
Abstract
Transcanal endoscopic ear surgery is a minimally invasive procedure that allows a clear visualization of the middle ear. Recently, indications for endoscopic surgery have been expanding. We performed combined underwater endoscopic and microscopic surgery for external auditory canal cholesteatoma, the computer tomography of which indicates the possibility of cholesteatoma not only in the canal wall but also in the mastoid. The 30° endoscope and underwater technique makes the surgical view clear, and we could remove the cholesteatoma without canalplasty. To the best of our knowledge, no case of external auditory canal cholesteatoma treated with underwater endoscopic and microscopic surgery has been previously reported. This case indicates that the procedure could be a good indication for external auditory canal cholesteatoma.
Introduction
Transcanal endoscopic ear surgery (TEES) is a minimally invasive procedure that allows a clear visualization of the middle ear. Recently, indications for endoscopic surgery are expanding. Previous reports suggested that TEES is also a good indicator for external auditory canal cholesteatoma.1,2 One of the problems during endoscopic surgery is that the visibility worsens due to bone dust and blood. Previous reports show that underwater endoscopic ear surgery solves these problems during middle ear surgery.3-6
We performed combined underwater endoscopic and microscopic surgery for external auditory canal cholesteatoma, the computer tomography (CT) of which indicates the possibility of cholesteatoma not only in the canal wall but also in the mastoid.
Case report
A 38-year-old woman consulted an otolaryngologist with a frequent history of otorrhea in the right ear. She had no history of surgical intervention, such as tympanoplasty or canalplasty. After being diagnosed with a possible external auditory canal cholesteatoma, she was transferred to our department.
Clinical examination on presentation revealed a small perforation in the right middle posterior wall of the external auditory canal (Figure 1A). Her pure tone audiometry was within normal limits. Computed tomography revealed erosion and perforation in the right external auditory canal and small soft tissue shadow in the right mastoid (Figure 1B), which