
Abstract
Oncocytic tumors comprise a group of rare benign neoplasm of salivary glands, accounting for less than 1% of all salivary gland tumors. Nodular oncocytic hyperplasia characterized by multiple unencapsulated oncocytic nodules in the salivary glands is an extremely rare condition. We report a case of bilateral nodular oncocytic hyperplasia of parotid glands with parapharyngeal space extension in an 80-year-old woman whose initial presentation was recurrent parotitis. Our case may be the first report of nodular oncocytic hyperplasia in the parapharyngeal space, arising from the parotid gland. The patient underwent total parotidectomy and excision of parapharyngeal tumors using a transparotid transcervical approach, and at the 2-year follow-up, no evidence of recurrence was found.
Introduction
Oncocytes are transformed epithelial cells characterized by their large size and abundant eosinophilic granular cytoplasm. 1 The newest World Health Organization (WHO) classification of salivary gland neoplasms includes 3 oncocytic entities: oncocytoma, nodular oncocytic hyperplasia (NOH), and oncocytic carcinoma. 2 Oncocytoma, a well-circumscribed tumor composed of oncocytes, is the most common form. 1 Nodular oncocytic hyperplasia is characterized by multiple nonneoplastic and unencapsulated nodular proliferations comprising oncocytes, which are separated by normal salivary gland tissues. 3 Compared to oncocytoma, NOH has no dominant fibrous capsule. NOH accounts for less than 1% of salivary gland tumors and is diagnosed mainly in the sixth decade of life or later.1,2 The average patient age at presentation is approximately 57 years with 85% of cases occurring in women. 2 The most common manifestation is a painless swelling in the parotid region. Nodular oncocytic hyperplasia is usually unilateral in the parotid glands, with rare bilateral involvement. The cause of NOH occurrence mostly remains unknown. However, human papillomavirus infection (HPV53) and mutations in mitochondrial DNA (m. 4561TA) have been identified as causative factors. 2 To our knowledge, NOH of parotid glands with bilateral involvement of the parapharyngeal space (PPS) has not been reported previously. In this report, we describe the clinical course of NOH in the bilateral parotid glands with PPS extension in an 80-year-old woman. We also briefly review the literature.
Case Report
An 80-year-old woman with hypertension presented with painful bilateral swelling of the infraauricular regions, particularly on the right side, for 2 days. In the emergency department, a fever of 38.0 °C without any other discomfort was noted. She had 2 similar episodes in the last 2 years, both particularly affecting the right side. However, since the symptoms were relieved within 1 to 2 weeks after taking oral antibiotics, she did not seek advice in the absence of inflammation. Physical examination revealed bilateral tenderness and swelling of the infraauricular regions and bulging of the left lateral soft palate. Laboratory tests demonstrated leukocytosis (14 300/mm3) with a predominance of segmented neutrophils (85.2%), and the C-reactive protein level was elevated (16.6 mg/dL). Sonography showed multiple parotid tumors and enlarged lymph nodes at bilateral neck level II. Fine-needle aspiration cytology (FNAC) revealed sheets and clusters of oncocyte-like cells with granular cytoplasm. Contrast computed tomography demonstrated multiple masses in the bilateral parotid regions and PPSs; the largest one had a diameter of approximately 3.8 cm (Figure 1). Warthin tumor with oncocytic differentiation was suspected. Surgery was recommended for histopathologic confirmation and treatment of recurrent obstructive parotitis. She underwent surgery on the right side first because more severe symptoms were present on that side. Although the physical examination showed a bulge of the left-side soft palate, it did not cause dysphagia or other discomfort. Therefore, right-side total parotidectomy with the facial nerve preservation and excision of PPS tumors using a transparotid transcervical approach were conducted.
