
Abstract
Objective
The present study aimed to introduce the surgical method for addressing type II first branchial cleft anomalies (FBCAs) in patients with visible abnormalities lateral to the tympanic membrane.
Design
Retrospective analysis.
Setting
Beijing Children’s Hospital of Capital Medical University from January 2016 to January 2020.
Method
We performed a retrospective analysis of data from patients with type II FBCAs with visible abnormalities lateral to the tympanic membrane. All patients underwent magnetic resonance imaging, (MRI), computed tomography (CT), and otoscopy examinations before surgery. Data regarding the patient’s age, location of the opening, side affected, MRI/CT results, otoscopy findings, the relationship between the lesion and the external auditory canal (EAC), complications, and surgical procedure were recorded.
Results
15 patients with type II FBCAs (Work’s classification) were included in our study. There were 3 different types of visible abnormalities lateral to the tympanic membrane: white masses (Type A), a fibrous band between the tympanic membrane and the EAC floor (Type B), and defects in the inferior wall of the EAC (Type C). Types A and C demonstrated internal fistulas of the FBCA. The roots of the FBCA in all 3 types were deep. Endoscopy was required for complete exposure of the fistula, especially for Types A and C.
Conclusion
Some type II FBCAs patients had visible abnormalities lateral to the tympanic membrane. Otoscope was recommended for routine examination. For these kinds of patients, combined endoscopy during surgery was helpful for reducing the recurrence rate.
Level of Evidence
Level 3.
Keywords
Introduction
Type II (Work’s classification) 1 first branchial cleft anomalies (FBCAs) are described as duplications of the membranous and cartilaginous external auditory canal (EAC), which are difficult to diagnose and treat. FBCAs are congenital disease which account for about 8%–10% of all branchial cleft anomalies. 2
The tract opening in the parotid/neck is below the angle of the mandible and extends toward the inferior part of the EAC. 3 Surgical excision is considered the most appropriate treatment for FBCAs. However, this type of surgery has a high rate of postoperative recurrence rate.
The reason for the high recurrence rate is that the internal fistula was not removed completely. Lots of papers had confirmed that FBCAs had a close relationship with EAC. In other words, abnormal development of the EAC causes FBCAs. So it is very important to recognize if there is some abnormality in the EAC before surgery.
In some patients, physical examination can reveal novel changes and abnormal structures lateral to the tympanic membrane. The tympanic membranes considered a fusion point for the 3 primary vestigial layers of the first branchial apparatus; therefore, abnormal embryologic development in this region often leads to otologic abnormalities. 4 Some patients exhibiting white masses in front of the tympanic membrane are misdiagnosed with congenital cholesteatoma. During surgery, we have observed other structural abnormalities involving the inner opening of the FBCA, which is difficult to expose during traditional surgery due to the depth of the tract. However, endoscopy can aid in detection of the tract. Therefore, in the present retrospective study, we aimed to introduce our experience in treating patients with FBCAs with visible abnormalities lateral to the tympanic membrane utilizing facial nerve monitoring and endoscopy during surgery.
Materials and Methods
Patients
We retrospectively analyzed data from patients with type II FBCAs with visible abnormalities lateral to the tympanic membrane who had undergone surgery at Beijing Children’s Hospital of Capital Medical University from January 2016 to January 2020. The research ethics board of Beijing Children’s Hospital approved the study and waived the requirement for informed consent due to its retrospective nature. Diagnosis of FBCA was made on the basis of clinical evaluation, imaging characteristics, and surgical pathology. We collected data related to the patient’s age, location of the opening, side affected, magnetic resonance imaging (MRI) and computed tomography (CT, window width = 4000 HU, window level = 700 HU) findings, the relationship between the lesion and the external auditory canal (EAC) (otoscopy findings), and complications. The patient with FBCA had undergone surgery before and was excluded for the study. All patients underwent MRI, CT, and otoscopy prior to surgery.
