
Abstract
Objective
To compare the clinical effects of repairing tympanic membrane perforation (TMP) with the tragus perichondrium–cartilage island and temporalis muscle fascia (TMF) under the otoendoscope.
Methods
The clinical data of 84 patients (total 84 ears) with TMP repaired by otoendoscopy from March 2019 to April 2021 were analyzed. The patients were randomly divided into the control group (n = 42, TMF repair) and the experimental group (n = 42, perichondrium–cartilage island repair). The intraoperative blood loss, operation time, length of hospital stay, success rate of the TMP repair, mean air-conducted sound, and air–bone gap before and after surgery were compared between the two groups.
Results
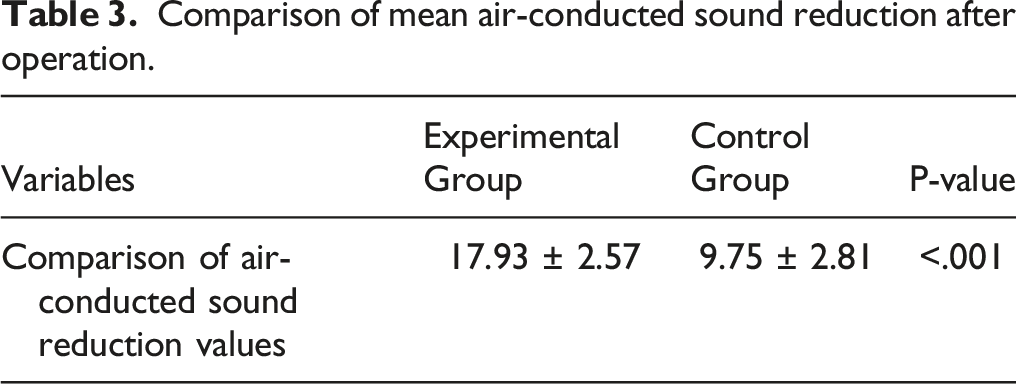
The mean air–bone gap and mean air-conducted hearing threshold in the experimental group were significantly lower after surgery at all frequencies than those of the control group (all P < .05). The reduction of the mean air-conducted hearing threshold in the experimental group was significantly higher than that of the control group (P < .001). The surgery time of the experimental group was significantly shorter than the control group (78.04 ± 2.23 vs. 84.27 ± 1.67 minutes, P < .001). The success rate of the TMP repair was 95.24% (40/42) in the experimental group and 92.86% (39/42) in the control group, indicating that there was no significant difference in the success rate of TMP repair between the two materials (risk ratio = 1.75; 95% confidence interval: .31-12.04; P = .71).
Conclusion
Repairs with the tragus perichondrium–cartilage island have a short operation time, high healing rate, and more significant postoperative hearing improvement, which makes it a more effective method of TMP repair.
Keywords
Introduction
Tympanic membrane perforations (TMPs) are a common condition, often induced by trauma, tympanitis, and persistent perforations after the insertion of an air pipe. 1 There are various ways to repair TMPs with a high success rate. 2 Small and acute TMPs, such as those caused by mechanical injury, usually heal naturally, which suggests that the tympanic membrane has an innate repair potential. Larger and chronic perforations usually do not heal on their own. 3 Myringoplasty is a surgery that repairs TMPs and consequently improves hearing. Various graft materials have been used to close TMPs, including temporalis muscle fascia (TMF), cartilage, perichondrium, periosteum, dura mater, venous tissue, fat, and skin. TMF is the most common material for repairing TMP; however, using TMF leads to Eustachian tube dysfunction, TMF shrinkage, and adhesive otitis media. As a result, cartilage transplantation has become increasingly implemented. 4
This study analyzes and compares the clinical efficacies of repairing TMPs with tragus perichondrium–cartilage island and TMF under an otoendoscope to provide a basis for future clinical treatment.
Materials and Methods
Participants
Patients meeting the following criteria were included in this study: (I) The TMP did not heal for more than three months, and there was no pus in the past three months; (II) there were no signs of inflammation or infection in the middle ear by otoendoscopy and computed tomography (CT); (III) patients with an intact ossicular bone; (IV) the TMP area was ≥25%; and (V) no history of middle ear surgery.
