
Abstract
Introduction
Hemangiomas are benign tumors originating in the vascular tissue of the skin, mucosa, muscles, glands, or bones. 1 Lobular capillary hemangioma (LCH), also known as pyogenic granuloma or granuloma gravidarum, is a rapidly growing lesion with extensive endothelial proliferation. This lesion typically appears in the oral cavity and is rarely found in the nasal region. 2 The etiology of LCH during pregnancy remains unclear. The most widely accepted hypothesis is that this lesion may be the result of the interaction between local irritants and a subsequent tissue inflammatory response enhanced by female sex hormones produced during pregnancy. 3 LCH resolves mostly after delivery and endoscopic endonasal total excision surgery is usually the definitive treatment. 4 Although there are several reports of oral LCH during pregnancy, clinical information of pregnant patients with nasal LCH is not completely understood. Therefore, we performed a systematic review of published cases of nasal LCH in pregnant patients.
Case Report
A 32-year-old woman (gravida 3, para 2) with a twin pregnancy of 33 weeks and mild preeclampsia was referred to the otolaryngology service by a 2 week history of a fast-growing tumor that completely obliterates the left nostril, intermittent moderate epistaxis, and fetid rhinorrhea (Figure 1a). No previous history of nasal trauma or infectious processes was reported. Rhinoscopy revealed a brown-grayish mass with well-defined borders, occupying the left nasal vestibule and provoking right septal deviation without evidence of active epistaxis. Magnetic resonance imaging (MRI) showed a well-defined soft tissue mass in the left nostril extending from the middle turbinate to the vestibule and displacement of the nasal septum to the right, without infiltration of the adjacent nasal tissue (Figure 1b). Noncontrast T1-weighted MRI images revealed an isointense mass, which was hyperintense on the T2-weighted sequence. One week later, cesarean delivery was performed and both fetuses were viable. Two days later, the patient presented a new episode of epistaxis and, due to decreased level of hemoglobin (6.9 mg/dL), 2 globular packets were transfused. At this time, a contrasted computed tomography scan showed a well-defined mass filling the anterior part of the left nasal cavity. No bony erosion was detected, suggesting a benign process. One week after delivery, surgical excision through nasal endoscopic surgery was performed. An irregular, dark red, mobile, and nonpulsatile mass of 5 cm × 3.4 cm was found. This mass was depending on the Cottle’s area III in the nasal septum. Histopathological examination revealed a hypervascularized tumor composed of small thin-walled channels (capillary type), which anastomose and generate a discreetly lobular pattern. It contained areas of recent necrosis, abundant polymorphonuclear cells, lymphocytes, and plasmocytes immersed in abundant myxoid and collagenous stroma (Figure 1c). The patient had a favorable postoperative evolution, and 2 weeks after surgery, there is no evidence of recurrence of the tumor.
