
Abstract
Schneiderian papilloma is typically found on the lateral nasal wall, but, in rare cases, can be located at the mucosa of the nasal septum. Respiratory epithelial adenomatoid hamartoma (REAH) is rare, non-neoplastic lesion characterized by an abnormal proliferation of glandular part of the respiratory nasal mucosa. We present a case of a 42-year-old man with five-year history of bilateral nasal obstruction, rhinorrhea, epistaxis, and hyposmia. On endoscopic examination, we found lobulated, yellowish-pink soft tissue masses on both sides of the nasal septum. The results of histopathological analyses showed the characteristics of Schneiderian papilloma in the lesion excised from the right and REAH in the lesion excised from the left side of the nasal cavity. To our knowledge, cases of simultaneous presentation of Schneiderian papilloma and REAH on opposite sides of the nasal septum have not been published so far. An appropriate cooperation of rhinologist and pathologist allows for a correct diagnosis of these rare and unusual lesions.
Introduction
Inverted papilloma (IP), also known as Schneiderian papilloma, is a benign neoplasm that is associated with three key biological characteristics: tendency to recur, capacity for local destruction, as well as a tendency towards malignant transformation in 3–10% of cases, according to data from the literature.1-3 It is typically found on the lateral nasal wall, but, in very rare cases, can be located at the mucosa of the medial parts of the nasal cavity.1-3 Olfactory part of the nasal septum is an exceptionally rare site of the IP origin and only a few cases with that location have been previously reported.1-3 Respiratory epithelial adenomatoid hamartoma (REAH) is a rare, non-neoplastic lesion characterized by an abnormal proliferation of glandular part of the respiratory nasal mucosa. 