Patients meeting the following criteria were excluded: (I) patients with ossicular discontinuity; (II) patients with tympanitis combined with other ear diseases; (III) patients with cholesteatoma; (IV) patients with nasal polyps; (V) patients with amygdalitis; (VI) patients with dysfunction of the Eustachian tube; (VII) patients with uncontrolled diabetes and hypertension; (VIII) patients younger than 12 and older than 65; and (IX) patients with sensorineural hearing loss and tympanic sclerosis.
Study Design
The study protocol was registered in Xuzhou Central Hospital and approved by its Ethics Committee (No. XZXY-LJ-20180521-016). All patients were fully informed of the study’s contents and signed informed consent before their surgery.
In the preliminary study, 20 patients were enrolled into two groups of 10. The air conduction (AC) threshold, its mean value, and the corresponding standard error were calculated. The study sample was calculated based on a two-sided 5% type I error and 80% power. The exact number of patients was calculated according to the following formula: Nc=2*S2*(u1+u2)2/(S1-S2)2. u1 and u2 were the corresponding proportion in a normal distribution, and 80 patients were asked for analysis.
A total of 90 patients with TMP treated at Xuzhou Central Hospital from March 2019 to April 2021 were randomly allocated into the experimental (perichondrium–cartilage island) and control groups (TMF), with 45 patients in each group. Six patients were lost to follow-up, so 84 patients were included in the final analysis (42 in each group) (Figure 1). Before surgery, the patients underwent physical examinations and provided detailed medical histories. Flowchart of patients selection.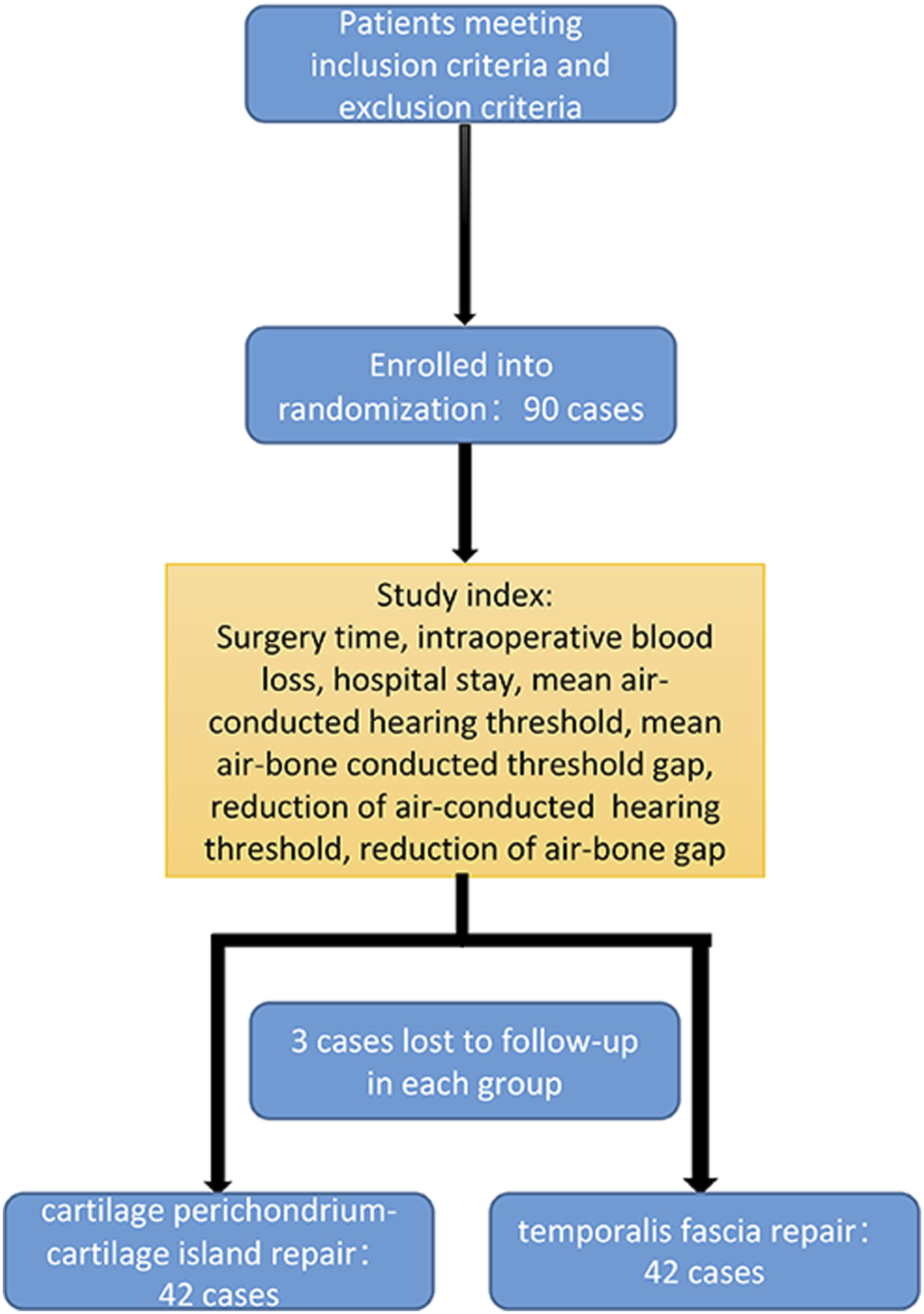
Surgical Methods
The same surgeon performed the surgeries for all the patients.