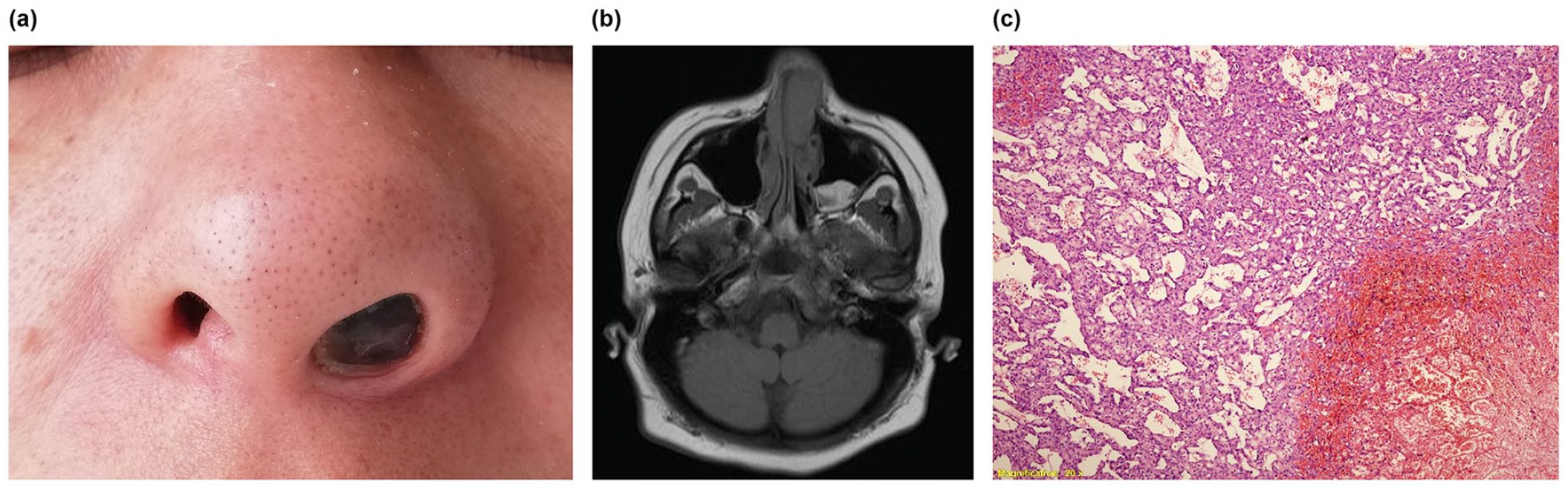
Characteristics of lobular capillary hemangioma of our case report: (a) the external appearance revealed a prominent left nostril, (b) the preoperative magnetic resonance imaging showed a mass occupying the left nasal cavity with displacement of the nasal septum to the right, and (c) the histopathological examination showed numerous small thin-walled channels, areas of necrosis, and inflammatory cells surrounded by abundant stroma (×20).
Methods
This review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 5
Search Strategy
We searched in the following electronic database: PubMed, Embase, Scopus, Web of Science, and LILACS. The search was performed from inception to September 7, 2020, with an update until June 30, 2022. The complete search strategy is available in Supplemental Table S1. There were no restrictions on language or publication date. We also conducted a hand search of reference lists of all included articles and relevant reviews to identify additional studies.
Eligibility Criteria
We included studies involving adult pregnant patients (≥18 years old) with based on the clinical and/or histopathological criteria. Editorials, abstracts, commentaries, systematic reviews, and narrative reviews were excluded.
Study Selection
We downloaded all articles to EndNote X8 software (Clarivate, Philadelphia, PA, USA) and duplicate records were removed. Titles and abstracts were independently screened by 2 review authors (YLB and CDA) to identify relevant studies. Likewise, the same review authors independently assessed the full text of each eligible study and registered reasons for the exclusion. Any disagreement on title/abstract and full-text selection was resolved by consensus.
Data Extraction
The information from each included article was independently extracted by 2 review authors (YLB and CDA) using a standardized data extraction form. Any disagreement was resolved by consensus. If additional data were needed, the corresponding author was contacted through email. The following data were extracted: first author name, publication year, country, study design, sample size, age, sex, comorbidities, clinical features, characteristics of the lesion, imaging findings, treatment, and recurrence. Studies published in languages other than English were included if the article could be translated with Google Translate.
Statistical Analysis
Frequencies and proportions were used to summarize categorical variables. Means ± standard deviations or median (interquartile range) were used for continuous variables. All analyses were performed using R 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study Selection
Our electronic search retrieved 928 articles. After the removal of duplicates, 405 articles were screened by title/abstract, and of those, 360 articles were excluded. After full-text assessment of 45 remaining articles, 22 were excluded: without full text (22) and other populations (22). Finally, 23 articles2-4,6-25 (20 case reports and 3 case series) were selected (Figure 2).
