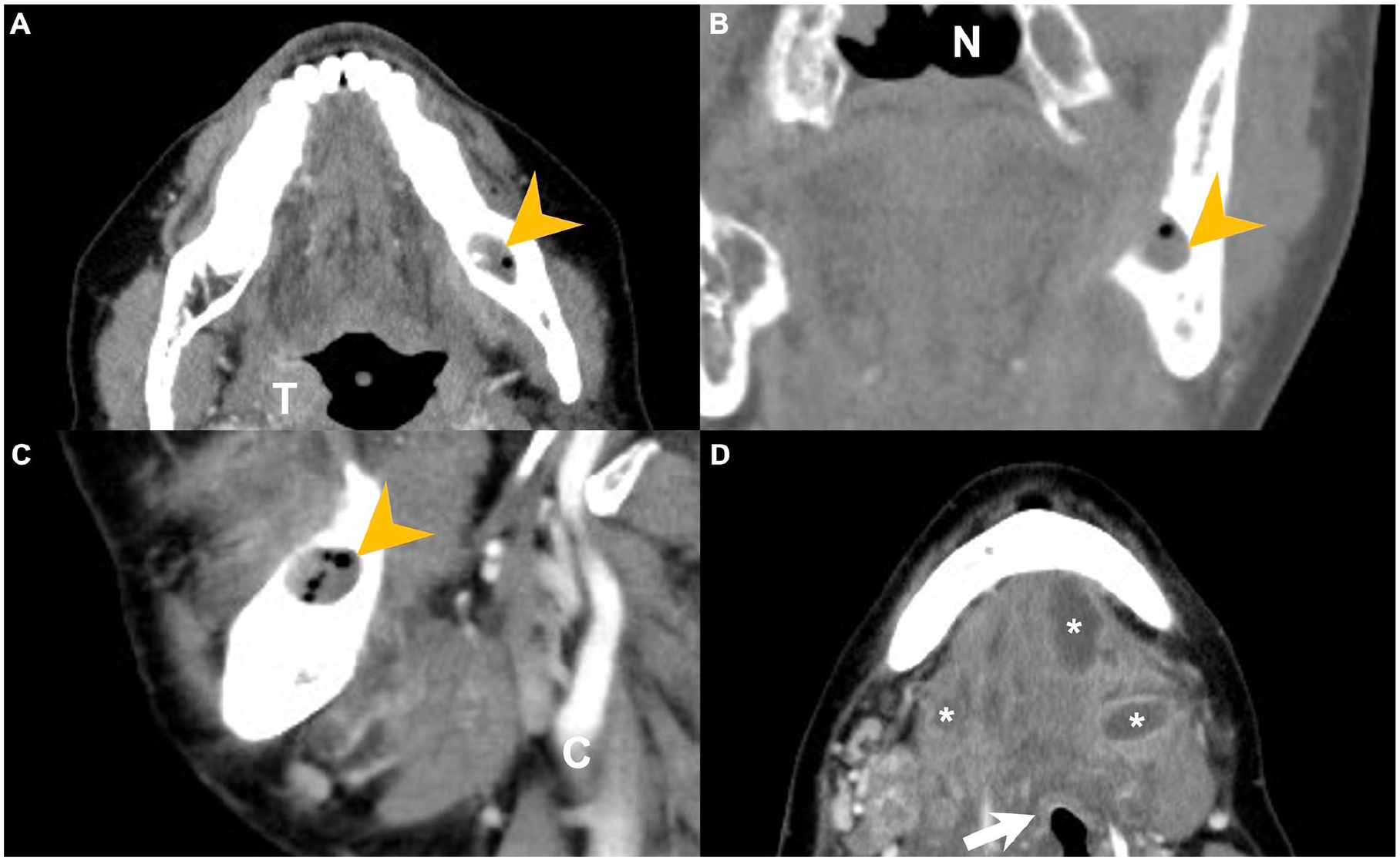
Contrast-enhanced CT images of a patient following removal of infected dentures. Panels (A) and (D) represent axial views, panel (B) shows the coronal view, and panel (C) illustrates the sagittal view. Yellow arrowheads indicate the original dental cavity with gas accumulation. Asterisks mark regions of multiloculated abscess formation. Key anatomical structures are labeled as follows: arrow = epiglottis; C = carotid artery; N = nasal cavity; T = tonsil. CT, computed tomography.
Definition of Denture Types
In this study, the term “denture use” encompasses a range of prosthetic dental devices used to restore missing dentition. Specifically, the following types were included:
1. Removable Partial Dentures: Prostheses designed to replace one or more missing teeth, supported by the remaining natural teeth and oral mucosa. These are entirely removable by the patient and do not involve dental implants.
2. Complete Acrylic Dentures: Full-arch removable prostheses made entirely of acrylic resin, used in edentulous patients. These rest solely on the oral mucosa and alveolar ridge without any implant support.
3. Implant-Supported Prostheses: This category includes both fixed and removable prosthetic restorations anchored by dental implants:
(a) Fixed implant-supported restorations: refer to permanently affixed bridges or full-arch prostheses entirely supported by implants.
