
Abstract
Nasal extranodal NK/T-cell lymphoma (NNKTL) is a lethal disease due to poor prognosis with rapid progress. A 56-year-old man complained of left nasal obstruction and blood-stained nasal drip for two months. Incisional biopsies were performed at the outpatient department three times, and the diagnosis of SCC was made. The patient underwent wide excision of the entire lesion via endoscopic sinus surgery with navigation. Final pathologic report revealed NNKTL. Pathological examination of the tumor revealed overlying epithelium presenting as pseudoepitheliomatous hyperplasia (PEH), which mimicked SCC invasion, with infiltration of atypical lymphocytes in the deeper sections. Immunohistochemistry supported the diagnosis of NNKTL. Chemoradiotherapy was administered, and a complete response was achieved at the two-year follow-up. The correct diagnosis of NNKTL is essential for prompt treatment and prevention of superfluous surgery. Although the link between PEH and NNKTL may lead to a misdiagnosis of SCC, multiple large and deep biopsies can prevent this dilemma. A biopsy showing ulceration or necrosis can indicate PEH and imply potential malignancy. Repeated biopsies and complete immunohistochemical studies are important for diagnosing NNKTL.
Keywords
Introduction
Nasal extranodal natural killer (NK)/T-cell lymphoma (NNKTL) is a lethal and rapidly progressive disease with a poor prognosis. The prevalence of NNKTL in Asia is 10-fold higher than in Western countries and is strongly associated with Epstein-Barr virus infection. 1 However, the disease, which was first described in the 20th century, is still rare. The most common symptoms of NNKTL are nasal obstruction and bloody rhinorrhea. NNKTL usually presents as an ulcerative mass lesion in the nasal cavity. Invasion of the facial bones and orbits causes craniofacial destruction in the advanced stage. The disease is often diagnosed at an advanced stage because of its nonspecific symptoms and rarity. Thus, treatment is often delayed.
Immunological and biochemical techniques are used to confirm NNKTL diagnoses. The histopathological features can be misinterpreted as squamous cell carcinoma (SCC) due to the pseudoepitheliomatous hyperplasia (PEH). PEH is considered a diagnostic pitfall of NNKTL. However, the link between PEH and NNKTL has not been thoroughly explored. Herein, we report a necrotic nasal tumor that was initially misdiagnosed as SCC. The correct diagnosis of NNKTL was made after surgical intervention. Approval was obtained from the Institutional Review Board of the Mackay Memorial Hospital of this study (22MMHIS204e).
