
Abstract
This case report introduces a novel surgical procedure to occlude the lateral semicircular canal through the external auditory canal. The patient was a 64-year-old male with Ménière’s disease who had suffered from left ear vertigo accompanied by tinnitus for more than 4 years. He also suffered from paroxysmal vertigo, fluctuating hearing loss, tinnitus symptoms, and ear distension and tightness. The patient had been treated with dexamethasone injected into the tympanic cavity for 1 year, but his condition often recurred and could not be controlled. We developed a novel procedure using an endoscope to occlude the lateral semicircular canal through the external auditory canal to provide a surgical option for the treatment of Ménière's disease.
Introduction
Ménière's disease is characterized by recurrent rotary vertigo, fluctuating sensorineural hearing loss, and tinnitus with (or without) ear fullness, which seriously affects a patient’s quality of life.1,2 Currently, thiazide diuretics and micropressure pulse therapy apparatus are the first-line options for the treatment of Ménière's disease, and steroid hormone injections into the drum cavity is the second-line treatment. In addition, gentamicin injected into the tympanic cavity is the transitional plan between second-line treatment and third-line surgical treatment. There is a consensus that patients with intractable Ménière's disease for whom conservative treatment has proved ineffective be reassigned to surgery. The conventional theory is that the pathogenesis of Ménière's disease is caused by endolymphatic hydrops. 3 Therefore, endolymphatic sac decompression, vestibular nerve transection, labyrinthine resection, semicircular canal occlusion, and endolymphatic catheter clipping are common surgical methods for clinical treatment of Ménière's disease. 4 Herein, we introduce a novel surgical procedure to occlude the lateral semicircular canal through the external auditory canal.
Case Presentation
Case Background
A 64-year-old male patient with Ménière's disease presented at our clinic. He had suffered left ear vertigo accompanied by persistent tinnitus of the left ear for more than 4 years. The patient had paroxysmal vertigo, fluctuating hearing loss, tinnitus symptoms, and ear distension and tightness. There was no history of ear canal abscess, headache, walking instability, facial paralysis, or other accompanying discomfort. According to the hearing test results, the left ear had no useful hearing. The right ear had better hearing than the left ear, and the average decibel hearing level was approximately 38 dB, which was considered to be mild to moderate hearing loss, but the hearing loss was greater at 4000 and 8000 Hz. Temporal bone computed tomography showed that the bilateral external auditory canals were unobstructed, the bilateral middle ear tympanum and mastoid sinus cavities were clear, bilateral auditory ossicles were not obviously abnormal, and the left maxillary sinus had a little sinusitis. The patient had received dexamethasone injection into the tympanic cavity for 1 year, but his condition often recurred uncontrollably, and consequently, the patient resorted to surgical treatment to control his vertigo attacks.
Procedures of the Surgical Intervention
We followed regular preparation procedures for otoscopic surgery according to the specifications and standardized surgical procedures as follows: (1) the external auditory canal was cleaned with normal saline (Figure 1A). (2) Lidocaine epinephrine was injected under the skin of the external auditory canal to reduce possible hemorrhaging caused by preparation of an external auditory canal tympanic membrane flap (Figure. 1B). (3) A tympanic membrane U-shaped skin flap larger than 180° was created from the 3-o’clock direction of the external auditory canal (Figure 1C and D), severing the malleus–incus joint in the process. During the operation, the tympanic cord nerve and malleus handle were carefully protected. (4) Next, a curette was used to scrape the bone on the outer wall of the upper drum (Figure 1E). (5) Using a U-shaped osteotome, the depression of the outer side wall of the upper drum created by the curette was enlarged (Figure 1F) to expose a sufficient field of view of the middle ear cavity. (6) The plica and mucosa on the surface of the manubrium of the malleus were removed, exposing the incudostapedial joint, and then the joint between the incus and the stapes was cut (Figure 1G). (7) The incus was removed (Figure 1H). (8) Curettes were used to continue scraping part of the bone in the inferior wall of the attic so that the endoscopic field of vision covered the inferior tympanum and the posterior tympanum (Figure 1I). (9) The lateral semicircular canal was exposed, using an electric drill to grind out part of the semicircular canal bone to form a window (Figure 1J and K), taking care to avoid damaging the membranous semicircular canal. (10) The foramen of the semicircular canal was enlarged with the needle tip of a hook needle to expose the membranous semicircular canal (Figure 1L and M and Figure 2A and B). (11) After the membranous semicircular canal was identified, it was filled with subcutaneous tissue from the external auditory canal (Figure 1N and 2C and D), and the membranous semicircular canal was pressed against the bone wall opposite the window hole to completely block it. (12) Bone wax was used to seal the semicircular canal, and its periphery was glued with biological glue to prevent extralymphatic leakage (Figure 1O). (13) Using bio-glue, the incus was connected to the incudostapedial joint and the position of the incus bone was restored (Figure 1P). (14) The tissue defect of the lateral wall of the supratympanic cavity was repaired with subcutaneous tissue and the bone defect of the inferior wall of the supratympanic cavity was repaired with a small piece of cartilage (Figure 1Q and R). (15) Finally, the external auditory canal flap was replaced (Figure 1S).