Fifteen patients were divided into groups based on 3 types of abnormalities lateral to the tympanic membrane. Patients with white masses in front of the tympanic membrane were included in the Type A group (Figure 1A). Those with a fibrous band between the tympanic membrane and the EAC floor without secretion were included in the Type B group (Figure 1B). Lastly, those with a defect in the inferior wall of the EAC with purulent secretion were included in the Type C group (Figure 1C). Three types of abnormalities lateral to the tympanic membrane, which were categorized as Types A, B, and C, respectively. Type A: With white masses (asterisk) in front of the tympanic membrane (Panel A). The white mass in front of tympanic membrane was exfoliation of squamous epithelium. Type B: With a fibrous band between the tympanic membrane and the EAC floor (asterisk) without secretion (Panel B). Type C: With a defect (asterisk) in the inferior wall of the EAC with purulent secretion (Panel C).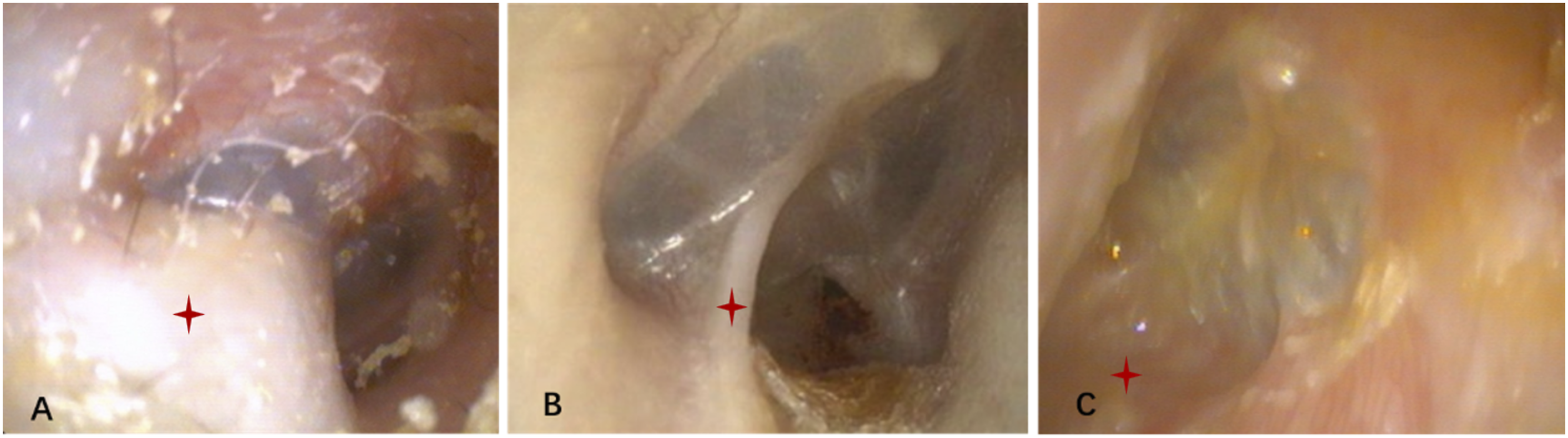
Surgical Procedure
We utilized endoscopy, microscope, and facial nerve monitoring for all patients.
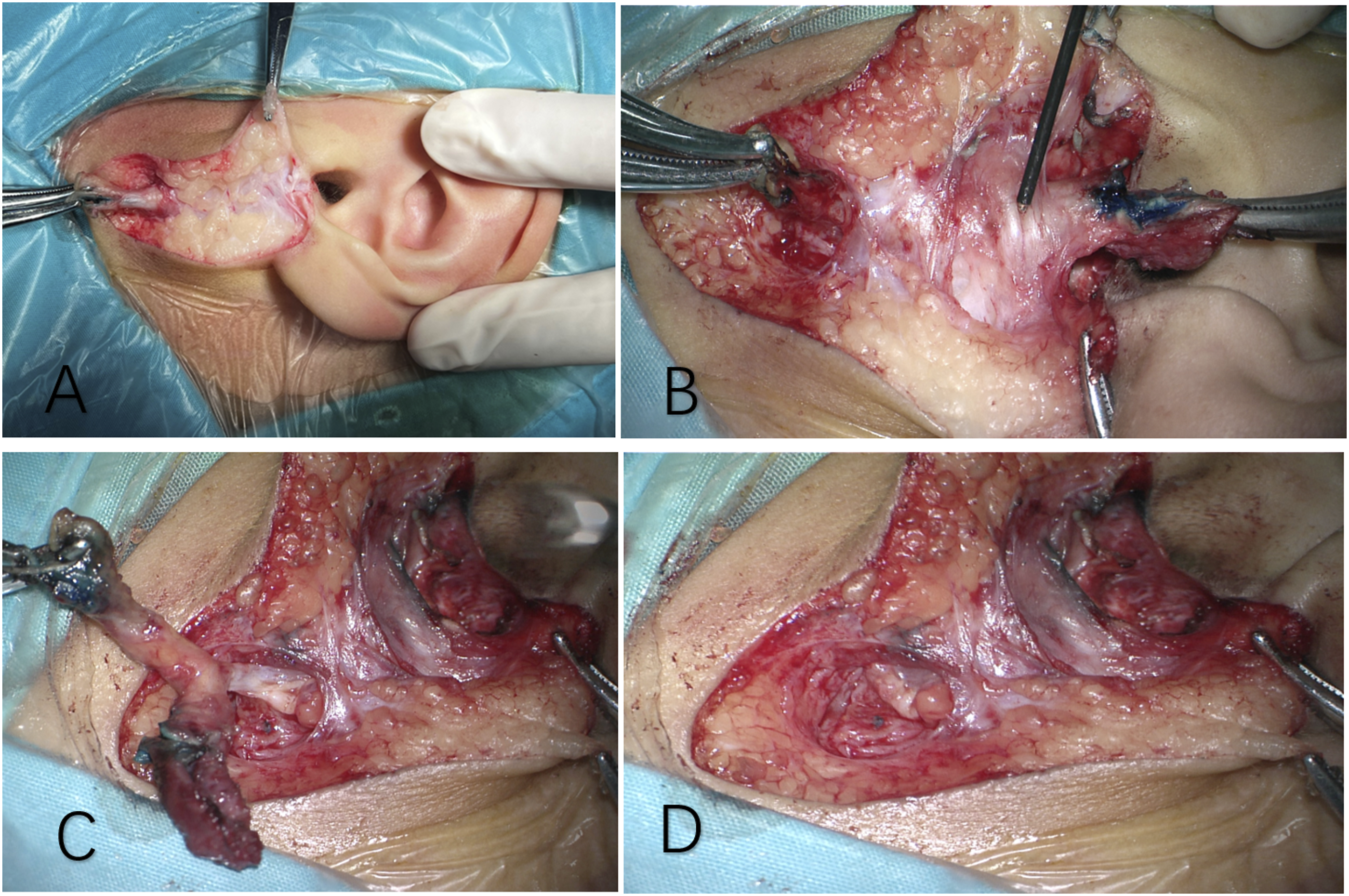