Cartilage: After a preliminary assessment of the tympanic membrane and its pathology, the tragus was infiltrated with 2% lidocaine and adrenaline (1:200,000). An approximately 3 mm incision was made around the cartilage fornix. The soft tissue and muscle fibers were dissected from the cartilage’s lateral surface to expose the cartilage’s lateral and medial sides completely. After obtaining the composite perichondrium–cartilage graft, the graft site remained open. The perichondrium attached to the anterior side of the tragus cartilage was removed, while the perichondrium on the other side was retained. The cartilage membrane was trimmed by removing the muscle fibers attached to it. Only the island cartilage in the center of the perichondrium was left. The edge of the tympanic membrane was cleaned by micro crochet, and the prepared cartilage was placed between the tympanic membrane and the malleus.
Fascia: An ipsilateral incision across the ear was made directly above the auricle attachment point. The TMF graft was retained, and any residual attachment to muscle and soft tissue fibers was bluntly removed. The grafts were dried and trimmed to the correct size. Then the graft was placed inside the malleus handle and in the residual tympanic membrane in the way of the pad lining.
Observation Indexes
Surgery time, intraoperative blood loss (the weight of the cotton piece with blood minus the weight of the original dry cotton piece plus the volume of drainage), and the length of hospital stay were compared between the two groups. The patients were followed up for one year, and the tympanic membrane healing was compared under an otoendoscope. Pure tone audiometry was performed in the follow-up. The pure tone audiometry of speech frequency (.5, 1, 2, and 4 kHz), the mean air-conducted hearing threshold, the mean air–bone-conducted threshold gap, the reduction of air-conducted hearing threshold, and the reduction of the air–bone gap before and after surgery were compared between the two groups.
Statistical Analysis
All the data collected in this study were analyzed using SPSS 22.0 software. Normally distributed measurement data were expressed as mean ± standard deviation, and Student’s t-test was used to examine the comparisons. The categorical data were expressed as n (%), and the differences between the two groups were examined by chi-square analysis or Fisher’s exact test. P < .05 was considered statistically significant.
Results
Clinical Data
Data of 84 cases of TMP in the experimental group and the control group (%).