(b) Implant-retained removable overdentures: involve prostheses that are stabilized by attachments connected to implants, but still rely partially on the mucosa for support and can be removed by the patient.
For the purposes of this study, all patients using any of the above prosthetic modalities were categorized as “denture users.” This classification was based on dental records and imaging at the time of hospital presentation.
Exclusion Criteria
Patients meeting the following criteria were excluded from the study cohort: those with severe cardiopulmonary diseases, vocal cord paralysis, persistent tracheostomy, or feeding dependence via a nasogastric tube; individuals with a history of prior radiotherapy or surgery involving the head and neck region; patients who had ingested sharp foreign bodies; individuals under the age of 18; and those who were immunocompromised.
Data Collection
Patient data were systematically collected to investigate the potential correlation between denture use and DNI. The variables assessed included demographic factors (such as gender and age), laboratory parameters (including C-reactive protein [CRP] levels and blood sugar), and clinical characteristics such as the number of deep neck spaces involved, specific anatomical spaces affected by the infection, and the presence of mediastinitis. 15 Additional factors included the need for tracheostomy, I&D procedures, and the duration of hospitalization. Pathogen identification, along with the occurrence of complications such as esophageal perforation or acute supraglottitis, was also recorded.
Ethics Statement
This study was approved by the Institutional Review Board (IRB) of the Chang Gung Medical Foundation (IRB approval no. 202401253B0). Data collection was conducted retrospectively, with all patient information anonymized prior to analysis to ensure confidentiality and compliance with ethical standards. The requirement for informed consent was waived by the IRB due to the retrospective nature of the study and the use of anonymized data.
Statistical Analysis
Statistical analyses were conducted using MedCalc software (version 18.6; MedCalc, Ostend, Belgium). The Kolmogorov–Smirnov test was applied to assess the normality of data distribution, which revealed a non-normal distribution. Consequently, categorical variables were compared using the Chi-square test, while continuous variables were analyzed using the non-parametric Mann–Whitney U test. To identify factors associated with the outcome of interest, both univariate and multivariate logistic regression analyses were performed. Variables demonstrating statistical significance in univariate analysis were subsequently included in a multivariate logistic regression model using a forward stepwise selection approach.
The forward stepwise method was chosen to avoid model overfitting, especially given the limited number of events relative to potential predictors, identify independent predictors by adding variables sequentially based on statistical contribution, manage collinearity by ensuring only variables that provide unique explanatory power are retained in the final model, and enhance model parsimony while maintaining explanatory accuracy. A 2-tailed P value of <.05 was considered statistically significant throughout all analyses.
Results
Table 1 summarizes the clinical characteristics of the 337 patients diagnosed with DNI, of whom 223 (66.17%) were male and 114 (33.82%) were female. The mean age of the cohort was 55.85 ± 17.83 years, with an average CRP level of 158.13 ± 108.11 mg/L and a mean blood glucose level of 150.03 ± 72.03 mg/dL. Regarding the anatomical distribution of the infections, 120 patients (35.61%) had involvement of three or more deep neck spaces. The infection locations were as follows: 194 patients (57.56%) had parapharyngeal space infections, 160 (47.47%) had submandibular space infections, 108 (32.04%) had retropharyngeal space infections, 68 (20.17%) had masticator space infections, 60 (17.81%) had parotid space infections, 29 (8.61%) had anterior cervical space infections, 28 (8.31%) had carotid space infections, 24 (7.12%) had visceral space infections, 14 (4.15%) had perivertebral space infections, and 10 (2.96%) had posterior cervical space infections. Mediastinitis was present in 41 patients (12.16%).
Clinical Characteristics of the 337 Patients With DNI.