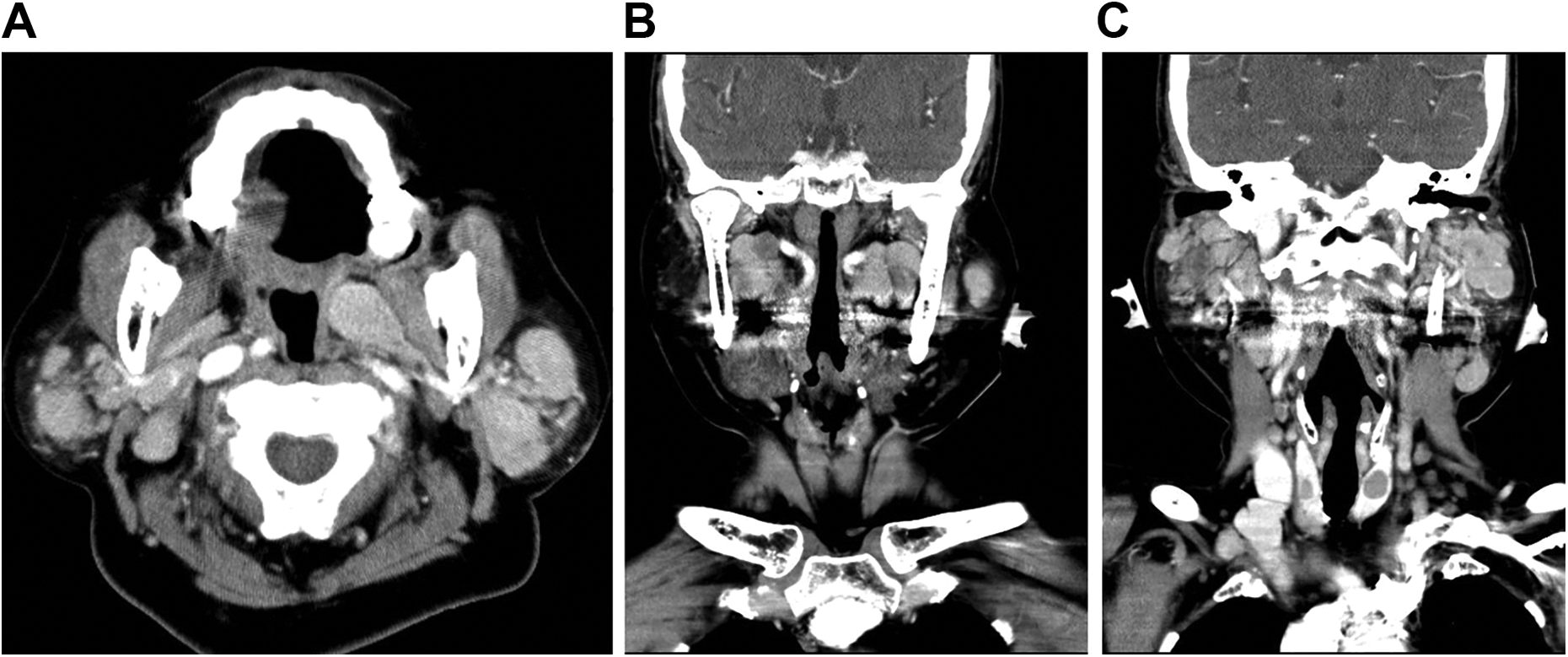
Contrast medium–enhanced computed tomographic images: the axial view (A) and the coronal views (B,C) demonstrated multiple nodular tumors in the bilateral parotid glands and parapharyngeal spaces.
Gross examination revealed that the tumor contained unencapsulated nodules that were brown-mahogany in color (Figure 2A). Microscopic examination of the tumors of the parotid gland and PPS revealed multiple unencapsulated nodules scattered within the normal salivary gland tissues; these nodules were composed of densely packed uniform and polygonal cells with abundant granular eosinophilic cytoplasm and centrally located uniform nuclei (Figure 2B and C). Nodular oncocytic hyperplasia of the bilateral parotid glands with PPS extension, complicated with recurrent obstructive parotitis, was diagnosed. Since the right parotid gland lesion was benign and nonneoplastic, and the inflammation was mainly on the right side, surgery for the left-side lesions was not performed after discussing with the patient. During the 2 years of follow-up after the surgery, she experienced no recurrence of the right parotid lesion and no progression or inflammation of the left parotid swelling (Figure 3).

Gross examination of the resected specimen revealed multiple unencapsulated and brown-mahogany nodules (A). Hematoxylin–eosin stain of the PPS tumors and parotid tumors both revealed multiple unencapsulated oncocytic nodules scattered within normal parotid gland tissue. (B, original magnification ×40). The nodules are composed of densely packed uniform cells with abundant granular eosinophilic cytoplasm, arranged in an organoid pattern (C, original magnification ×200). PPS indicates parapharyngeal space.