Case Report
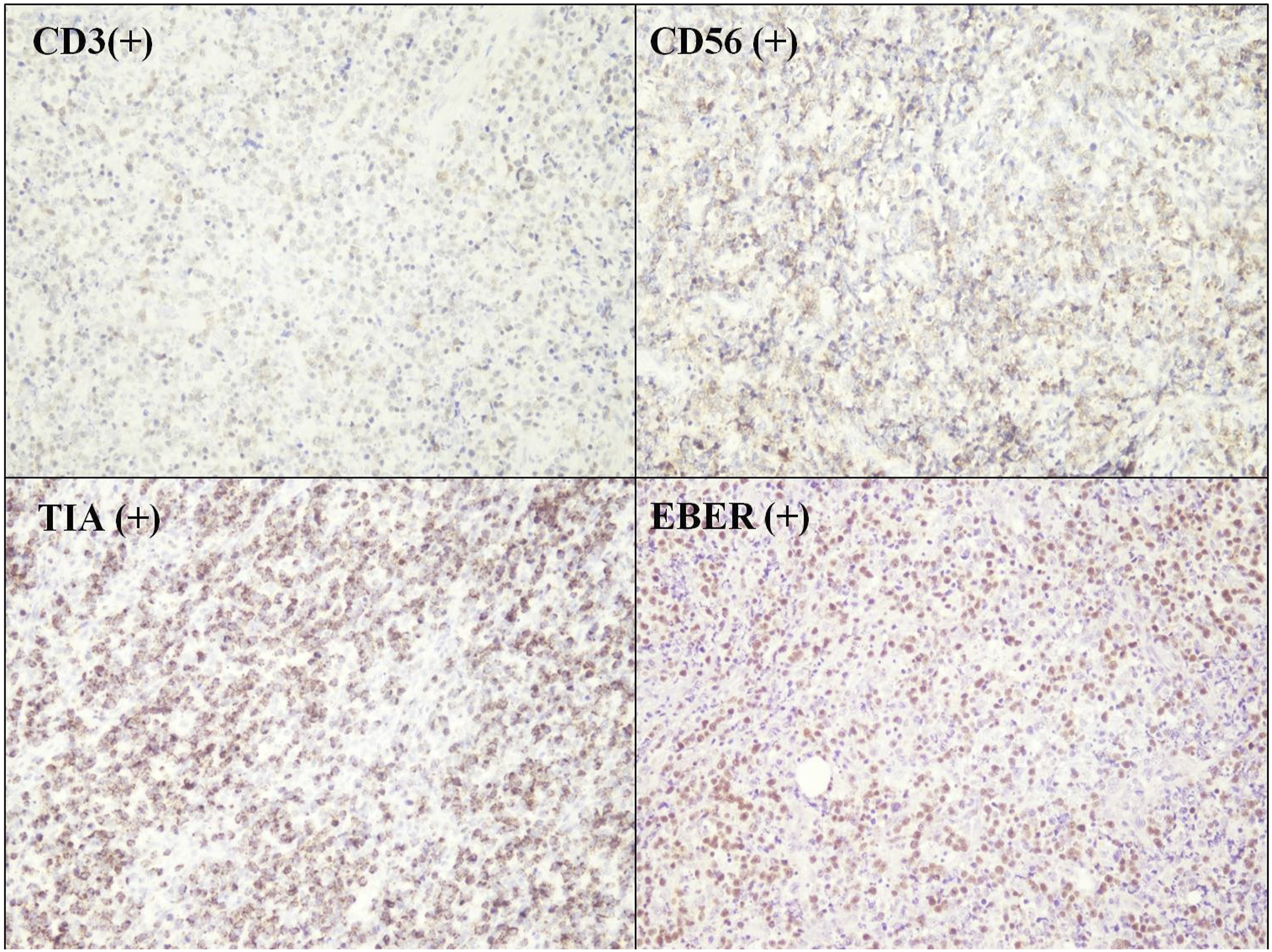
A 56-year-old man complained of left nasal obstruction and blood-stained nasal drip for two months. He had received septomeatoplasty five years previously for deviated nasal septum and chronic hypertrophic rhinitis. Apart from diabetes mellitus, the patient had no systemic diseases. Rigid sinoscopic examination showed an ulcerated mass lesion involving the left nasal septum and inferior turbinate (Figure 1(A)). At the outpatient clinic, biopsies were performed three times over one and half months as the tumor gradually grew. The first biopsy revealed necrotic tissue. The second biopsy showed squamous epithelial hyperplasia without an increased Ki-67 index. In the third time biopsy, irregular epithelial hyperplasia was strongly and diffusely cytokeratin 17-positive upon immunostaining. Thus, a diagnosis of SCC was made. Cancer staging workup showed a tumor involving the nasal septum and left nasal cavity without metastasis. The patient underwent endoscopic tumor excision with navigation. Pathological examination of the tumor revealed overlying epithelium presenting as PEH, which mimicked SCC invasion, with infiltration of atypical lymphocytes in the deeper sections (Figure 1(B)). Immunohistochemistry revealed atypical lymphocytes, which were diffusely positive for CD3, CD56, T-cell intracytoplasmic antigen (TIA), and Epstein-Barr virus-encoded small RNA (EBER) (Figure 2) but negative for CD20. These results supported the diagnosis of NNKTL. Chemoradiotherapy was administered, and a complete response was achieved at the two-year follow-up. (A) Ulcerated mass over the left nasal septum and inferior turbinate. (B) Tongue-like downward epidermal projections mimicking the invasion of squamous cell carcinoma with infiltration of atypical lymphocytes. Immunohistochemical staining showed positive CD3, CD56, TIA, and EBER staining (TIA, T-cell intracytoplasmic antigen; EBER, Epstein-Barr virus-encoded small RNA).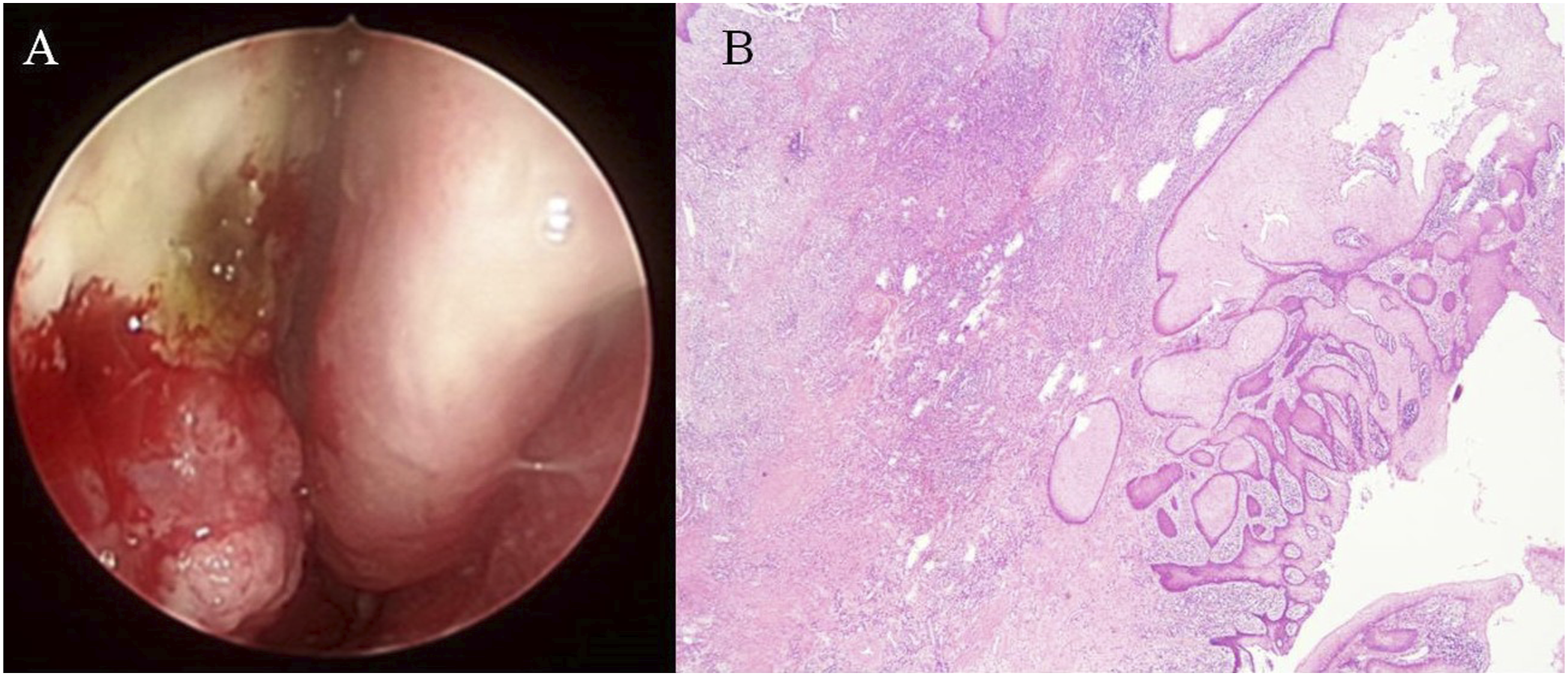
Discussion