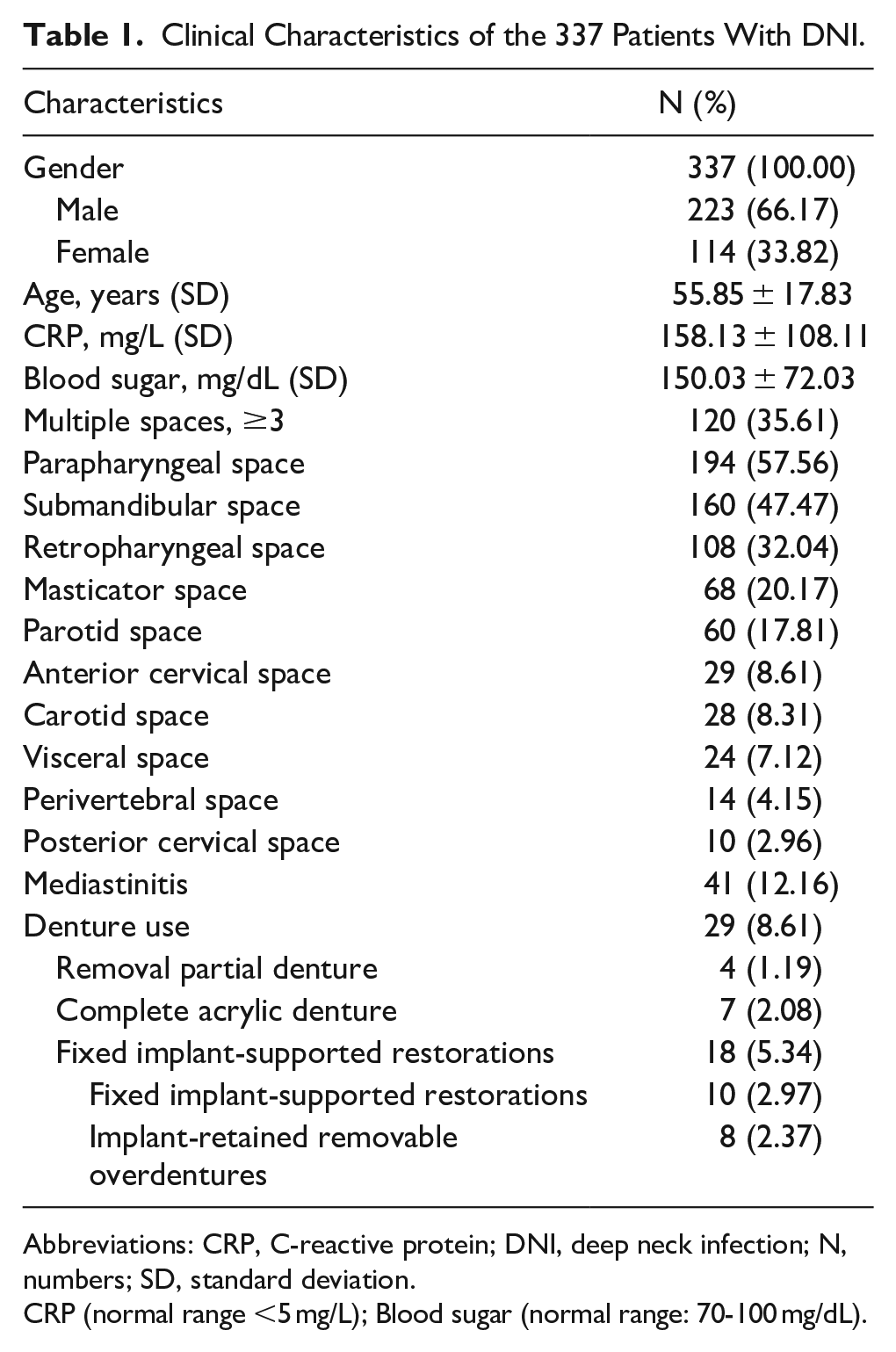
Abbreviations: CRP, C-reactive protein; DNI, deep neck infection; N, numbers; SD, standard deviation.
CRP (normal range <5 mg/L); Blood sugar (normal range: 70-100 mg/dL).
Among the 29 patients (8.61%) identified as denture users, 4 (1.19%) used removable partial dentures, 7 (2.08%) wore complete acrylic dentures, and 18 (5.34%) utilized implant-supported prostheses. Among those with implant-supported prostheses, 10 (2.97%) had fixed implant-supported restorations, while 8 (2.37%) used implant-retained removable overdentures.
Table 2 compares the clinical characteristics between patients with and without denture implants. There were no significant differences in terms of gender, age, CRP levels, or blood sugar levels (P > .05). However, the involvement of the parapharyngeal (P = .0172), submandibular (P = .0190), and parotid (P = .0213) spaces was significantly higher in denture-wearing patients