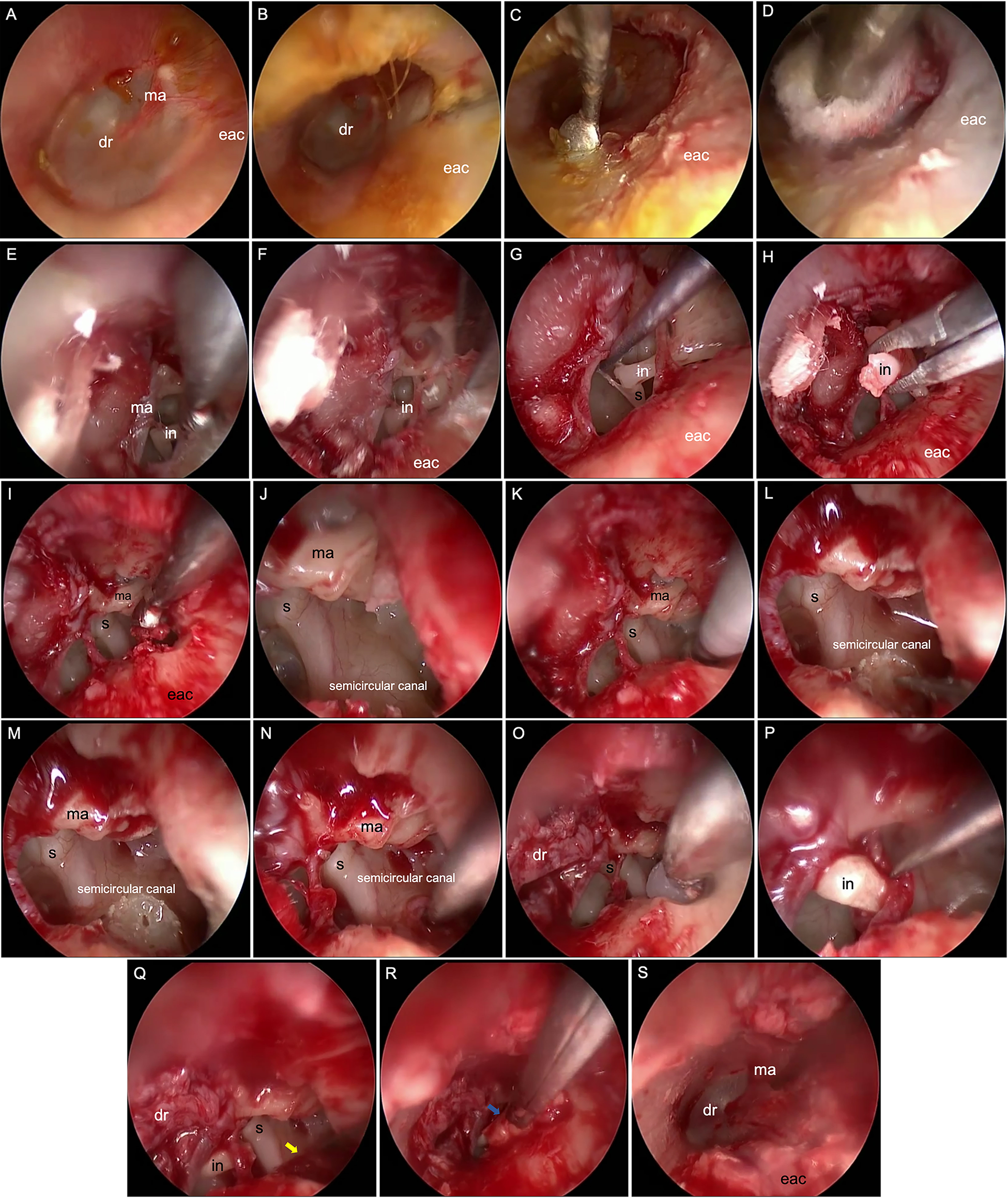
Surgical steps 1 to 15. A, Cleaning the external auditory canal. B, Injecting lidocaine epinephrine under the skin of the external auditory canal. C, Creating a tympanic membrane U-shaped flap. D, Lifting the tympanic membrane flap. E, Scraping the bone of the outer side wall of the upper drum. F, Expanding the outer side wall of the upper drum. G, Severing the joint between the incus and the stapes. H, Removing the incus. I, Grinding out part of the bone in the inferior wall of the attic. J, Exposing the lateral semicircular canal. K, Grinding out part of the semicircular canal bone. L, Using a needle tip to enlarge the semicircular canal. M, Exposing the membranous semicircular canal. N, Using subcutaneous tissue from the external auditory canal to fill the membrane semicircular canal. O, Using bone wax to seal the semicircular canal. P, Resetting the incus. Q, Covering the semicircular canal with subcutaneous tissue (indicated by the yellow arrow). R, Repairing the inferior wall of the attic with a small piece of cartilage (indicated by the blue arrow). S, Resetting the tympanic membrane flap. dr indicates drum; eac, external auditory canal; in: incus; ma, malleus; s, stapes.
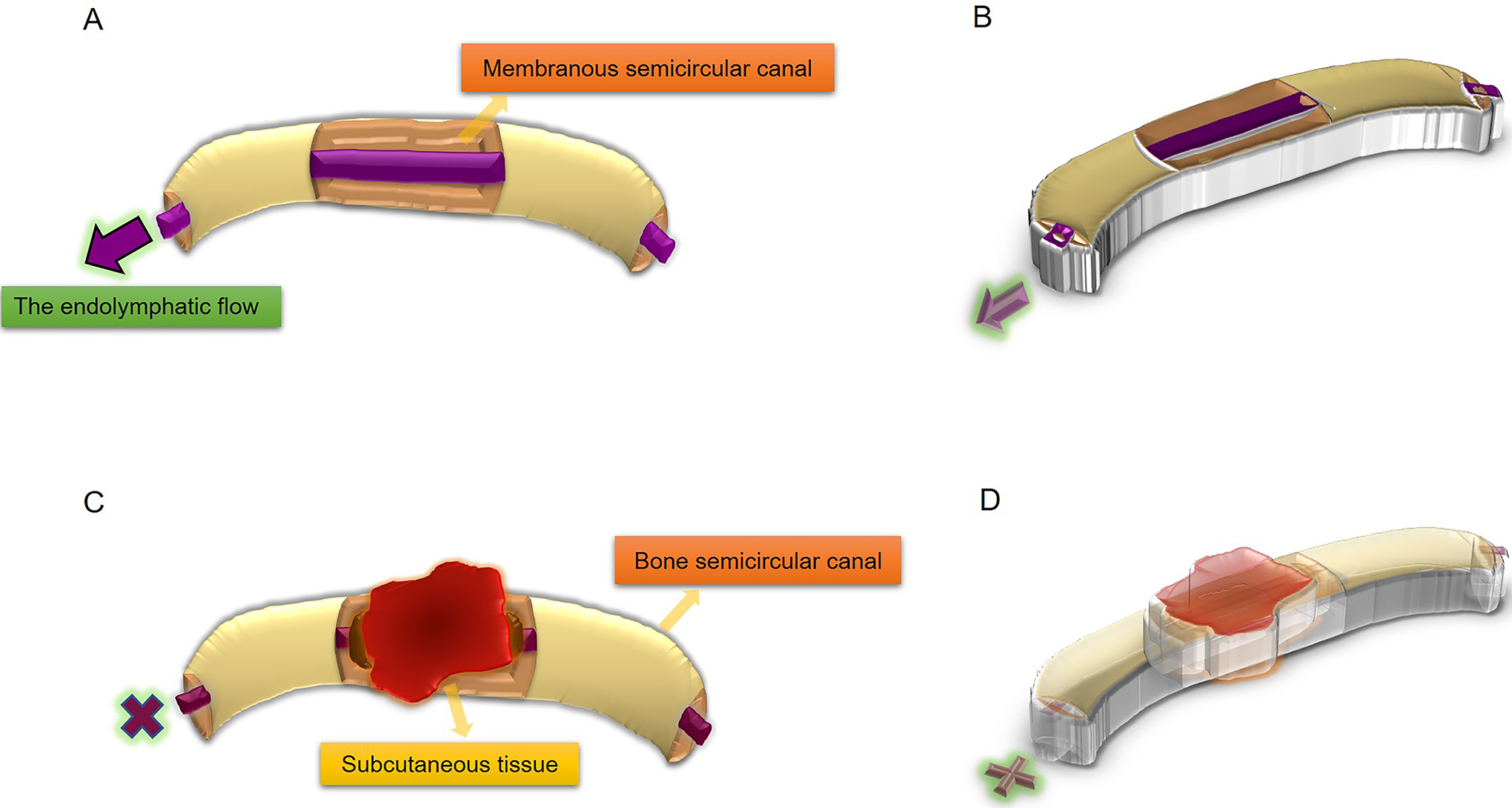
Schematic diagram of the operation principle. A, Sagittal plane of the lateral semicircular canal. In order to expose the membranous semicircular canal, part of the bone semicircular canal is ground out, and the purple arrow indicates the direction of lymph flow. B, Horizontal plane of the lateral semicircular canal. C, Subcutaneous tissue is used to plug the membranous semicircular canal; the purple cross indicates that endolymphatic flow is blocked. D, Horizontal plane of the lateral semicircular canal.
