
Abstract

Among the sinonasal malignancies, adenocarcinoma is the second most common type next to squamous cell carcinoma and it accounts for about 13% of all primary malignancy of sinonasal tract. 1 The 2005 World Health Organization classified sinonasal adenocarcinomas (SNACs) into 2 main categories: salivary and non-salivary SNACs. Salivary SNACs in sinonasal tract show similar pathologic results of SNACs which were founded throughout the entire upper aerodigestive tract. Adenoid cystic carcinomas, acinic cell carcinomas, polymorphous low-grade adenocarcinomas, and mucoepidermoid carcinomas were included in this category. 2,3 The non-salivary SNACs are subdivided into intestinal and non-intestinal type. And, both of intestinal and non-intestinal type also showed low and high grade features according to their histologic charicteristics, respectively. 4
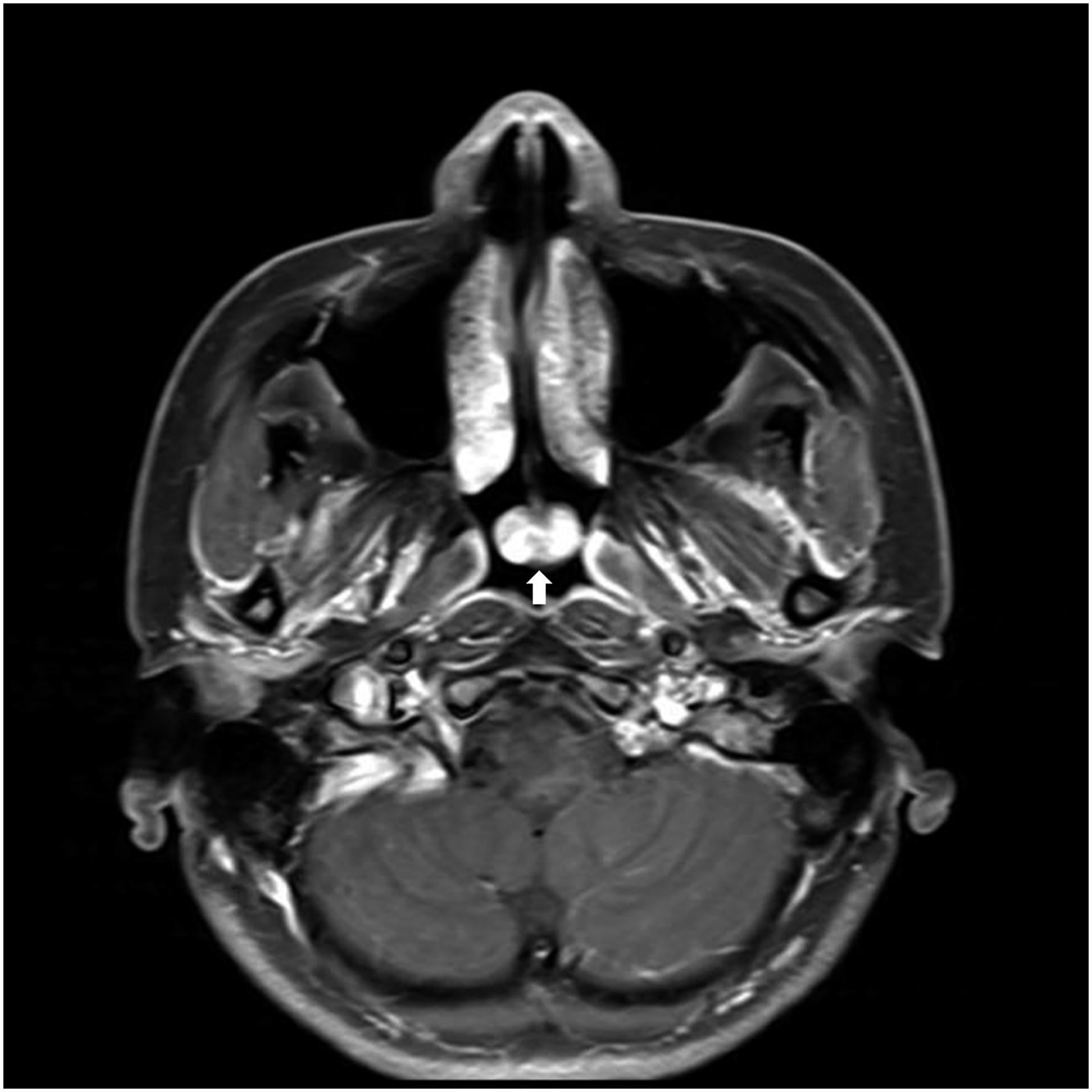
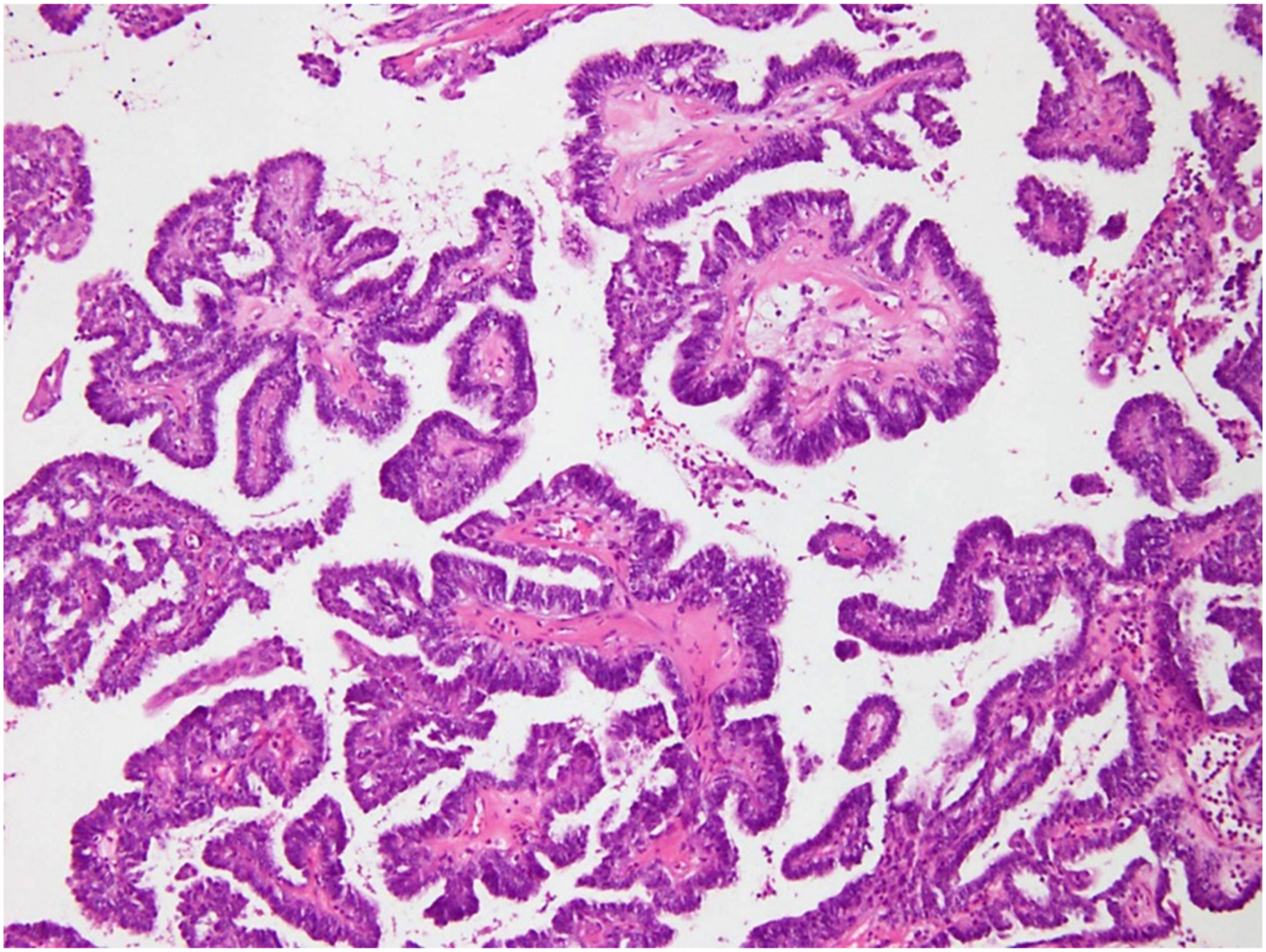
A 29-year-old woman was referred with posterior choanal mass. She presented discomfort at deep inside of the nose when she swallowed for a month. She denied other nasal symptoms such as rhinorrhea, epistaxis, and nasal obstruction. Endoscopic exam shows a round shape polypoid mass at the posterior end of nasal septum (Figure 1). T1 weighted magnetic resonance imaging (MRI) showed a 1.1 × 1.7 × 0.8 cm sized well-defined heterogeneous mass with low signal intensity, and well enhanced with gadolinium (Figure 2). This mass showed high signal intensity in T2 weighted imaging. Endoscopic biopsy was performed and pathologic report showed complex glandular growth with atypical papillary architecture. And, neoplastic glands are lined by a single layer