compared to non-denture patients. The occurrence of DNI involving these 3 anatomical spaces was notably more prevalent in denture-wearing patients.
Comparison of Clinical Characteristics Between Patients With and Without Denture Implant.
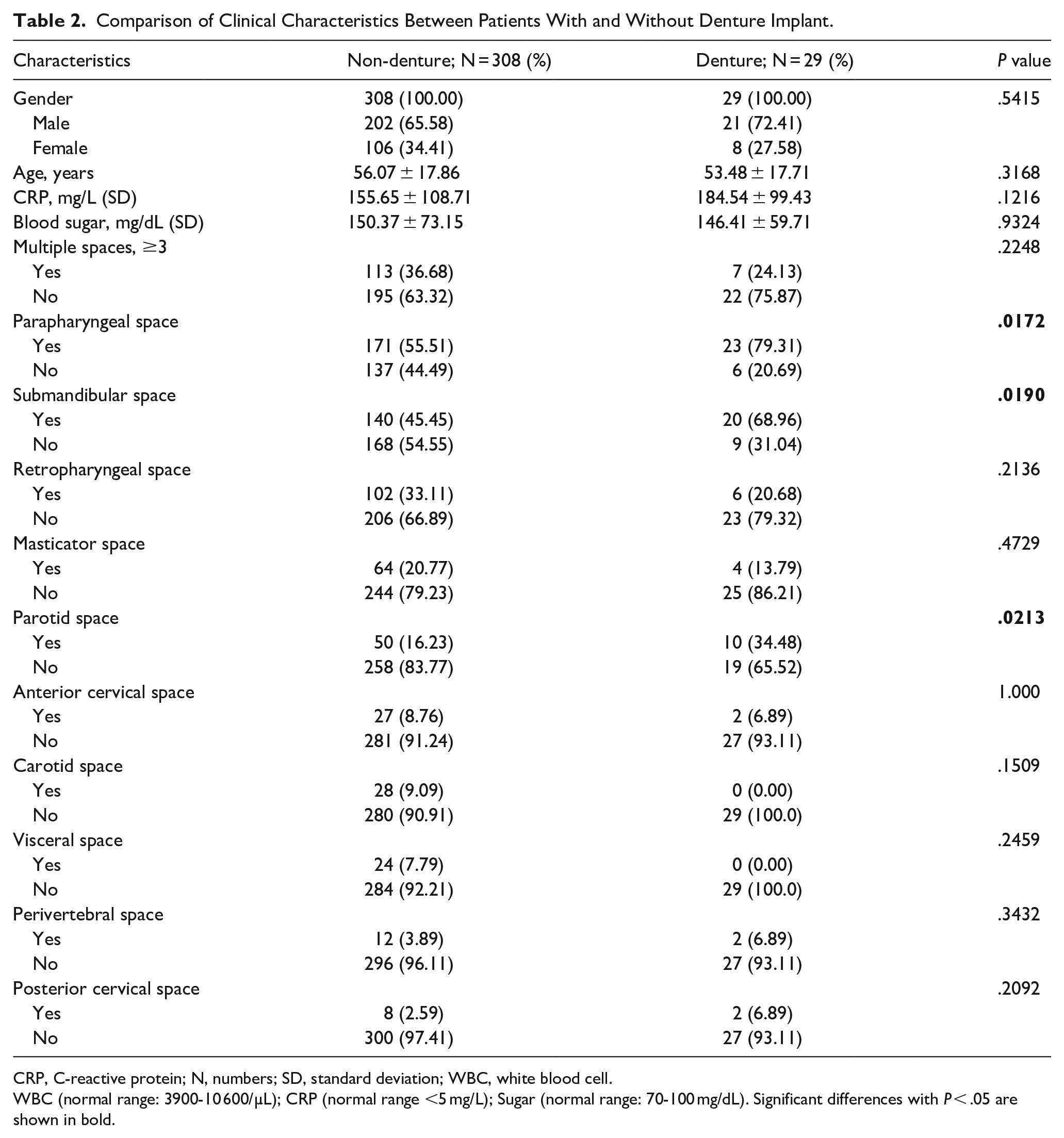
CRP, C-reactive protein; N, numbers; SD, standard deviation; WBC, white blood cell.
WBC (normal range: 3900-10 600/µL); CRP (normal range <5 mg/L); Sugar (normal range: 70-100 mg/dL). Significant differences with P < .05 are shown in bold.
Table 3 presents a comparison of management strategies between patients with and without denture implants. No significant differences were observed between the 2 groups regarding the need for tracheostomy, I&D procedures, or the length of hospital stay (P > .05).
Comparison of Management Between Patients With and Without Denture Implant.
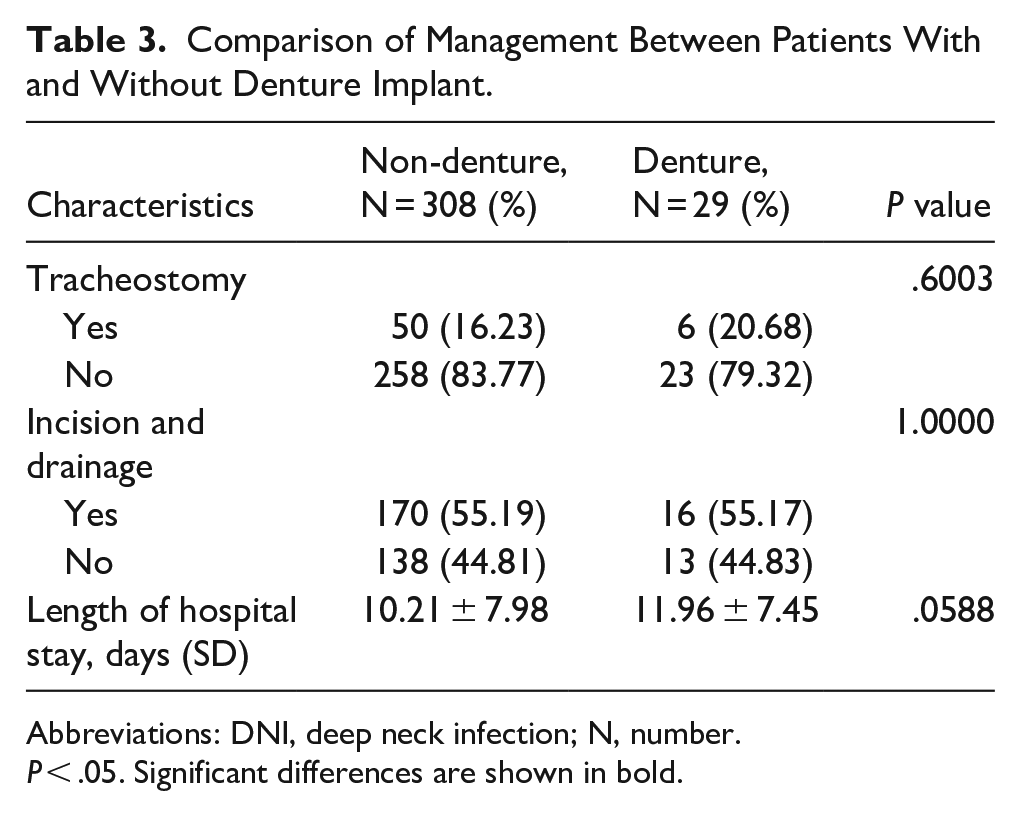
Abbreviations: DNI, deep neck infection; N, number.