If FBCA locates between the subcutaneous tissue and parotid, the surgical procedure is as follows: 1. Endoscopic examination. To make sure the relationship between abnormalities lateral to the tympanic membrane and the FBCA. If the abnormality is type I or type III, we should resect it under endoscopy to make sure the inner fistula was complete excision. 2. Make a fusiform incision, another straight incision is made from the top of the fusiform incision to the inferior wall of the EAC. Dissect along the fistula (Figure 2A). Manipulate under a microscope and with the help of a facial nerve monitor to recognize the main train of facial nerve at the location of 1–1.5 cm below the earlobe, after separating subcutaneous fat. (Figure 2B) 3. Separate the FBCA and facial nerve (Figure 2C). Complete the excision of FBCA. (Figure 2D) 4. Exploration of the inferior wall of EAC for the second time to make sure that there are no residual lesions. 5. The wound is sutured, and the EAC is stuffed with gauze. The surgical procedure with FBCA located between the subcutaneous tissue and parotid. A: Make a fusiform incision, another straight incision was made from the top of the fusiform incision to the inferior wall of the EAC. Dissect along the fistula. B: Manipulate under a microscope. The facial nerve probe demonstrated the main train of facial nerve. C: Separate FBCA and facial nerve. D: Complete resection of FBCA.