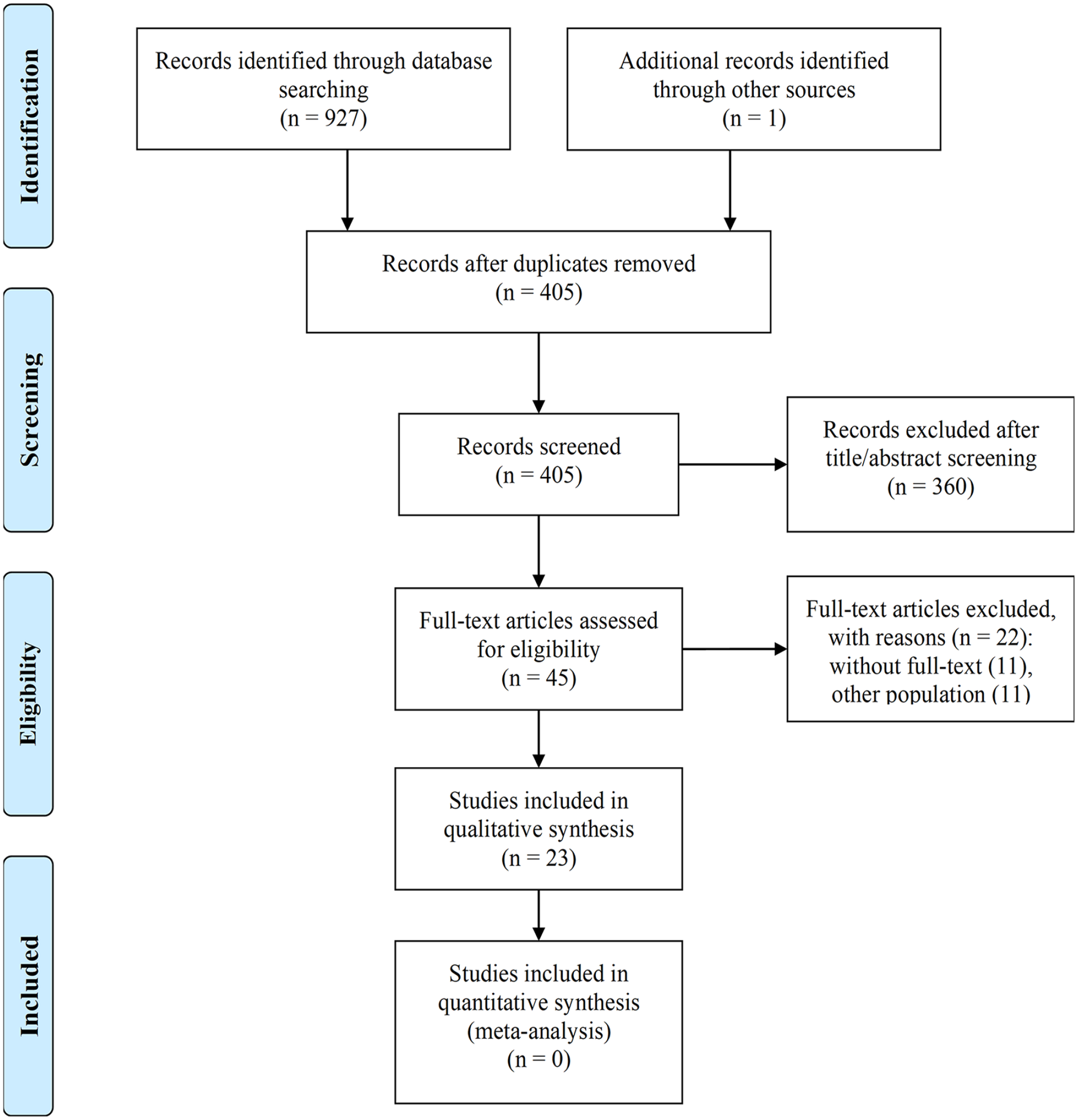
Flow diagram of study selection.
Demographics and Clinical Features
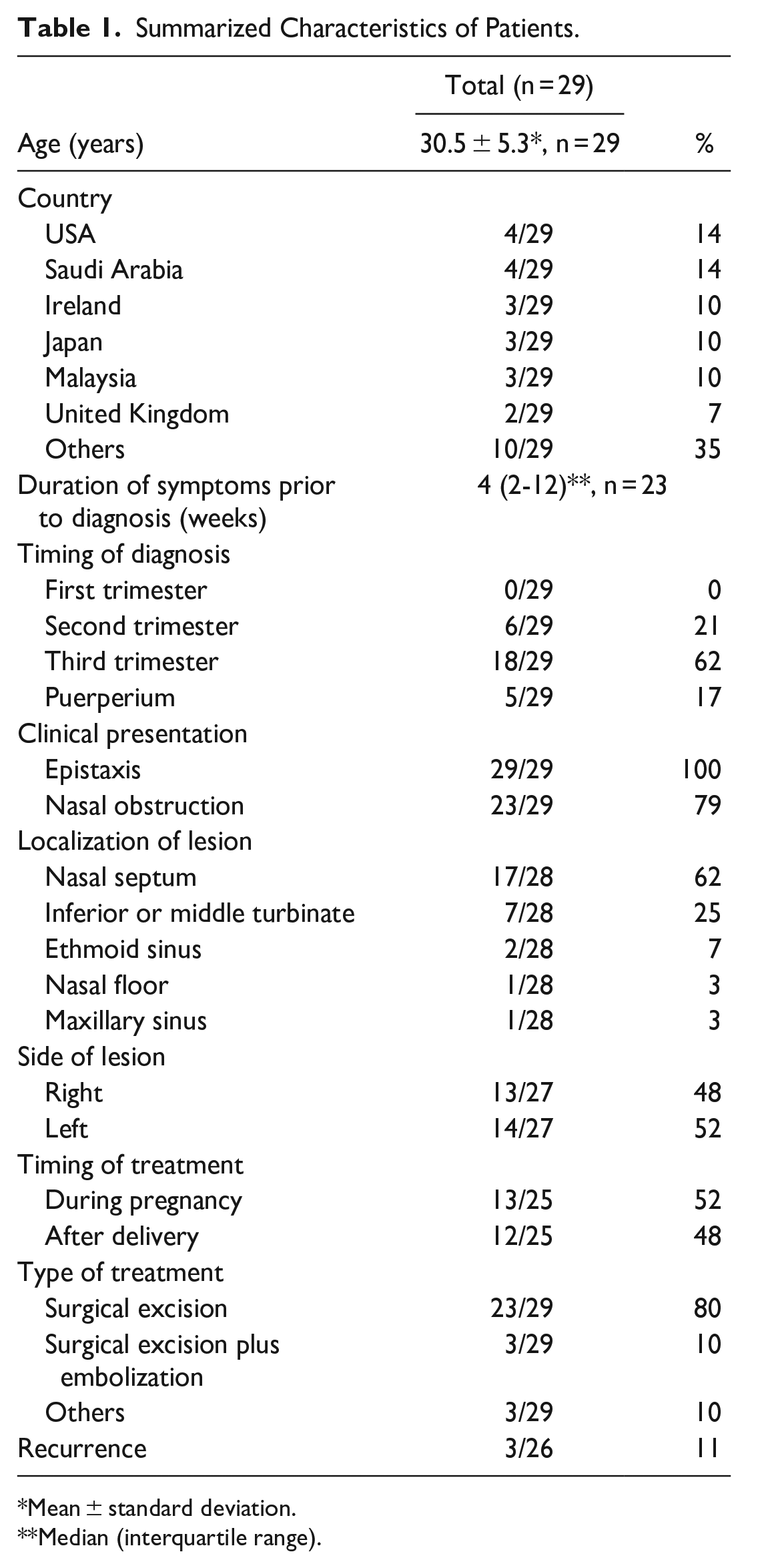
A total of 29 pregnant patients with nasal LCH (including our case report) were included (Tables 1 and 2). The mean age was 30.5 ± 5.3 years. Most cases were from the United States (14%) and Saudi Arabia (14%). Twenty out of 23 patients reported no comorbidities. The median duration of symptoms prior to diagnosis of nasal LHC was 4 (2-12) weeks. The majority of patients (62%) were diagnosed in the third trimester of pregnancy and all cases presented with epistaxis. Laterality of the nasal LCH was split essentially evenly between left and right sides (48% vs 52%, respectively). The nasal septum and inferior or middle turbinate were the most common locations of the lesions (87%).
Summarized Characteristics of Patients.
Mean ± standard deviation.
Median (interquartile range).
Case Reports of Lobular Capillary Hemangioma During Pregnancy.