4 Contrary to IP, with which there are certain macroscopic similarities, REAH is commonly located in the olfactory area and can have a bilateral presentation, often associated with nasal polyposis.4-6 We present a unique case of a male patient with IP originating from the right-sided superior part of the nasal septum associated with the REAH of the left olfactory area of the same nasal septum.
Case presentation
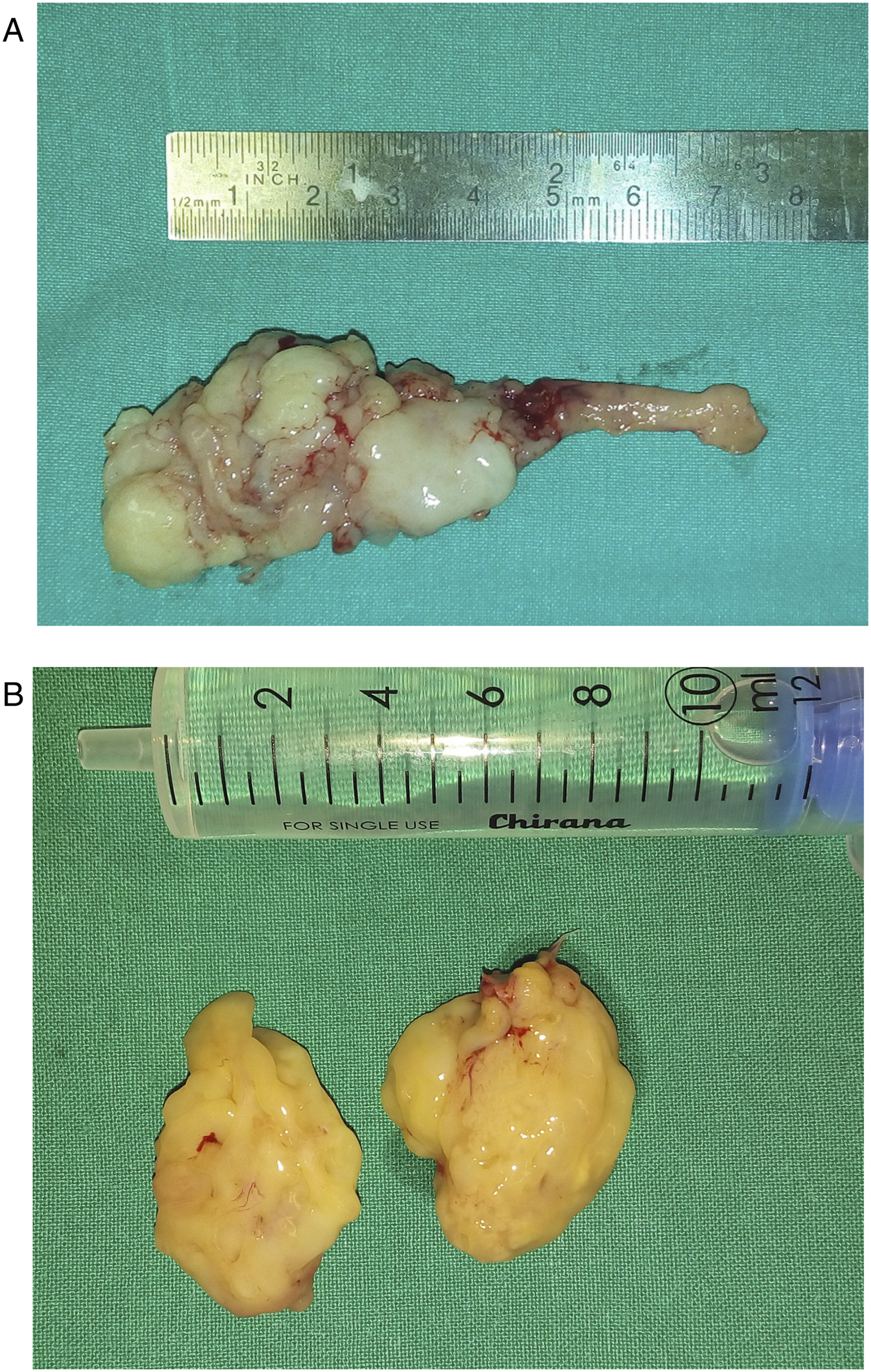
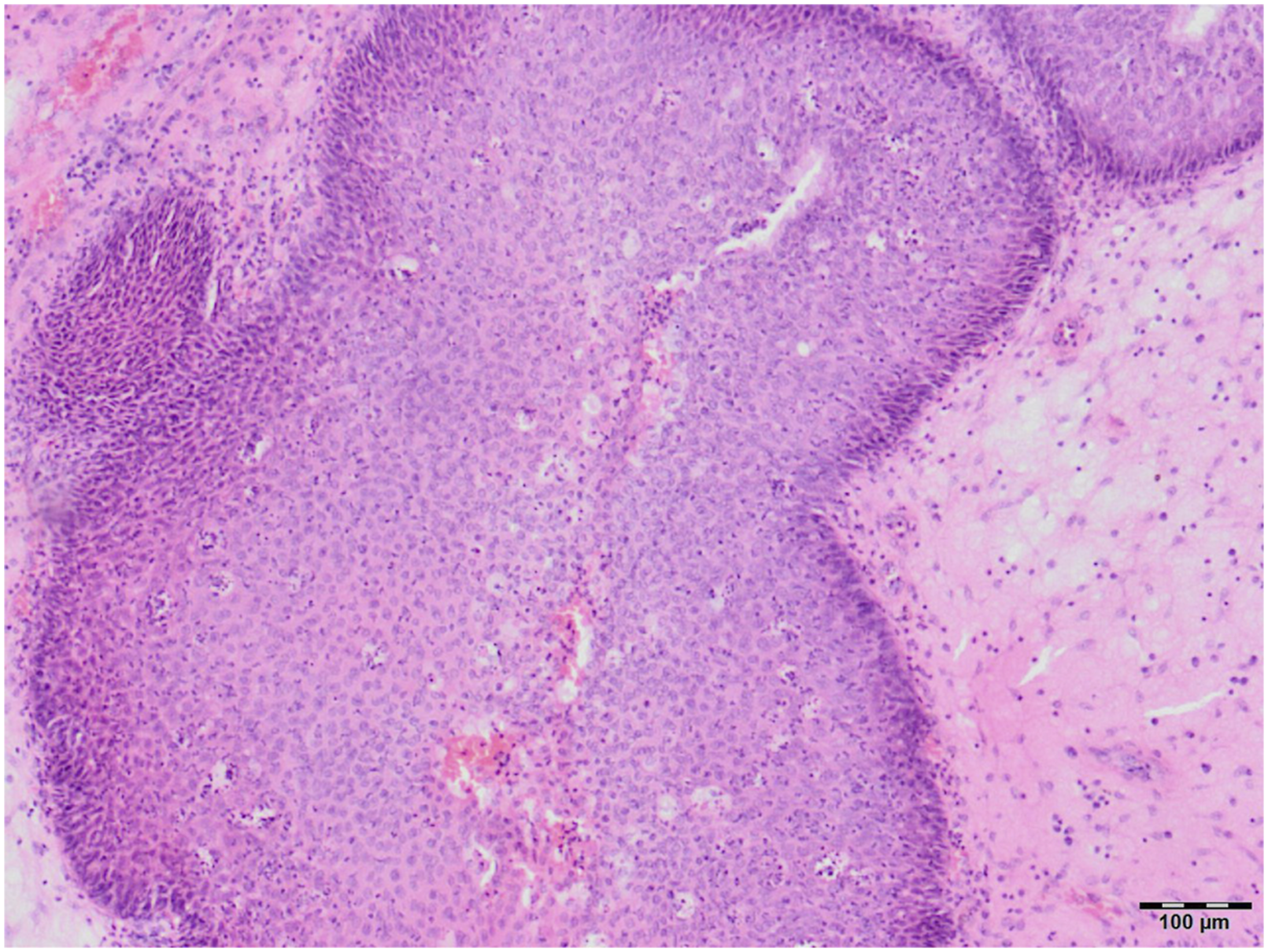
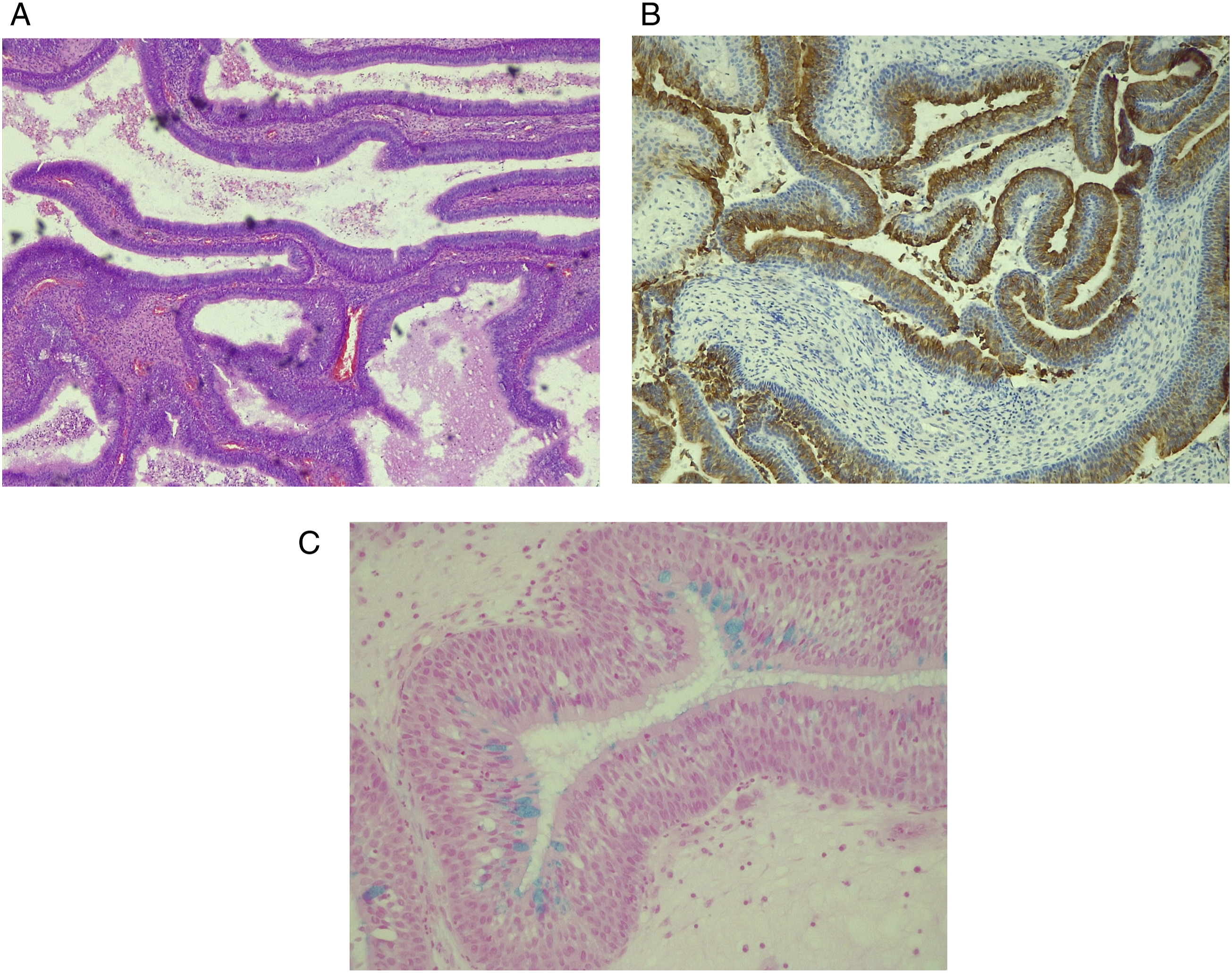
A 42-year-old man was examined in our outpatient office for slowly progressive bilateral nasal obstruction, mucous discharge from the nose with postnasal drip, impaired sense of smell, and scanty epistaxis. Symptoms generally progressed equally slowly on both sides of the nasal cavity. Apart from the perennial allergic rhinitis that he has had since childhood, the patient was in relatively good health. An allergy test showed hypersensitivity to dust mites (Dermatophagoides pteronyssinus) and mold (Alternatia alternata). On endoscopic examination, we found smooth, lobulated, yellowish-pink lesions attached to the corresponding parts of the olfactory mucosa on both sides of the nasal septum. A computed tomography (CT) scan of the paranasal sinuses showed the presence of soft tissue masses filling both sides of the nasal cavity, as well as fluid collection in the left ethmoid labyrinth and left maxillary sinus (Figure 1). Therapy consisted of complete endoscopic excision of the masses, left-sided ethmoidectomy