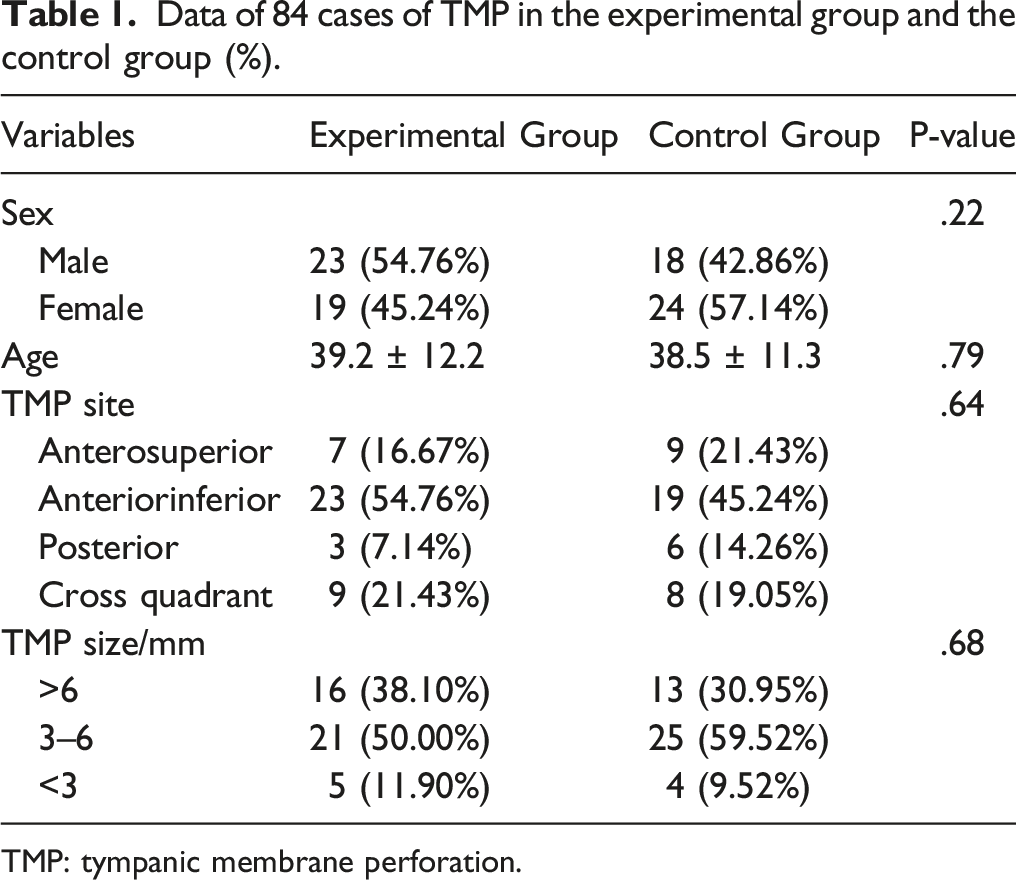
TMP: tympanic membrane perforation.
Comparison of Mean Air-Conducted Sound and the Air–Bone Gap Between the Two Groups Before and After Surgery
Comparison of mean air-conducted sound and air–bone gap between the two groups before and after operation (mean ± SD, dBHL, n = 42).
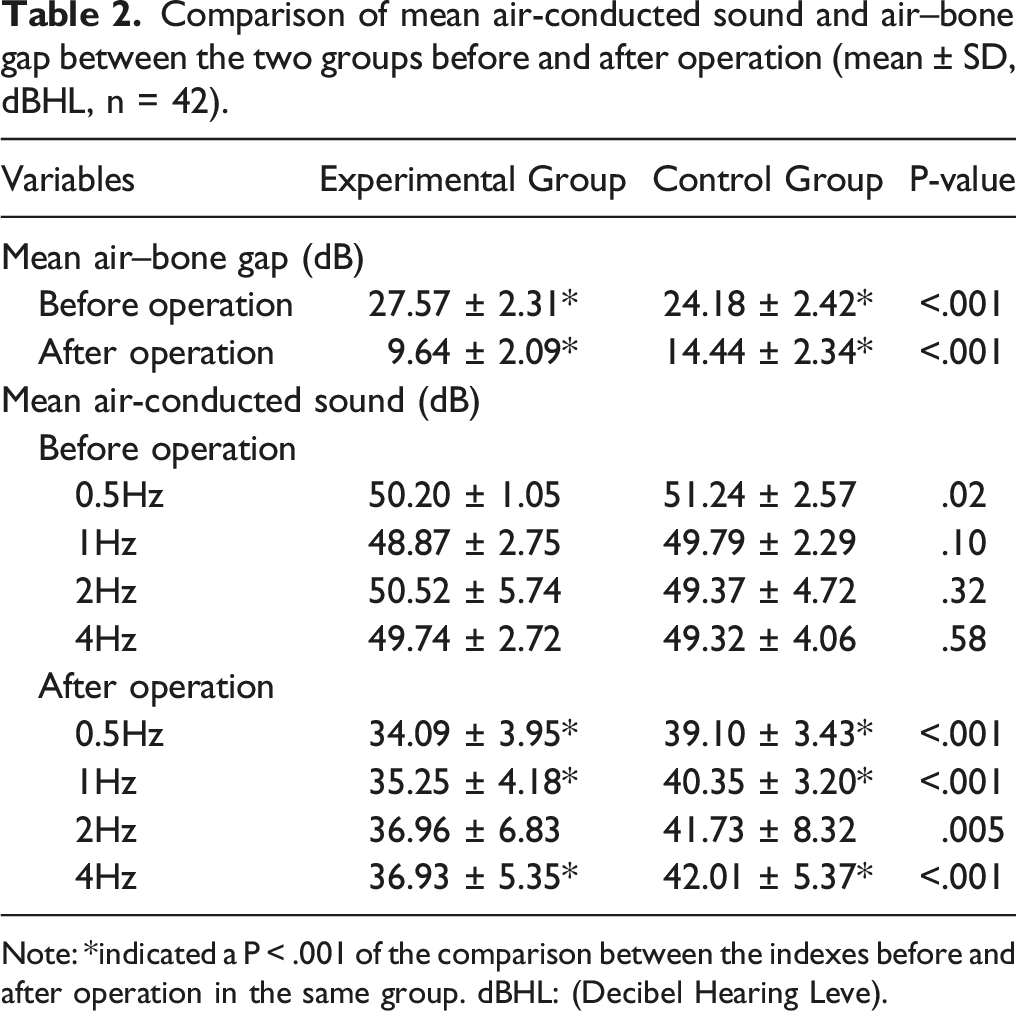
Note: *indicated a P < .001 of the comparison between the indexes before and after operation in the same group. dBHL: (Decibel Hearing Leve).