of cuboidal to columnar appearing cells with uniform, round nuclei and eosinophilic cytoplasm (Figure 3). However, mitotic figures and necrosis were not identified. Immunohistochemical staining did not show positivity for CDX-2 and CK20. The pathological evaluation confirmed low-grade non-intestinal type adenocarcinoma. We performed endoscopic complete mass excision via endoscopic approach. Mass was well demarcated and bleeding was minimal. She was discharged at 2 days after surgery without any complications. Round-shaped smooth surface mass was identified at the posterior end of nasal septum. Paranasal sinus MR showed a well-defined ovoid heterogeneous enhancing mass in posterior choana area (white arrow). (T1 weighted image with gadolinium enhance). Neoplastic glands are lined by a single layer of cuboidal to columnar appearing cells with uniform, round nuclei and eosinophilic cytoplasm. (X200, H&E).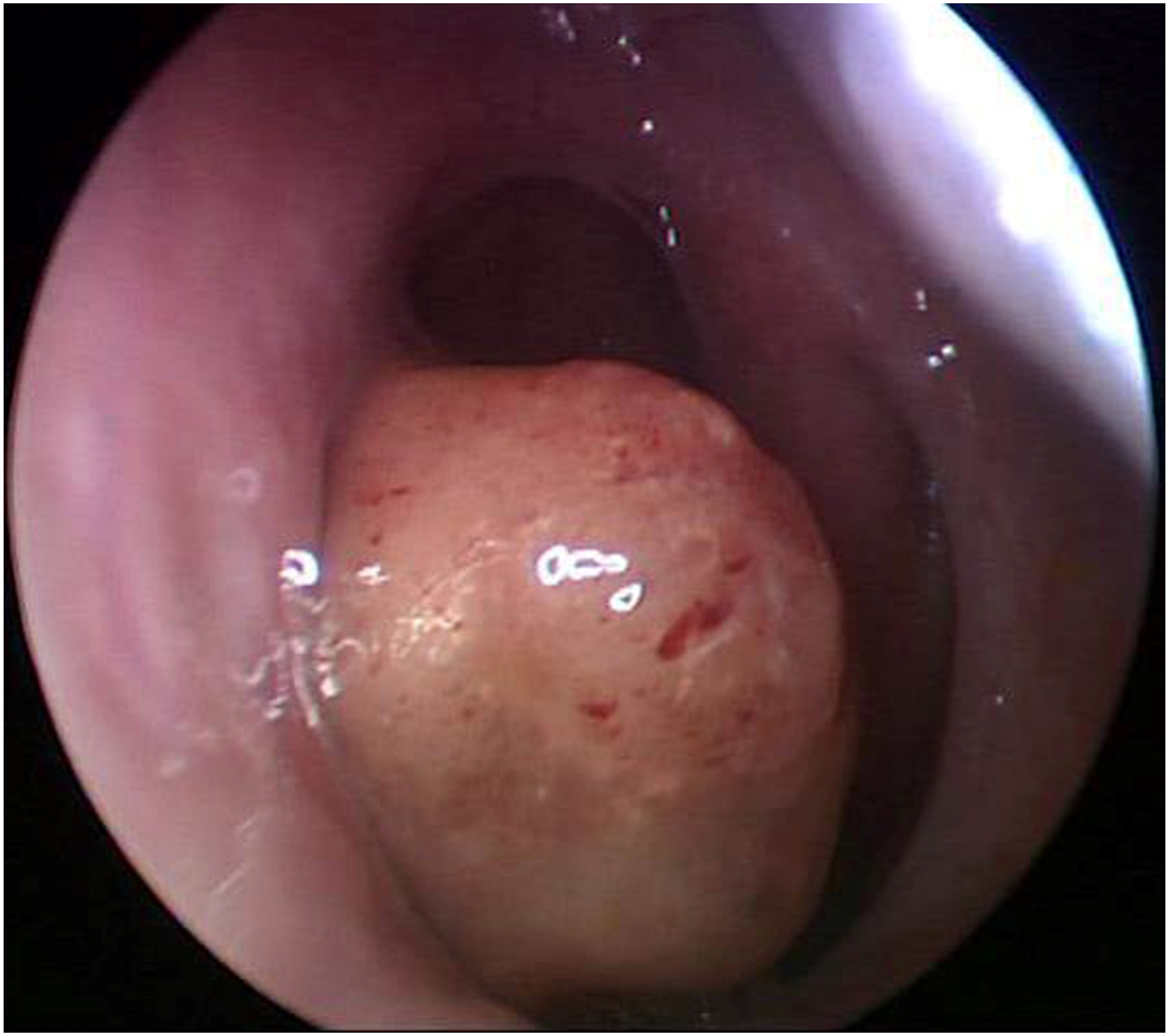
Intestinal type SNACs resemble with colonic adenocarcinomas and can show a mucinous or even signet-ring phenotype. The intestinal SNACs are most common type among sinonasal adenocarcinoma, which account 6% to 13% of primary neoplasms in sinonasal tract. Frequent exposure to wood dust was suggested as risk factor of intestinal type SNACs, even though there was no concrete conclusion. 2,5 Non-intestinal type SNACs are generally diagnosed through exclusion of other possible diagnosis because non-intestinal type SNACs showed marked morphologic heterogeneity such as exophytic papillae, tubular or glandular patterns, trabecular, cribriform, and clear cell and mucinous patterns. 