and antrostomy. One mass measuring 5 x 3 x 2 cm was removed from the right side of the nasal cavity (Figure 2A), and two masses measuring about 2 x 2 x 1 cm each were removed from the left (Figure 2B). Macroscopically, the lesions had a similar papillomatous appearance, but the masses removed from the left side were lighter in color, with a more yellowish tint (Figure 2A, and B). The histopathological report indicated bilateral IP. As the finding of bilateral IP of the olfactory region was very unusual and as we expected confirmation of other diagnosis, the surgeon requested a revision of the histopathological analysis by another pathologist. After the repeated analysis, the diagnosis of IP was confirmed for the lesion removed from the right side of the nasal septum. Infoldings and stromal invaginations of the transitional cell (Schneiderian) epithelium, with absence of glandular proliferation were highly indicative of the diagnosis of IP (Figure 3). However, the finding for the lesions removed from the left side of the septum was different. The pathologist described a submucosal proliferation of small-to-medium-sized, round-to-oval glands, lined with several layers of ciliated respiratory epithelium, often admixed with mucin-secreting cells (Figure 4A). Immunohistochemical analysis demonstrated that stromal epithelial (glandular) components of lesion were predominantly strongly positive for cytokeratin-7 (CK-7) (Figure 4B). Ki-67 staining was positive only in the basal layer of the epithelium, indicating normal proliferative activity. Finally, alcian blue-periodic acid-Schiff (AB-PAS) staining was most intense in the mucinous glands, and the majority of metaplastic cells were