In the experimental group, the mean air-conducted hearing threshold was 50.20 ± 1.05, 48.87 ± 2.75, 50.52 ± 5.74, and 49.74 ± 2.72 dB HL before surgery at the frequencies of .5, 1, 2, and 4 Hz, respectively. The corresponding thresholds in the control group were 51.24 ± 2.57, 49.79 ± 2.29, 49.37 ± 4.72, and 49.32 ± 4.06 at the frequencies of .5, 1, 2, and 4 Hz, respectively. The threshold of the experimental group was significantly higher at .5 Hz than that of the control one (P = .02). However, there was no difference between these two groups at other frequencies (P > .05).
In the experimental group, the mean air-conducted hearing threshold was 34.09 ± 3.95, 35.25 ± 4.18, 36.96 ± 6.83, and 36.93 ± 5.35 dB HL after surgery at the frequency of .5, 1, 2, and 4 Hz, respectively. The corresponding thresholds in the control group were 39.10 ± 3.43, 40.35 ± 3.20, 41.73 ± 8.32, and 42.01 ± 5.37 at the frequencies of .5, 1, 2, and 4 Hz, respectively. The thresholds of the experimental group were significantly higher at all frequencies than those of the control group (P < .001) (Table 2).
Comparison of mean air-conducted sound reduction after operation.
Bleeding Volume, Operation Time, and Length of Hospital Stay in the Two Groups
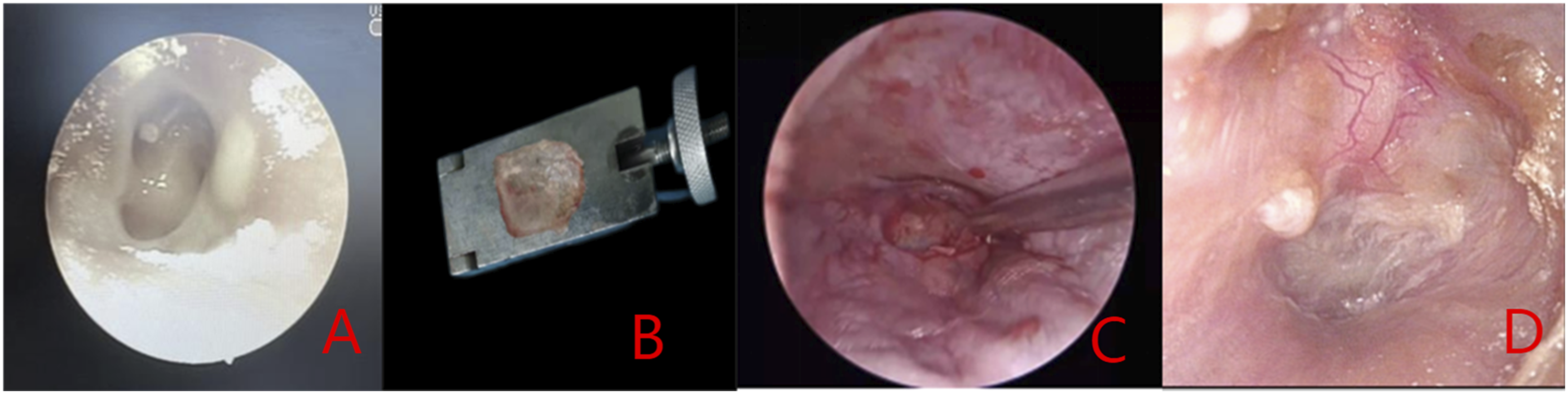
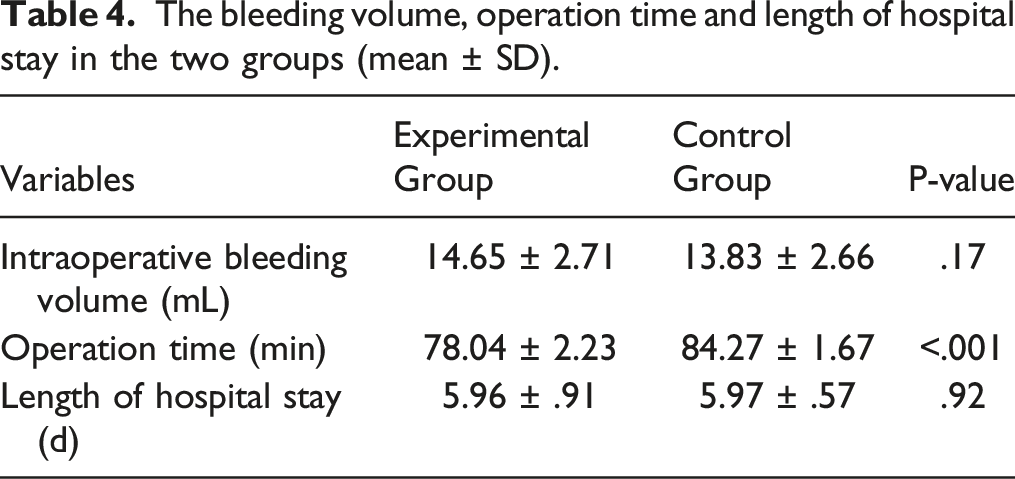
The tympanic membrane healed well in both the experimental and control groups (Figures 2 and 3). The success rate of the TMP repairs was 95.24% (40/42) in the experimental group and 92.86% (39/42) in the control group. The Fisher’s exact test (odds ratio = 1.75; 95% confidence interval: .31-12.04; P = .7126) showed no significant difference in the success rate of the TMP repairs between the two materials. In the experimental group, the average operation time was 78.04 ± 2.23 minutes, the average intraoperative blood loss was 14.65 ± 2.71 ml, and the average length of hospital stay was 5.96 ± .91 days. In the control group, the average operation time was 84.27 ± 1.67 minutes, the average intraoperative blood loss was 13.83 ± 2.66 ml, and the average length of hospital stay was 5.97 ± .57 days. Surgery time in the experimental group was shorter than in the control group, and the difference was statistically significant (t = −14.49, P < .001). The differences in intraoperative blood loss (t = 1.40, P = .17) and