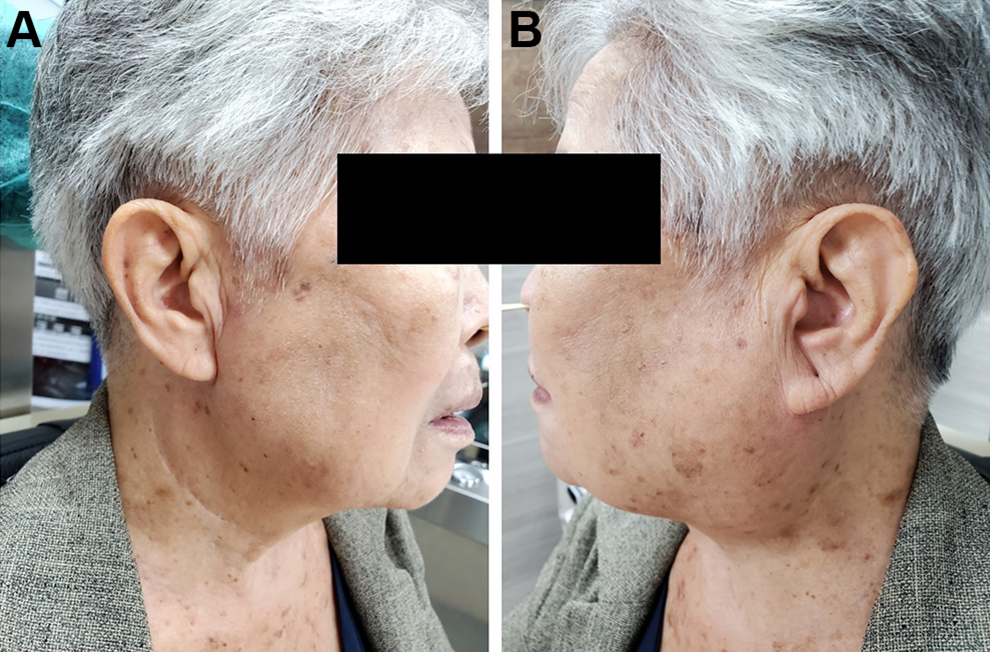
At 2 years postoperatively, no signs of recurrence of the right parotid gland lesions were observed (A), and there was no progression of the left parotid swelling (B).
Discussion
On reviewing the available literature on oncocytic salivary gland neoplasms, it was found that the naming of oncocytic tumors is complex and unclear, particularly oncocytosis. The second edition of the WHO classification of salivary gland neoplasms published in 1991 divided oncocytic lesions into 3 distinct categories: oncocytosis, oncocytoma, and oncocytic carcinoma. 4 Oncocytosis was further divided into diffuse hyperplastic oncocytosis (DHO) and multifocal adenomatous oncocytic hyperplasia (MAOH) or multifocal nodular oncocytic hyperplasia (MNOH). 4 Diffuse hyperplastic oncocytosis is the complete oncocytic metaplasia of acinic and ductal cells, resulting in filling of oncocytes in almost all glands. Multifocal adenomatous oncocytic hyperplasia or MNOH is different from DHO in that it consists of multiple unencapsulated nodular foci of oncocytic cells from ductal epithelium with remnants of the salivary tissue between the oncocytic nodules. 4 The fourth edition of the WHO classification of salivary gland neoplasms released in 2017 changed the classification of oncocytosis to NOH. 2 Synonyms of NOH include MNOH, MAOH, nodular oncocytosis, and clear cell oncocytosis. 2 However, DHO is not described in this edition.
Nodular oncocytic hyperplasia of the parotid gland is extremely rare. Palmer et al analyzed 3500 salivary gland tumors, and only 9 cases of oncocytosis (9/3500, 0.25%) were identified, including 7 MNOH and 2 DHO. 5 To the best of our knowledge, only 11 patients with NOH of the parotid glands have been reported in 10 case reports published between 1999 and 2019 (Table 1).6-15 Of the 12 patients, including ours, there were 9 (75%) females and 3 (25%) males with a median age of 67.9 years (range, 53-80 years). Half of the patients had bilateral lesions. Almost all patients had painless swelling of the parotid region without any symptoms or signs of infection, and only 2 patients, including ours, experienced painful swelling with inflammation. As for the treatment, 9 patients underwent either superficial or total parotidectomy, depending on the tumor’s location, and the remaining 3 underwent biopsy or excisional biopsy for pathologic diagnosis. Of the 3 patients, 2 had their lesions unchanged approximately 2 years after the surgery, and the condition of the other patient was not described in the report.