indicated a possibility of cholesteatoma. (A) Retraction and perforation in the right middle posterior extra auditory canal. The lesion could not be observed by microscope, but it could be observed with an endoscope. (B) Preoperative computed tomography image. It shows a destructive lesion in the right posterior wall and low-density area in mastoid.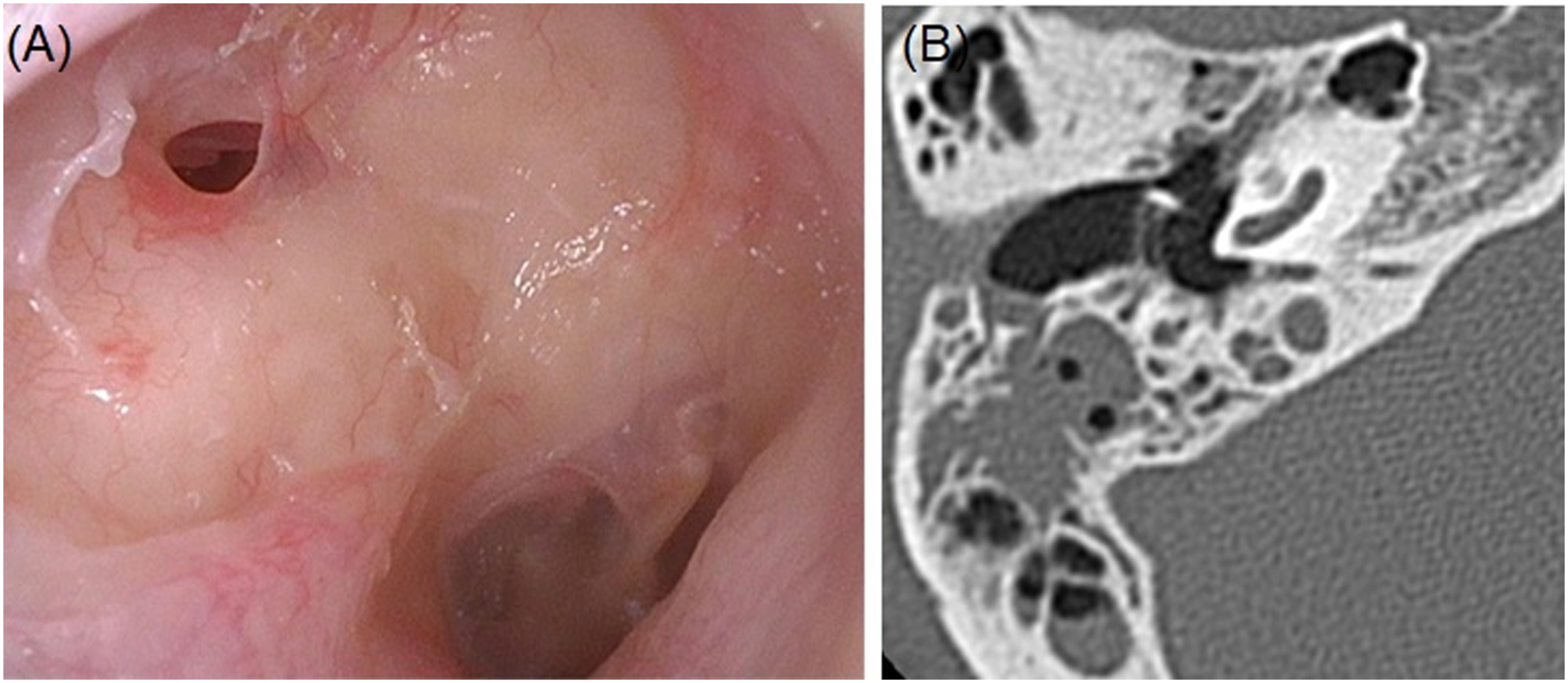
Then, we planned a combined underwater endoscopic and microscopic surgery for external auditory canal cholesteatoma. Using a general anesthesia, a postauricular skin incision was accomplished during surgical intervention. Fortunately, no cholesteatoma was found throughout canal wall up mastoidectomy. Since the bottom of cholesteatoma could not be visualized by microscope (Figure 2A), we tried to remove the extra auditory canal cholesteatoma with an underwater endoscopy technique. We used a 2.7-mm diameter, 18-cm length, 30° endoscope. While removing the cholesteatoma, saline solutions were refluxed with a 50-cc syringe by an assistant (Figure 2B–D). (A) The bottom of cholesteatoma not visualized via microscopic view. (B) Although the 30°-endoscope visualized the bottom of cholesteatoma, the blood and fog disturbed clear view. (C) The underwater technique gives a clear view by washing blood and dust. (D) The extra auditory canal cholesteatoma was resected.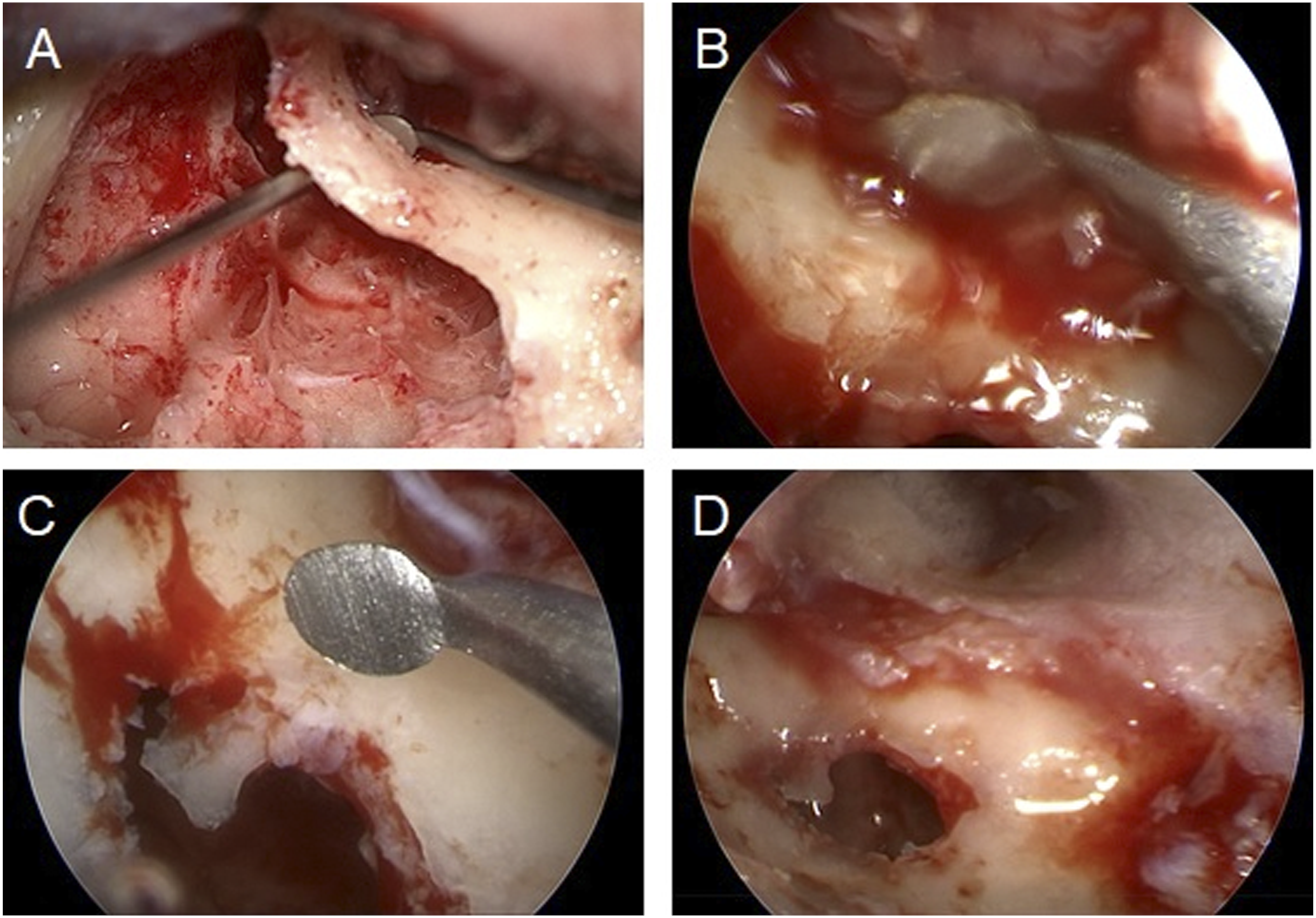
After the extra auditory canal cholesteatoma was resected, the canal wall was reconstructed with bone pate, auricular cartilage, and temporal fascia using fibrin glue. The patient’s postsurgical clinical course was unremarkable, with facial nerve palsy or reperforation. After 3 months upon completion of the procedure, the right ear canal had dried.
Discussion
To the best of our knowledge, no case combining underwater endoscopic and microscopic surgery for external auditory canal cholesteatoma has been reported yet. In the late 1990s, as endoscopic middle ear surgery became more popular, 7 a novel procedure detailed by Yamauchi et al as underwater endoscopic ear surgery was suggested in repairing the superior canal dehiscence and labyrinthine fistulas with positive outcomes and has the benefits of preserving of the inner ear activity and providing clear operative view.3,4 Chen et al. reported the advantage of transcanal underwater endoscopic ear surgery to eliminate cholesteatoma that expands into the mastoid cavity. 