goblet cells (Figure 4C). Thus, from our initial assumption, the diagnosis of REAH was confirmed only for the lesion removed from the left side of the septum. The patient regularly came for follow-up examinations, and one year after the surgery, he is free of nasal symptoms and with normal findings in the nasal cavity. A CT scan of the paranasal sinuses showing the presence of soft tissue masses filling both sides of the nasal cavity, as well as fluid collection in the left ethmoidal labyrinth and left maxillary sinus. (A) Macroscopic appearance of lesion removed from the right side of the nasal cavity. (B) Macroscopic appearance of lesions removed from the left side of the nasal cavity. Photomicrograph of histopathological finding of lesion removed from the right side of the nasal septum. See the infoldings and stromal invaginations of the transitional cell (Schneiderian) epithelium, with absence of glandular proliferation. This finding is highly indicative of the diagnosis of inverted papilloma (Hematoxylin & eosin staining, magnification x 100). Photomicrograph of histopathological finding of lesion removed from the left side of the nasal septum. (A) Submucosal proliferation of small-to-medium-sized, round-to-oval glands, lined with several layers of ciliated respiratory epithelium, often admixed with mucin-secreting cells (Hematoxylin & eosin staining, magnification x 50). (B) Stromal epithelial (glandular) components of lesion are predominantly strongly positive for cytokeratin-7 (CK7) (magnification x 100). (C) Alcian blue-periodic acid-Schiff (AB-PAS) staining is most intense in the mucinous glands, and the majority of metaplastic cells are goblet cells (magnification x 200).