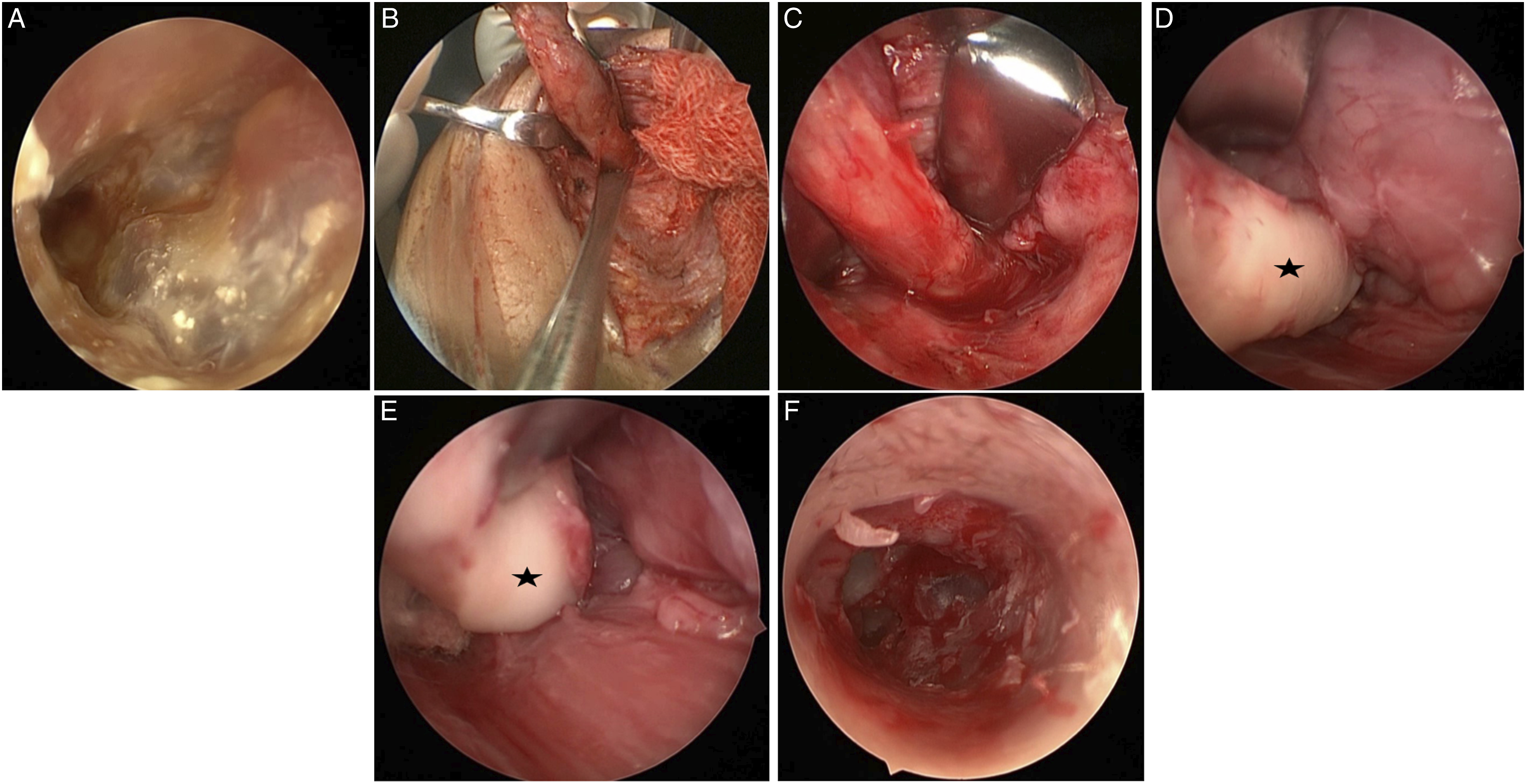
If FBCA locates between the parotid and the carotid sheath, the surgical procedure is as follows: 1. The EAC is observed using a 0°endoscopy. All 15 patients had different types of abnormalities lateral to the tympanic membrane. 2. An incision is made along the abnormal structures (Types A and C) in the EAC to identify the internal fistula of the FBCA. 3. A fusiform incision is made to include the external component of the fistula or sinus. Dissection under a microscope is performed along the lesion, and surgeons attempt to make the wall of the lesion as thin as possible (Figures 3B and 3C). At the root of FBCA, a malformed cartilage could be detected (Figures 3D and 3E). During this step, we should pay attention to the facial nerve, which is recommended using a facial nerve monitor. When dissecting to the EAC, we use a 70° endoscope instead of a microscope to locate the root of the FBCA and the communication between the internal and external fistulae (Figure 3F). 4. The wound is sutured, and the EAC is stuffed with gauze. The surgical procedure with FBCA located between the parotid and the carotid sheath. Pictures showed the endoscopic findings. A: Internal fistula of a first branchial cleft anomaly. B: Dissection along the fistula. C: Manipulate with endoscope. D, E: Dissection until the abnormal cartilage is exposed (asterisk). F: Communication of the internal and external fistula.
Results
Clinical Data
We analyzed the data of 15 patients (5 boys, 10 girls; median age = 4 years; age range = 1–13 years) with type II FBCAs. Lesions were left-sided in 11 patients, while those in the remaining patients were right-sided. Four, 6, and 5 patients were included in the Type A, B, and C groups, respectively.