P < .05. Significant differences are shown in bold.
Table 4 compares the pathogens identified in patients with and without denture implants. There were no significant differences in the microbial pathogens between the 2 groups, which is consistent with the anticipated polymicrobial nature of DNI, as demonstrated in prior studies. 16
Comparison of Pathogens Between Patients With and Without Denture Implant.
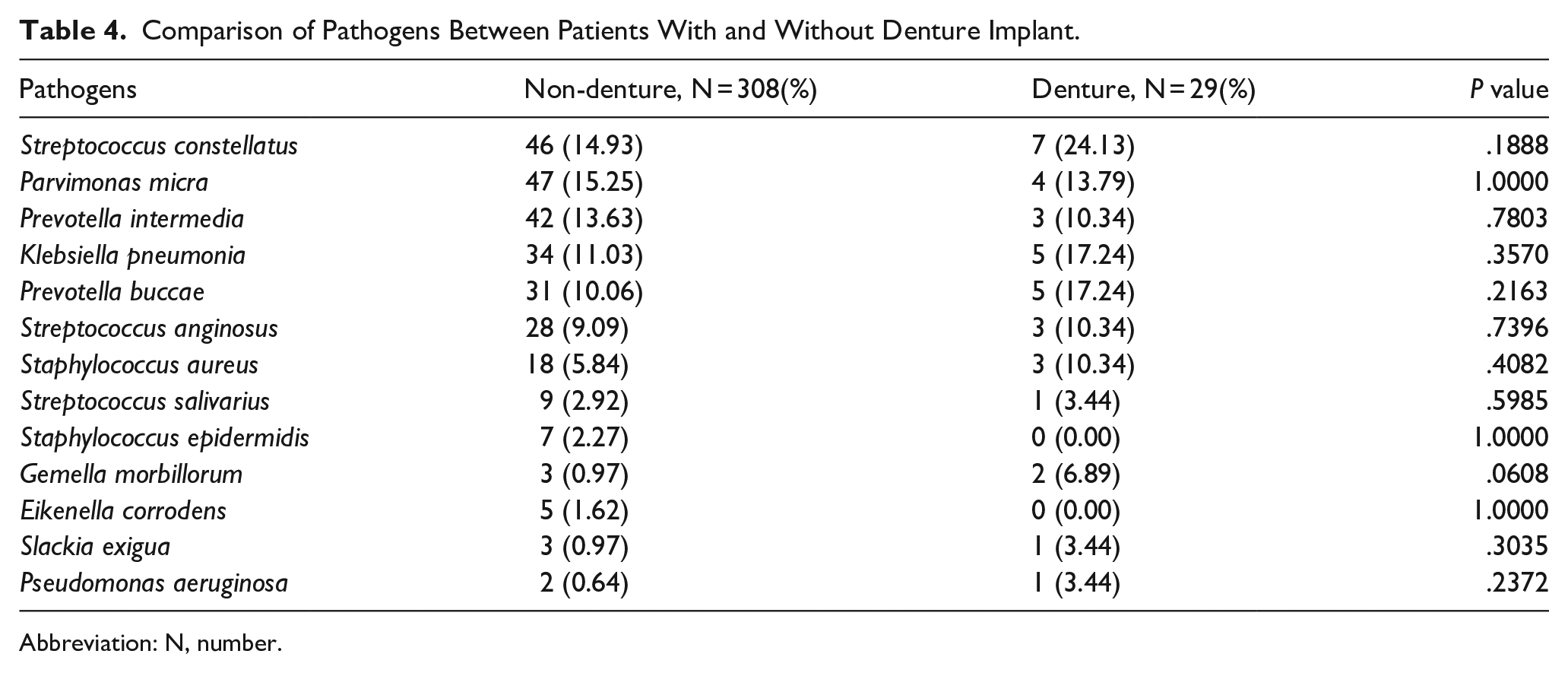
Abbreviation: N, number.
Table 5 presents the results of univariate and multivariate analyses of the 29 DNI patients with denture implants who experienced prolonged hospitalization, defined as a hospital stay exceeding 14 days. The univariate analysis identified several significant factors associated with prolonged hospitalization, including advanced age, elevated CRP levels, and involvement of multiple deep neck spaces. In contrast, the multivariate analysis revealed that advanced age was the sole independent risk factor for prolonged hospitalization. Specifically, patients aged 60 years or older were found to have a significantly higher risk for prolonged hospitalization (odds ratio [OR] 27.000, 95% confidence interval [CI] 2.5034-291.19, P = .0010). Furthermore, a CRP level of 220 mg/L or higher was also identified as a risk factor for extended hospitalization (OR 8.5000, 95% CI 1.2471-57.933, P = .0201). In addition, involvement of three or more deep neck spaces was associated with a significantly prolonged hospital stay (OR 8.4444, 95% CI 1.2261-58.159, P = .0258). In the multivariate analysis, however, only age ≥60 years remained a statistically significant independent factor for prolonged hospitalization in DNI patients (OR 18.494, 95% CI 1.5789-216.63, P = .0201).