Overview of Published Cases of Nodular Oncocytic Hyperplasia in the Parotid Glands.
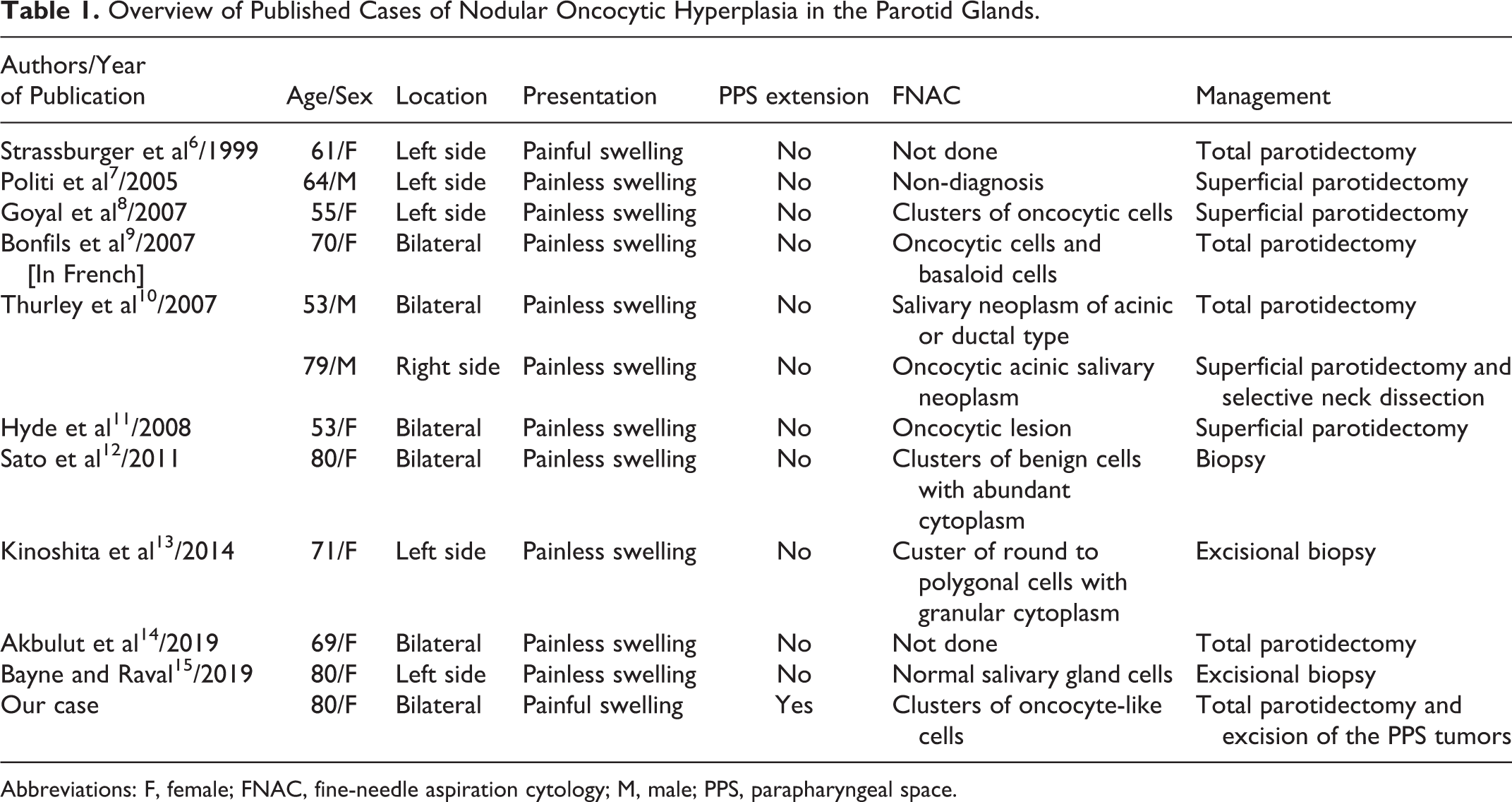
Abbreviations: F, female; FNAC, fine-needle aspiration cytology; M, male; PPS, parapharyngeal space.