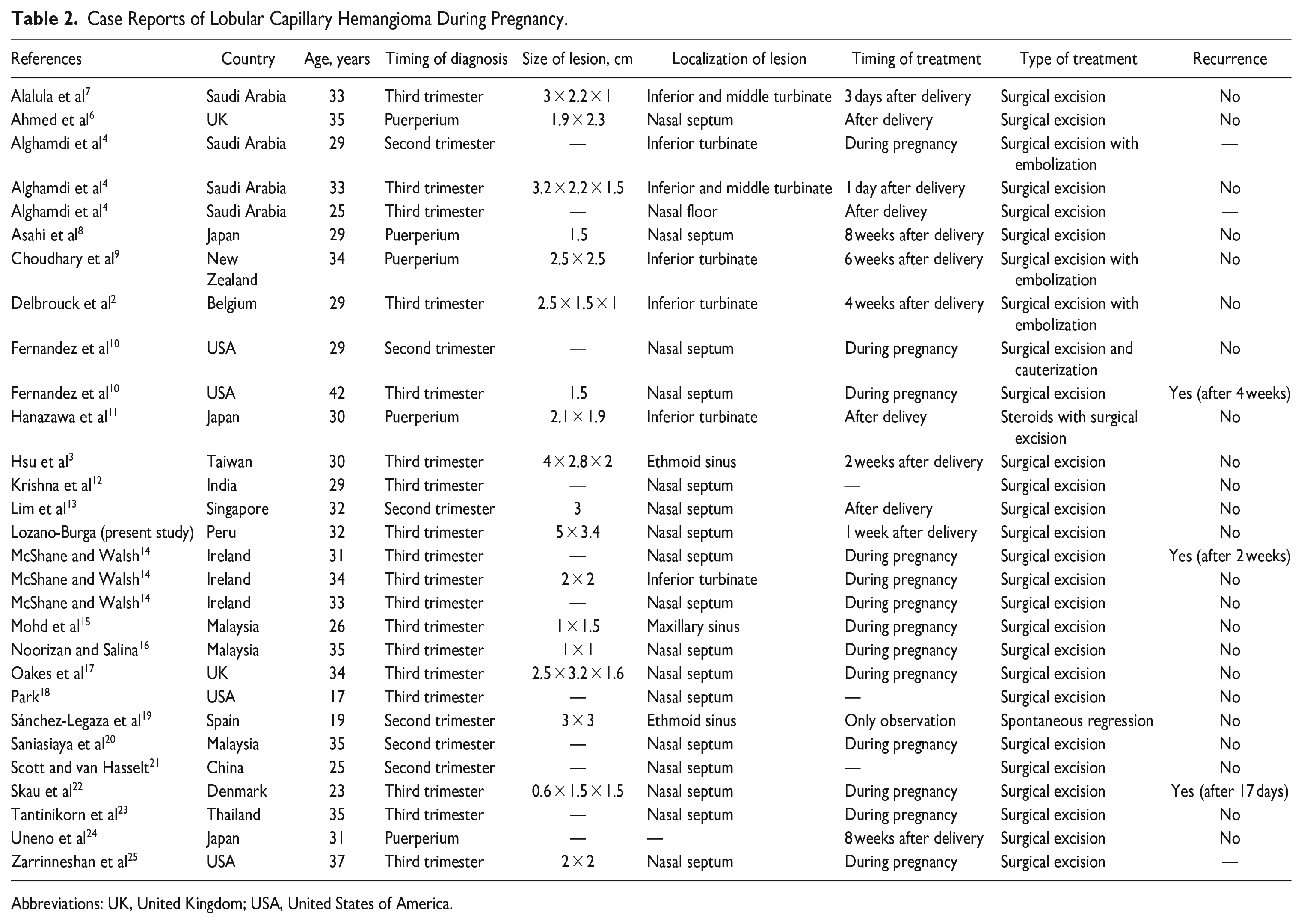
Abbreviations: UK, United Kingdom; USA, United States of America.
Imaging
Data on imaging were reported only in 41% of reports. Overall, nasal LCH on MRI demonstrates isointensity and hyperintensity in T1- and T2-weighted images, respectively. 6 On computed tomography, as a unilateral mass of soft tissue density that usually fills the nasal cavity. 2 Cases of bony erosion were not reported.
Treatment and Outcomes
Nearly half of the patients (48%) were treated after delivery and 45% of cases during pregnancy. Surgical excision was performed in 80% of patients. Recurrence occurred in only 11% of cases and occurred 2 to 4 weeks after surgery. All cases with recurrence occurred only in those treated during pregnancy and none after delivery. Overall, only one patient had spontaneous regression of nasal LCH. 19
Discussion
To our knowledge, this is the first study that summarizes published cases of nasal LCH during pregnancy. Most cases were diagnosed in the third trimester of pregnancy. The most frequent location of LCH was the nasal septum. Nearly half of the cases were treated by surgical excision after delivery and recurrence was relatively low.