Univariate and Multivariate Analyses of 29 DNI Patients With Denture Implant for Prolonged Hospitalization (>14 days).
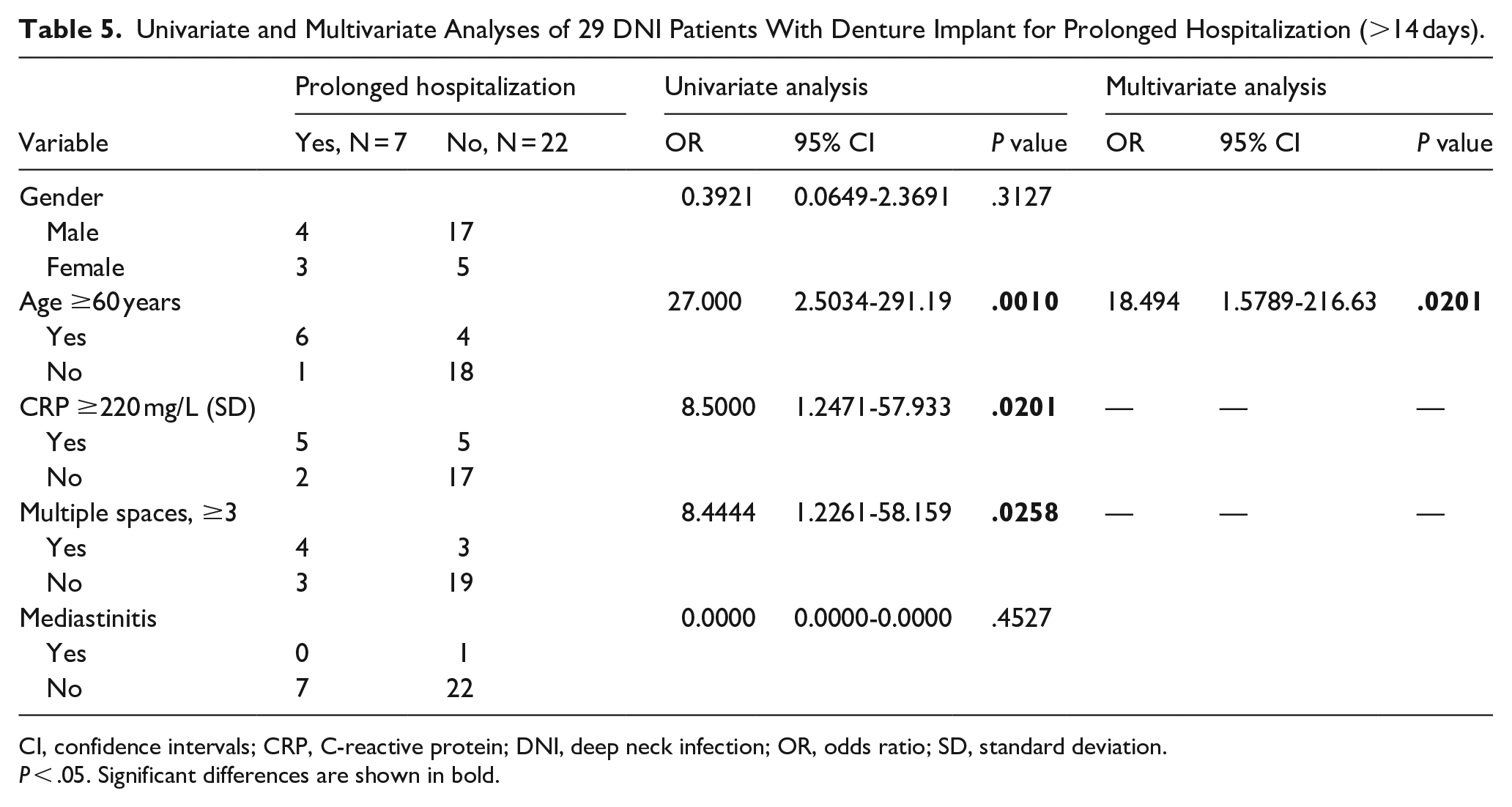
CI, confidence intervals; CRP, C-reactive protein; DNI, deep neck infection; OR, odds ratio; SD, standard deviation.
P < .05. Significant differences are shown in bold.
Table 6 compares the complications between patients with and without denture implants. There were no significant differences observed between the 2 groups in the incidence of mediastinitis, esophageal perforation, or acute supraglottitis (all P > .05).
Comparison of Complications Between Patients With and Without Denture Implant.