5 Nishiike et al. reported a novel endoscopic hydromastoidectomy technique for TEES using a lens cleaning system. 6 In our case, underwater procedure was used at key points during the surgery according to the method already reported by Yamauchi. The tip of the endoscope is completely immersed under the surface of the saline solution, and the assistant continuously perfuses it using a syringe.2,3 This method is simple and inexpensive and can be performed at any facility. We have already reported the advantage of underwater ear surgery on cholesteatoma with a dehiscent high jugular bulb. 8 These underwater procedures kept a clear view by flushing out blood and dust (bone or tissue) from the operative site. Dähn et al. reported the value of transcanal endoscopic surgery for external ear canal cholesteatoma up to Naim stage III.1 Our case was stage III external cholesteatoma placed on the middle posterior wall. The bottom of cholesteatoma, which made the bony wall perforated, was not well visualized via microscopic view although we tried to angle the microscope. The canalplasty which has a risk of mastoid cell exposure would be required to widen a narrowed external auditory canal to enhance access and visualize for the bottom of the extra auditory canal cholesteatoma in the case of microscopic surgery. The 30° endoscope and underwater technique makes the surgical view clear, and we could remove the cholesteatoma without canalplasty. We also performed canal wall down mastoidectomy with a microscope as a combined approach because preoperative CT shows a low-density area in the mastoid cavity, which cannot exclude the possibility of cholesteatoma.
We present a case of combined underwater endoscopic and microscopic surgery for external auditory canal cholesteatoma. To the best of our knowledge, no case of external auditory canal cholesteatoma treated with underwater endoscopic and microscopic surgery has been previously reported. This case indicates that the procedure could be a good indication for external auditory canal cholesteatoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number 18K16857