Patients in the Type A group experienced recurrent neck infection and exhibited white masses in front of the eardrum. Patients in the Type B group also experienced recurrent neck infection, while those in the Type C group presented with chronic otorrhea as well as recurrent neck infections.
The signals of the lesions were hypointense or isointense on T1-weighted MRI, while they were hyperintense on T2-weighted imaging. Figure 4 shows a CT image of a bone defect in the inferior wall of the EAC. All patients with Type A and C abnormalities had bone defects of the EAC. CT scan showing a bone defect of the inferior wall of the external auditory canal (EAC).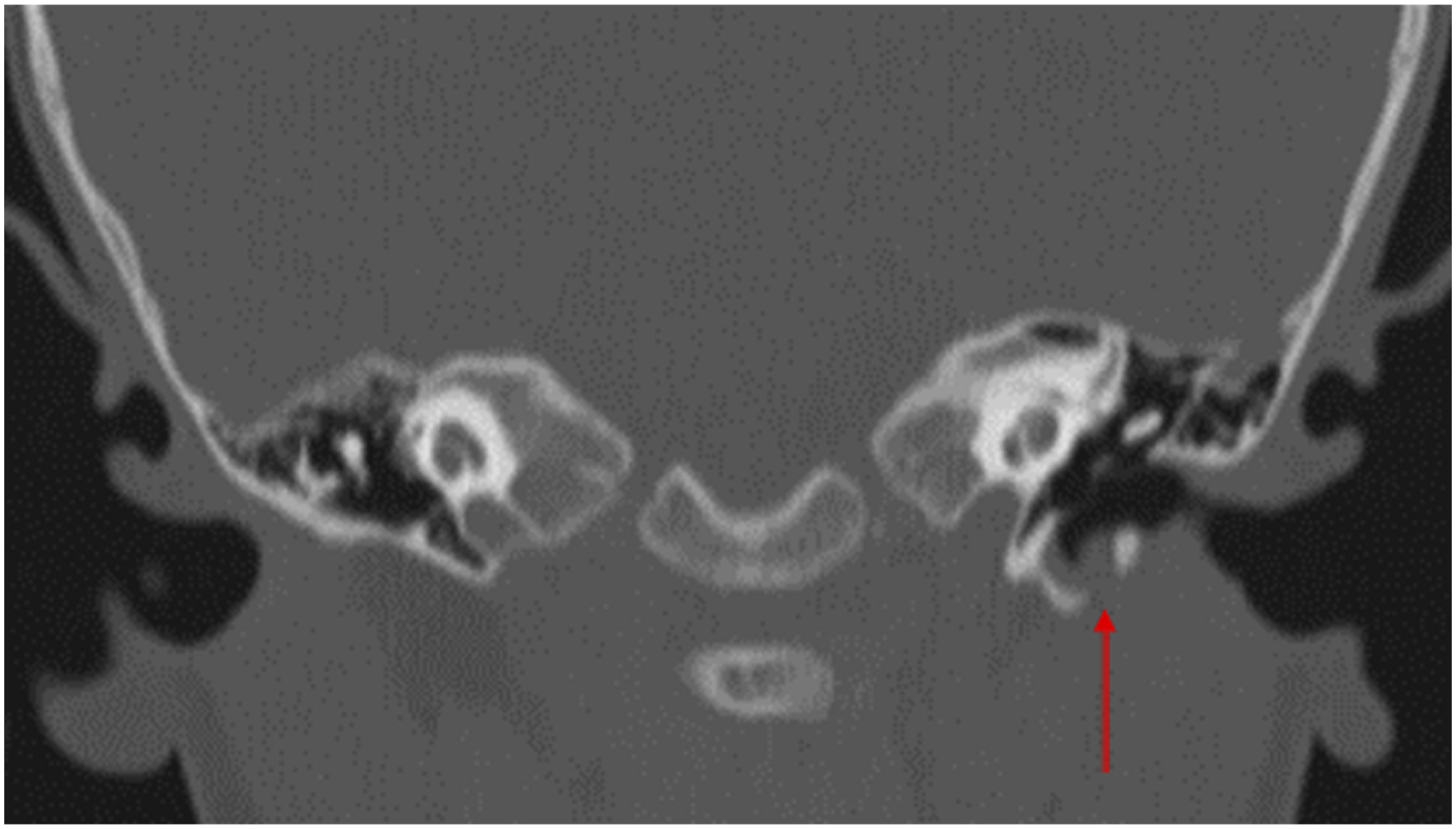
Relationship Between Different Type and Internal Fistulas
Internal fistulas in patients A and C were in the inferior wall of the EAC. Patients in the Type B group did not have internal fistulas. The fibrous band between the tympanic membrane and the EAC floor without secretion was just a blind end. Lesions in 2 of the 15 patients were in the sinus without an external fistula.