NNKTL is a rare form of NK/T-cell lymphoma, constituting 1–2% of all NK/T-cell lymphoma. 2 The common site of presentation is the upper respiratory tract, particularly in the nasal region. Various extranodal sites may be presented such as the gastrointestinal tract, skin, testes, liver, and spleen. Initial symptoms are nasal obstruction and epistaxis. Systemic symptoms include fever, night sweats, and body weight loss. After the necrotic lesions extend to the skin, orbits, oral cavity, and oropharynx, it can cause facial deformity. Study showed symptoms of NNKTL including nasal obstruction in 70–80% of patients, bloody rhinorrhea in 44–47% of patients, and B symptoms in 31–53% of patients. 3 Bone marrow infiltration occurs in lower than 10% of the patient. 4 These nonspecific symptoms are often suggestive of infection or inflammation and leading to management delayed. In the literature review, cases mimicking dacryocystitis, necrotizing sinusitis, or periorbital cellulitis with unresponsively antibiotics and surgical treatment are sporadically documented.5,6 In Sao Paulo, Brazil, 7 patients diagnosed with NNKTL from January 2005 to June 2013 and found that the time from symptom onset to histopathological diagnosis ranged between 2 months and 1 year, and the average time period between onset of symptoms and diagnosis was 5.3 months. 7 Sands et al. found that the mean time to diagnosis was 21.5 months in a study of NNKTL. 8
Microscopically, NNKTL is a disease of atypical lymphoid proliferation with exhibiting angiocentric and angiodestructive patterns. 9 Necrosis and fibrosis are observed over nasal mucosa. Inflammatory cells including small lymphocytes, plasma cells, macrophages, and eosinophils infiltrate the lesions. The tumor cells express NK cell marker (CD56), T-cell marker (cytoplasmic CD3), and cytotoxic granules (granzyme-B, TIA-1, perforin). 10 They are usually detected by in situ hybridization for EBER, indicating that EBV plays a part in lymphomagenesis. In some studies, the level of plasma EBV DNA affects disease-free survival significantly. 11