LCH is a common lesion of the skin and mucous membranes, which is seen in women in the second decade of life. 26 LCH shows an unusual predilection for pregnant women and its incidence during pregnancy ranges from 2% to 5%. 26 Although it can develop at any time during pregnancy, our study found that it occurs mainly during the last 2 trimesters. The pathogenesis of LCH involves hormonal imbalance and an excessive inflammatory response following local trauma to the skin and mucosa. 27 Since no specific etiologic agent has been identified, the lesion is currently considered an inflammatory overgrowth. 27
Most LCH lesions are small and usually are located in the oral cavity. 26 Nasal LCH is rare, originating mainly in the soft tissues of the nasal cavity. 7 Our review showed that 62% of nasal LCH arise from the nasal septum (Kiesselbach’s plexus). Other sites included inferior or middle turbinate, maxillary sinus, ethmoid sinus, and nasal floor. The first clinical manifestation of nasal LCH is typically recurrent epistaxis. 6 Accordingly, we found that all published cases presented with epistaxis. Its rapid growth may result in nasal obstruction through the affected nostril with subsequent dilatation of the nares and protrusion of the nasal ala. Rhinoscopy often shows a wine-red mass, often covered by a grayish fibrinous membrane, usually attached to the septum by a narrow pedicle. 17 Although pain is not a characteristic of LCH, it may ulcerate or be covered by necrotic tissue.
Histopathologically, LCH is a lesion covered by a superficial layer of keratinized stratified squamous epithelium, often showing irregular ulceration. 23 It is characterized by a submucosal vascular proliferation arranged in lobules or clusters composed of central capillaries and branching tributaries. Extreme endothelial proliferation and the formation of numerous vascular spaces are the most common histologic features. The lesion has a characteristic lobular arrangement of capillaries within a network of fibrovascular tissue at its base. 2 These appearances are nonspecific and identical to those of a pyogenic granuloma. However, histiocytes may be a special feature of granuloma gravidarum and are usually not seen in pyogenic granulomas.4,18 There are few studies on the correlation between LCH pathogenesis and sex hormones or growth factors demonstrated by immunohistochemical analysis. The results have found a negative expression of estrogen and progesterone receptors, while they do show a positive expression of vascular endothelial growth factor. 28
In some cases, immunohistochemical analysis can help in the differentiation of LCH from other similar entities such as angiofibroma and hemangiopericytoma. 29 LCH is a benign vascular proliferation characterized by dilated and lobular capillaries, with typical immunohistochemical expression of endothelial markers such as CD31, CD34, and factor VIII, but with negative expression for beta-catenin protein and androgen receptor.29,30 In contrast, angiofibroma presents a more complex architecture with a combination of vascular and fibrous components, with positive expression for CD31 and CD34 on endothelial cells, as well as positive expression for beta-catenin and androgen receptor on stromal cells. 31 Hemangiopericytoma is characterized by spindle cells and positive expression for the CD34 marker, but negative for CD31. 32
Although the nasal LCH may spontaneously resolve in pregnant women within 1 to 2 months after delivery, surgical excision may be required if the lesion persists or bleeds excessively. 25 Only one case of spontaneous regression has been reported in the literature. 19 Endoscopic surgical excision is the treatment of choice for nasal LCH.4,10,20 Excision during pregnancy, when the mass becomes bothersome, may be an option, especially in cases where bleeding has caused alarm or there are obstructive symptoms. The choice of timing for surgical treatment should be individualized, and the risks and benefits for both mother and baby should always be previously discussed. Interestingly, 3 cases of surgical excision plus preoperative embolization have been described.2,4,9 Most vascular lesions of the nasal mucosa are small and can be safely removed without preoperative embolization or vascular ligation. For larger hypervascular lesions, preoperative embolization is an option that has been used to reduce lesion size, decrease the likelihood of significant blood loss, improve operative visualization, and reduce operative time. 33 In addition, it has been recommended that a small fragment of mucosa and perichondrium around the implantation pedicle should be resected to avoid recurrence. 4
Conclusions
Our review shows that nasal LCH during pregnancy is a benign condition that usually manifests in the third trimester. The most common clinical presentation is epistaxis. Nasal LCH can be treated surgically with a relatively low risk of recurrence.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241230218 – Supplemental material for Nasal Lobular Capillary Hemangioma During Pregnancy: A Systematic Review
Supplemental material, sj-docx-1-ear-10.1177_01455613241230218 for Nasal Lobular Capillary Hemangioma During Pregnancy: A Systematic Review by Yenny Lozano-Burga and Carlos Diaz-Arocutipa in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
None.
Author Contributions
Yenny Lozano-Burga and Carlos Diaz-Arocutipa were involved in study conception and design, data collection and analysis, and manuscript writing and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.