Relationship Between FBCA and Facial Nerve
A total of 5 patients (3 type B, 2 type C) occurred at our institution, the main trunk of the facial nerve adhered to the lesion and was located superficial to the FBCA (Figure 2B). Other patients were observed under an endoscope, it demonstrated that there was no obvious adhesion between the lesion and the facial nerve. There was no relationship between the 3 types EAC abnormality of FBCA and facial nerve.
Follow-Up
All 15 patients were followed up for 1–3 years. The was no recurrent case. There were no cases of long-term facial palsy. Two patients experienced temporary facial paralysis. They recovered postoperatively within 7 days following treatment with dexamethasone.
Discussion
First branchial cleft anomalies are a rare disease that arises due to incomplete closure of the ventral portion of the first and second branchial arches. Work 1 divided FBCAs into types I and II according to the anatomical and histological features of the lesion. Type I FBCAs are defined as cystic masses in the postauricular area extending medially and anteriorly along the EAC. Type II FBCAs frequently present with a fistula below the earlobe in the upper neck, which communicates with a sinus tract that extends medial or inferior to the EAC. 5
The development of the EAC is also determined by the first and second branchial arches. 6 As a result, FBCAs exhibit a close relationship with the EAC and have been described as duplications of membranous and cartilaginous EAC. As a result, endoscopy examination was recommended for all FBCAs patients as a routine. In the present study, we identified 3 different types of EAC duplications. Type A duplications presented as white masses lateral to the tympanic membrane, which can be misdiagnosed as congenital cholesteatoma. Some patients experienced hearing screening failed without any other symptom. Type C duplications represented another type of inferior wall defect in the EAC. Patients with such defects often experienced chronic otorrhea. While both types were characterized by an FBCA with an internal fistula, no internal fistulae were observed in patients with Type B abnormalities. Rather, such abnormalities presented as a fibrous band extends to tympanic membrane that did not exhibit secretory functions, similar to an atretic membranous EAC. However, regardless of the type, all lesions were characterized by long and deep routes.
Magnetic resonance imaging is regarded as the best choice for diagnosis, as it may allow surgeons to determine the relationship between the lesion, parotid gland, and EAC and aid in surgical planning. In the current study, additional CT imaging revealed bone defects in the inferior wall of the EAC in some patients, representing the root of the lesion. Inadequate exposure can make addressing deep lesions of the inferior wall of the EAC challenging, especially in patients whose inferior wall defects are located deep within the EAC. Failure to adequately address the otologic component of the lesion can result in persistent infection and misdiagnosis. 2 Therefore, we also recommended performing endoscopic examination and CT in patients with abnormal structures in front of the eardrum.
Surgical excision is the best choice for treating FBCAs. The traditional surgical method involves partial parotidectomy, in which the facial nerve is completely dissected. 7 Zhang et al. 8 recommended performing surgery with the help of a microscope. Microscope combined with facial nerve monitor can help us better identifying the facial nerve. However, for patients with Type A and C structures lateral to the tympanic membrane, because of long depth and angle of the lesion, with the help of endoscopy, the internal fistula could be exposed better.
Our novel approach using an endoscope involves 2 essential points during surgery. First, to account for the long path and special angle of the fistula or sinus, extracapsular resection is performed rather than partial parotidectomy. Second, the procedure utilizes 0°and 70° endoscopes for a combined approach to expose the lesion in the EAC and external fistula. Normally, we observed that the root of the fistula exhibited abnormal hyperplasia of the cartilaginous components (Figure 3C). These abnormal components should be resected to completely expose the internal fistula. Our study also has some defects. The study design was case series with chart review. In future studies, we will design a randomized controlled trial for further comparison of the surgical treatment between traditional surgery and combined endoscopy surgery in patients with type II FBCAs.
Conclusion
First branchial cleft anomalies patients were recommended getting EAC examination before surgery. Combined endoscopy can simplify surgical treatment of type II FBCAs in patients with lateral to the tympanic membrane by allowing for complete resection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Beijing Hospital Authority’s Ascent Plan, DFL20191201.