hospital stay (t = −.09, P = .92) between the experimental and control groups were not statistically significant (Table 4). Image of tragus perichondrium–cartilage island repairing group. A: preoperative image; B: material preparation; C: intraoperative repair; D: 6 months after operation. Image of temporalis fascia repairing group. A: preoperative image; B: material preparation; C: intraoperative repair; D: 6 months after operation. The bleeding volume, operation time and length of hospital stay in the two groups (mean ± SD).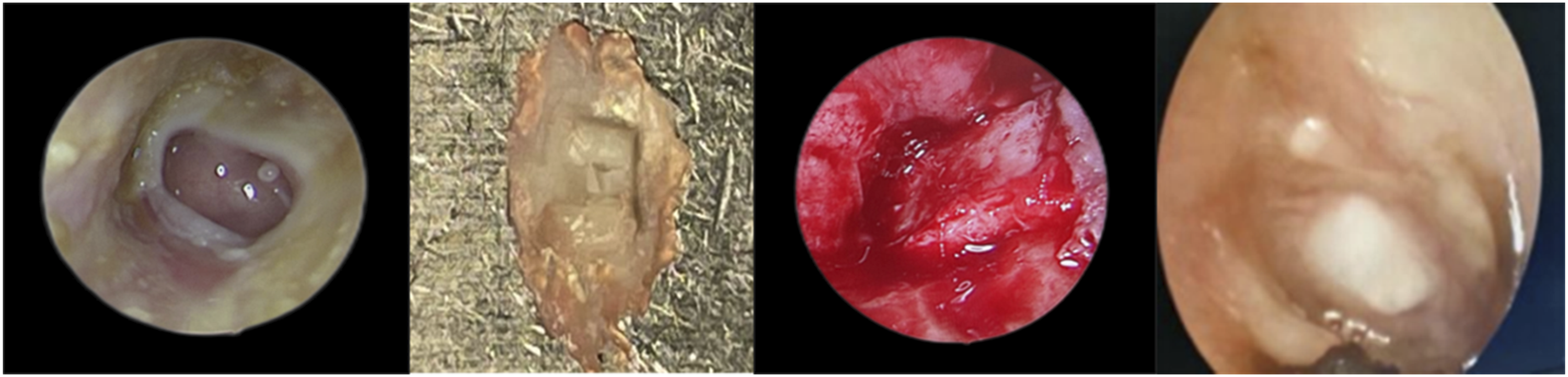
Comparison of Postoperative Repair Effects Between the Two Groups
Repair Effect in the Experimental Group
A large perforation of the pars tensa of the tympanic membrane of the left ear was seen before surgery. The tragus perichondrium–cartilage island was prepared during surgery. The graft was placed between the tympanic membrane and the malleus during surgery, and it could be seen that it healed well six months after surgery (Figure 2).
Repair Effect in the Control Group
A large perforation of the pars tensa of the tympanic membrane of the left ear was seen before surgery. The ear TMF was prepared and dried during surgery, and the graft was placed between the tympanic membrane and the malleus and smoothed during surgery. It could be seen that the graft healed well six months after surgery (Figure 3).
Discussion
Chronic tympanitis is a middle ear infection that can permanently change middle ear secretions and tympanic membranes. 5 The TMP is not just a hole in the tympanic membrane but may lead to hearing loss and significantly reduce the patient’s quality of life. The surgical treatments of chronic tympanitis or the repair of tympanic membrane defects are some of the world’s most common middle ear surgeries. Otoendoscope surgery has become the first choice for audiosurgeries because it is convenient and not highly invasive, and TMF has historically been the most commonly used material. However, an increasing number of cartilage implantations have been performed due to their unique advantages. 6