Postoperative Care and Follow-Up
The patient received vestibular rehabilitation treatment for 6 months after surgery. Regular follow-up showed that the patient’s recovery was ideal, and there were no recurrent attacks of vertigo or tinnitus, no serious complications, and the patient’s life quality was improved.
Ethical Approval
Approval was given by the ethics committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, China (approval No. 2020-0352).
Discussion
At present, conventional surgery for semicircular canal occlusion is to block endolymphatic flow with bone wax, bone debris, fascia, bio-gel, or using a laser after opening a window in the semicircular canal bone. The operation involves microscopic incision of the posterior auricular skin, exposing and opening the mastoid, contouring the mastoid, finding the posterior semicircular canal, and attempting to block it. 5 Anthony 6 used an argon laser to perform semicircular canal fenestration and occlusion. The aim of this procedure is to cauterize the bone semicircular canal, and its thermal effect causes local fibrosis and occlusion of the membranous semicircular canal, thus reducing endolymphatic flow. There is the possibility of incomplete occlusion of the semicircular canal. 6 Kartush and Sargent 7 used a CO2 laser to perform semicircular canal fenestration and occlusion. After the semicircular canal bone was removed with an electric drill to form a window, the CO2 laser was used to directly cauterize the membranous labyrinth, thus shrinking and occluding the membranous semicircular canal. This method can not only quickly and completely block the membranous semicircular canal during the operation but also reduce the risk of perforation of the membranous semicircular canal and endolymphatic leakage and reduce the possibility of labyrinthine trauma and sensorineural deafness after the operation. 7 All of the above operations are carried out under a microscope. Incisions need to be made behind the ear. Due to the need to grind away a large amount of bone, patients have a greater reaction, including pain and long-term numbness. To the best of our knowledge, we are the first to use endoscopy to enter the middle ear canal and block the lateral semicircular canal. Using this technique, there is no need to make a posterior auricular incision or grind away a large amount of mastoid bone. It is suitable for patients with vertigo, those with Ménière's disease who have experienced no obvious curative effect after 6 months of standardized medical diagnosis and treatment, patients without practical hearing, and patients without contraindications to surgery. This procedure uses an endoscope to conduct vertigo surgery and is more acceptable to patients, requires no head dressing, and causes less postoperative pain. The path through the external auditory canal is characterized by minimal invasion, no incision, and quick recovery. Moreover, the indications of this method are the same as those of traditional surgical methods. However, more cases are needed to evaluate the clinical cure rate and effect on prognosis.
Conclusion
Herein, we introduce a novel surgical procedure to occlude the lateral semicircular canal through the external auditory canal. This procedure is the first to apply an endoscope to occlude the lateral semicircular canal through the external auditory canal to provide a surgical option for the treatment of Ménière's disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (NSFC) [Grant numbers 81771003, 81570923].