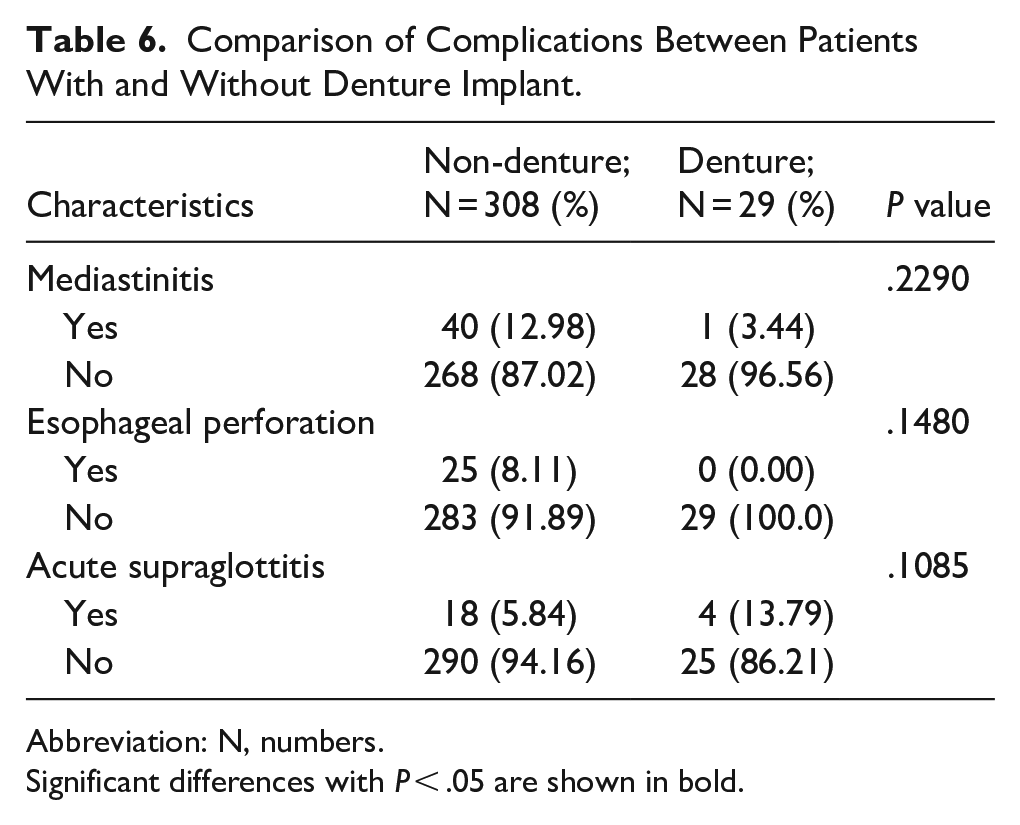
Abbreviation: N, numbers.
Significant differences with P < .05 are shown in bold.
Discussion
The microbiological spectrum of DNIs typically includes aerobic and anaerobic organisms, with Streptococcus spp., Staphylococcus aureus, and various anaerobes commonly implicated. Contrast-enhanced CT is widely regarded as the diagnostic imaging modality of choice, given its superior ability to identify the location, extent, and severity of the infection. Among the various etiologies, odontogenic infections constitute the most frequent source of DNI, highlighting the essential role of oral health maintenance in its prevention. Dentures, as a means of prosthetic rehabilitation, are employed to restore oral function, aesthetics, and quality of life, particularly in edentulous patients. Dentures can be broadly classified into several types based on indication, structural design, and patient-specific needs. Complete dentures are the most commonly utilized prostheses among elderly individuals with total edentulism in one or both arches. However, insufficient hygiene practices can lead to denture-related stomatitis in both fixed and removable variants. 17 Partial dentures, indicated for individuals with residual dentition, similarly require rigorous hygiene maintenance to prevent plaque accumulation and associated gingival inflammation, regardless of whether the prosthesis is fixed or removable.18,19 Other types of prosthetic options, including implant-supported dentures, immediate dentures, flexible dentures, and overdentures, are selected based on anatomical, functional, and patient-preference considerations, each necessitating tailored hygiene protocols to prevent local and systemic complications.
Although odontogenic infections have been well established as the primary etiological source of DNI, the role of denture-related pathology, particularly denture-induced gingivitis and stomatitis, has increasingly been recognized as a potential contributing factor to the development of DNI.17,19 In our study, we observed a predominance of male patients, with a mean age of approximately 55 years, findings that are consistent with those reported in previous epidemiological investigations.20,21 Notably, multivariate analysis identified age ≥60 years as an independent risk factor for the development of denture-associated DNI, suggesting a possible correlation between age-related decline in oral hygiene capability, and increased vulnerability to prosthesis-related infections. Despite this association, comparative analysis revealed no statistically significant differences in clinical management strategies, microbiological profiles, or complication rates between patients with denture-related DNI and those with DNI of non-denture origin. This suggests that, while the route of infection may differ, the clinical course and therapeutic approach remain broadly similar across both cohorts.
In our analysis, DNI involving the parapharyngeal, submandibular, and parotid spaces demonstrated a higher association with denture use compared to cases without denture involvement. This spatial predilection may be attributable to anatomical considerations. Similarly, odontogenic infections originating in the mandible can propagate along the mylohyoid line, leading to increased involvement of the submandibular space. 22 Moreover, infections in the masticator space, frequently of odontogenic origin, have been shown to exhibit a strong anatomical and pathological association with the parapharyngeal space, thereby explaining the observed correlation in our cohort. 23 These anatomical and pathophysiological relationships provide a plausible explanation for the distributional patterns presented in Table 2.