4,6 The papillae and glands are lined by a single layer of columnar or cuboidal cells. The tumor cells show a uniform morphology. Also, low-grade non-intestinal SNACs shows well-differentiated glands with minimal cellular pleomorphism, rare mitotic figures, and no necrosis, when we compared to high grade non-intestinal SNACs showing a marked cellular pleomorphism, necrosis, and numerous mitotic figures. 2,6 However, complex growth pattern and locally invasive growth of these tumors indicate them as malignancy. 4,6 Immunohistochemically, non-intestinal type SNACs are positive for CK7 and S-100 but usually negative for CK20 and CDX2. These findings are helpful to distinguish non-intestinal type adenocarcinoma from intestinal type tumor (positive for CK20 and CDX2). 2
Non-intestinal type adenocarcinoma occurs most frequently in the nasal cavity, followed by the ethmoid and maxillary sinus. 7 There were no known risk factors such as environmental or occupational carcinogens in non-intestinal type SNACs. However, Jo et al reported 4 cases of non-intestinal low-grade SNACs were associated with pre-existing harmatoma. 2
Various type of adenocarcinoma, respiratory epithelial adenomatous hamartoma (REAH), and inverted papilloma should be included for differential diagnosis. Adenoid cystic carcinoma showed nests composed of cytoplasm-rich, round-shaped cells. Tumor cells of ACCs are similar to serous acinar cells with granular or honeycomb cytoplasm of parotid glands. 8 REAH has individual glands of medium to large size extending to the surface, and the basement membrane tends to thicken. In addition, it has a multilayered ciliated respiratory epithelium, which is different from non-intestinal SNACs with a single row of cuboidal to columnar cells. In immunohistochemical staining, p63 and high-molecular weight keratin (HMWK) were positive unlike non-intestinal SNACs. 