Ten of the 12 patients underwent preoperative fine-needle aspiration (FNA); however, FNAC showed oncocytic lesions in only 5 patients. Fine-needle aspiration is often used as a primary screening tool for salivary gland lesions. However, the diagnosis of oncocytic tumors by FNA is less accurate, and the sensitivity is only 29% compared to 90% for other salivary tumors. 1 Rooper et al analyzed the FNAC in 12 cases of NOH identified in 11 patients. 3 Although NOH was listed in the differential diagnosis in only 1 case according to the cytologic findings, they found that FNAC in most cases of oncocytosis revealed a paucicellular specimen comprising small groups of oncocytic cells. These features are generally distinct from those of oncocytic salivary malignancies.
The PPS is an inverted pyramid-shaped deep space extending from the hyoid bone to the skull base. Parapharyngeal space tumors are rare, accounting for only 0.5% of all head and neck tumors. 16 Most PPS tumors (70%-80%) are benign with 40% to 50% of the total tumors originating from the salivary glands, particularly pleomorphic adenomas. The rest are neurogenic tumors (20%), such as schwannomas and neurofibromas, or other miscellaneous tumors. 16 Oncocytic neoplasms occurring in the PPS are relatively uncommon. After reviewing the literature, only a few reports of oncocytomas in the PPS were found; however, no literature reported NOH occurring in the PPS. Barrese et al reviewed the literature in 2009 and found only 5 cases of oncocytoma that occurred in the PPS. 17 In 2010, Tan and Tan reported 3 large oncocytomas in the PPS that were extensions of deep lobe parotid tumors. 18 To the best of our knowledge, our case may be the first report of NOH arising from the parotid gland, in the PPS.
There are 4 basic surgical approaches for excision of the PPS tumors: transoral, transcervical, transparotid, and transmandibular. 19 Due to the risks of significant bleeding and wound infection, the transoral approach is usually not used and is only suitable for small benign extra parotid tumors, especially in the prestyloid compartment. The transcervical approach starts with an incision at the hyoid bone level or approximately 3 cm below the inferior border of the mandible; the incision may extend to the parotid. This approach is preferred for PPS tumors with narrow attachments to the deep lobe of the parotid gland, which can be removed from the surrounding tissues by blunt finger dissection. 19 The transmandibular approach is only used for extensive PPS tumors. This approach involves splitting of the lower lip and a single parasymphysis osteotomy to expose the PPS widely. The transparotid approach is employed for tumors in the deep lobe of the parotid gland. It involves a superficial parotidectomy with identification and preservation of all the branches of the facial nerve. In addition, the combined surgical approach can also be effectively used for extensive PPS tumors. In our patient since multifocal NOH involved both lobes of the parotid gland, a total parotidectomy was indicated. After total parotidectomy, we easily resected the oncocytic nodules in the PPS through the transparotid approach. During our operation, the transparotid approach was combined with the transcervical approach, allowing excellent direct visualization of the PPS tumors and all critical neurovascular structures. Lombardi et al, in 2020, proposed an algorithm for selecting surgical approach to resect PPS lesion. 20 If the planned resection extends toward the upper PPS like our patient, it is recommended to use the transparotid transcervical approach.
Our patient had recurrent parotitis, and NOH of the parotid glands probably has the potential for secondary infection. Although malignant transformation of NOH has not been reported, complete surgical excision is recommended for establishing a histopathological diagnosis. Locally recurrent tumors are rare, but they may be anticipated when partial resection is performed. 21 Owing to the radioresistance of oncocytes, radiotherapy is not indicated, especially with the possibility of radio-induced malignant transformation. 22 The purpose of surgery in our patient was to make a definitive diagnosis, reduce the risks of secondary infection, and alleviate symptoms caused by the compression of the PPS.
In conclusion, when multiple nodules are found in the parotid gland, and FNAC reveals oncocytic lesions, a diagnosis of NOH should be considered, especially in patients aged more than 60 years. Although NOH is usually benign, parotidectomy should be considered if patients have recurrent secondary infection and to ensure histological diagnosis and further follow-up planning. In addition, our case may be the first report of NOH extending from the parotid gland to the PPS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.