As the prevalence of denture use increases substantially in individuals aged 60 years and older, advanced age has emerged as an independent risk factor for denture-associated DNI in our study population. 24 Consequently, older patients may be more susceptible to infections involving multiple cervical fascial spaces compared to their younger counterparts. CRP, an acute-phase reactant synthesized by the liver in response to systemic inflammation, infection, or tissue injury, serves as a sensitive biomarker of inflammatory status. 25 Previous studies have demonstrated an age-related increase in baseline CRP levels, independent of acute pathology, suggesting a heightened inflammatory milieu in older individuals. 26 This trend may account for the observed correlation between elevated CRP levels and multi-space involvement in patients of advanced age, as presented in Table 5. In contrast, no statistically significant differences in complication rates were observed between denture-related and non-denture-related DNI cases, as detailed in Table 6. This may be attributed to the anatomical distribution of infections. The retropharyngeal space, which is commonly implicated in life-threatening complications such as mediastinitis and esophageal perforation, was not among the most frequently involved spaces in denture-associated DNI.2,27 Instead, infections in the denture group predominantly affected the parapharyngeal, submandibular, and parotid spaces, which are less commonly associated with such severe sequelae.
Although our study demonstrates a potential association between denture use and specific patterns of DNI, it is important to recognize that the risk conferred by dentures is not solely determined by their presence, but also by how they are used, maintained, and cared for over time. Persistent biofilm maturation may disrupt the mucosal barrier, allowing microorganisms to invade deeper tissues and potentially spread along cervical fascial planes. Duration of denture use is another relevant factor influencing infection risk. Long-term wearers, especially those who have used the same prosthesis for many years without replacement or professional adjustment, often exhibit increased plaque retention and mechanical irritation of the oral mucosa. These chronic inflammatory processes may serve as a nidus for more severe infections such as DNI, particularly in elderly patients who diminished salivary flow. Prosthesis maintenance, including both daily cleaning routines and periodic professional evaluation, is fundamental to mitigating these risks. Regular mechanical cleaning and professional scaling or denture adjustments can significantly reduce microbial load and biofilm thickness. Patients who do not adhere to recommended maintenance practices, or who lack access to routine dental care, are therefore likely to be at greater risk of infection. Incorporating these parameters would allow a more nuanced understanding of the pathways by which denture-related biofilms contribute to DNIs. In addition, such data could inform targeted preventive strategies, including patient education campaigns emphasizing the importance of meticulous denture care and regular dental evaluations to reduce the burden of severe odontogenic infections.
Limitations
Several limitations should be acknowledged in the interpretation of this study’s findings. Foremost, the retrospective design inherently restricts the level of evidence, rendering the results more susceptible to biases such as incomplete data capture and unmeasured confounding, when compared to prospective or randomized study designs. Additionally, despite the clinical relevance of the topic, the current body of literature focusing specifically on denture-associated DNIs remains limited. The paucity of prior studies constrains the ability to perform meaningful comparisons or to draw broader epidemiological conclusions.
Our study does not distinguish between different types of dentures well, nor does it account for critical variables such as duration of denture use, oral hygiene practices, and the quality of denture fit. Another important limitation is the relatively small number of denture-wearing patients (n = 29) among the total cohort of 337 patients. This low sample size limits the statistical power of the analyses, particularly the multivariate logistic regression, and increases the risk of type II error. Therefore, the findings regarding the association between denture use and DNI must be interpreted with caution, and further studies with larger sample sizes are warranted to confirm these associations.
Although we conducted a regression analysis within the denture group to explore potential predictors of prolonged hospitalization (Table 5), we did not perform a parallel multivariate analysis in the non-denture group. Therefore, the specificity of these findings to denture-associated DNI remains uncertain and should be interpreted with caution.
Given these limitations, there is a clear need for future investigations with more rigorous methodological designs. Specifically, prospective studies involving larger, heterogeneous patient populations across multiple centers are warranted to validate our findings, enhance generalizability, and provide a more comprehensive understanding of the etiopathogenesis and clinical implications of denture-associated DNI.
Conclusion
This study investigated the association between DNI and denture use, with particular emphasis on the clinical implications in the elderly population. Our findings identified age ≥60 years as an independent risk factor associated with prolonged hospitalization among denture-wearing DNI patients. This suggests that advanced age may contribute to more severe clinical courses. Given the preventable nature of many denture-associated infections, we emphasize the importance of targeted oral health education for the elderly population. Enhancing awareness regarding proper denture maintenance and routine oral care may serve as an effective strategy to mitigate the risk of severe odontogenic infections, thereby reducing the likelihood of DNI and its associated morbidity.
Footnotes
Acknowledgements
The authors thank all of the members of Department of Otorhinolaryngology & Head and Neck Surgery, Linkou Chang Gung Memorial Hospital, for their invaluable help.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed in the study are included in this published article. The data are available on request.