7 Inverted papilloma could be confused with low-grade non-intestinal SNACs; however, the epithelium of inverted papillomas is 5–30 multilayered thick non-keratinizing cells and does not contain true glandular lumina. Immunohistochemical staining in inverted papilloma showed positive CK7, CK8, CK19, p63, and HMWK. 6,7
Generally, surgical excision is the treatment of choice for non-intestinal SNACs. As long as complete excision of the tumor is the primary objective, endoscopic approach shows lower morbidity. Postoperative radiotherapy has possibility of potential complications due to the close location with some vital structures and less benefit in completely resected case. Adjuvant radiotherapy should be given to patients with affected margin or high grade tumor. 9 However, intestinal type SNACs showed high risk of recurrence and deep local invasion, radiotherapy should be followed after complete surgical resection. 4
Significance Statement
Low-grade non-intestinal type adenocarcinoma that occurs in the nasal septum is rare. Differential diagnostics with tumors such as various types of adenocarcinoma, REAH, and inverted papilloma are essential. Low-grade non-intestinal type adenocarcinoma does not require additional radiation therapy but should be followed for recurrence after complete surgical reservation.
Footnotes
Authors’ Note
We confirm that the manuscript has been read and approved by all named authors and all authors contributed. There are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board of Jeju National University Hospital approved this study.