Discussion
Since the primary histopathology report of bilateral IP was highly unusual, an order to repeat the analysis was warranted in our case. According to the way of growth and biological characteristics, papillomas can be divided into exophytic, inverted (Schneiderian), and oncocytic. The exact etiology of IP is not known, although either chronic inflammation and human papilloma virus infection have been considered.1-3 It is usually a unilateral benign tumor of the lateral nasal wall, although cases of atypical presentations have been described in the literature. Frontal and sphenoid sinus locations have been reported, but the medial part of the nasal cavity and the bilateral presence of Schneiderian papilloma are exceptionally rare occurrences.1-3 Although the nasal septum and nasal vestibule are mainly known as the growth sites of exophytic type of papilloma, cases of inverted growth in lesions originating from the mucous membrane of the nasal septum have also been described.1-3 Given that bilateral presentation of IP is possible, it is necessary to carefully examine the contralateral nasal cavity before and during surgery as well as during the follow-up. 1 In any case, the bilateral presentation of IP should raise the suspicion on the existence of a malignant transformation in the IP tissue, and such a situation requires additional clinical and pathohistological diagnostics.
REAH is a benign sinonasal lesion of unknown etiology. It is a proliferation of various differentiated epithelial cells with no atypia with an edematous stroma infiltrated with inflammatory cells.6,7 Metaplasia involves only the goblet cells of the respiratory epithelium and it is reflected in the enlargement of these glandular cells and their overflowing with mucin. 7 Exactly such changes were observed in our patient in the lesion removed from the left side of the nasal septum. While most authors still consider it a developmental anomaly rather than a true neoplasm, the role of chronic inflammation is increasingly considered as a factor that initiates and stimulates the growth of REAH.4,5 Long-term allergic rhinitis in our patient could have been a factor that stimulated the growth of REAH. Similar to patients with allergic rhinitis and aspirin-exacerbated respiratory disease (AERD), REAH is often located in the central compartment of the nasal cavity, the part of the nasal mucosa most exposed to aeroallergens.4,5 Schertzer et al. 4 found that patients with REAH have a high incidence of allergy along with chronic inflammatory conditions. Due to the similarities in location and pathophysiology between allergic rhinitis, AERD and REAH, conditions located in the medial parts of the nasal cavity, marked as “central compartment atopic disease,” the authors hypothesize that these entities are the result of the action of the same etiological factors. 4 Indeed, the proliferation of the respiratory epithelium and the enlargement and enhanced function of goblet cells probably occur as a tissue response to inflammation caused by long-term exposure to allergens, as is the case with our patient.
Conclusion
To our knowledge, this is the first report of simultaneous presentation of Schneiderian papilloma and REAH in opposite sides of the nasal septum. An appropriate cooperation of rhinologist and pathologist allows for a correct diagnosis of these rare and unusual lesions. We suggest the need for repeated histopathological and, if necessary, immunohistochemical analysis in all cases with primarily diagnosed bilateral and medially located IP.
Footnotes
Author’s Note
The patient’s permission was obtained.
Acknowledgments
This investigation was conducted as a part of scientific project of the Military Medical Academy Faculty of Medicine, Belgrade, Serbia (MFVMA03/23-25/).
Ethics approval
This investigation was approved by Ethics Committee of the Faculty of Medicine of the Military Medical Academy, Belgrade, Serbia (No 21/2022).
Meeting information
This case report has been accepted for presentation at the 6th Congress of European ORL-HNS, Milan, Italy, October 29 - November 2, 2022.