Clinically, PEH is hard to distinguish from SCC, especially in superficial and small biopsies. PEH is a benign reactive feature related to chronic inflammation or neoplasm and is characterized by tongue-like downward epidermal projections elongating into the stroma. These projections have jagged borders and sharply pointed bases. The keratinocytes may show minor atypia and subtle mitosis. 12 Multiple sections, including the base of the lesion and the underlying lamina propria, and precise immunohistochemical biomarkers are required for a definitive diagnosis. Of note, the first diagnosis is not always correct. When a diagnosis of SCC is contemplated, the possibility of PEH with underlying neoplasia should be considered.
Presentation of PEH over NNKTL is uncommon. Ling et al. investigated 888 cases of NNKTL and found that the incidence of PEH was 3.8% (34 cases). 13 Because NNKTL is rare, the connection between PEH and NNKTL can be misinterpreted as SCC, leading to treatment delay, unnecessary radical surgery, and poor prognosis, with 5-year overall survival ranging from 10% to 45%. 14 We analyzed 41 patients with NNKTL from May 2002 to August 2022 in MacKay Memorial Hospital, a medical center. This is the only one case (2.4%, 1/41) mimicking as SCC because of PEH. In our case, the PEH overlaid the NNKTL, and atypical lymphocytes infiltrated deeply and focally into the stroma, imitating SCC invasion. Immunohistochemical staining, including positive staining for CD3, CD56, and TIA and negative staining for CD20 and cytokeratin, confirmed the NNKTL diagnosis. In addition, the in situ hybridization for Epstein-Barr virus was positive. 15
In conclusion, a correct diagnosis of NNKTL is essential for prompt treatment and prevention of superfluous surgery. Although the link between PEH and NNKTL may lead to a misdiagnosis of SCC, multiple large and deep biopsies can prevent this dilemma. A biopsy showing ulceration or necrosis can indicate PEH and imply potential malignancy. Repeated biopsies are important for diagnosing NNKTL. Furthermore, histological examination and complete immunohistochemical studies can confirm the diagnosis of NNKTL.
Footnotes
Acknowledgments
The material used in this study was provided by MacKay Memorial Hospital, Taipei, Taiwan. The authors would like to thank MacKay Memorial Hospital, Taipei, Taiwan, for their assistance
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approval was obtained from the Institutional Review Board of the Mackay Memorial Hospital, Taipei, Taiwan, of this study (22MMHIS204e).