Endoscopy is increasingly used in otological surgery. It is important to emphasize the main advantages and disadvantages of the endoscope’s features. The main advantage of the endoscope is that it provides a better angle and definition of vision. Endoscopy can also overcome some anatomical obstacles that hinder microscopic observation. Endoscopic technology provides an expanded surgical field with minimal surgical incision and minimizes the damage to soft tissue; thus, surgery efficiency is improved, and pain is reduced. 7 Compared with a microscope, otoendoscopy can obtain a clear field of vision and check whether there is epithelial hyperplasia of the TPM. Compared with a traditional microscope, otoendoscopy does not require a retroauricular incision, which is minimally invasive and has high aesthetic adaptability; the tympanic content can be observed in a linear field of vision without additional bone grinding.8,9 Through the rotating angle mirror, the endoscope can clearly present the complete picture of the surgery field at a mere glance, making the operator able to fully observe the marginal perforation, ear canal, anterior wall, upper and lower tympanic chambers, and other structures on the anterior tympanic membrane. 10 He et al. 11 pointed out that otoendoscopy is becoming more in general. It has a wide field of vision, relatively minimal invasion, a rapid recovery, and causes less pain, all with excellent cosmetic effects. Otoendoscopy is likely to replace middle ear microsurgery without mastoid opening in the future.
A national survey of tympanoplasty in Sweden revealed that it is an operation with a high success rate and low complications; its overall success rate can reach 88.5%. 12 Although otologists have always treated the disease through surgery, the choice of grafts and surgical methods has been controversial. The ideal TMP repair material should have good sound conduction performance, histocompatibility, and sufficient tensile strength. The choice of TMP repair materials is closely related to the success rate of surgery. Autologous materials, such as TMF, tragus perichondrium, cartilage periosteum complex, and other tissues as TMP reconstruction materials, are commonly used by clinical otologists. However, different grafts have different success rates. Temporalis muscle fascia has always been one of the most commonly used graft materials and is considered the gold standard compared with other grafts. Initially, the failure of the TMF graft is mainly related to infections, re-perforations of grafted fascia, and technical errors. The graft will shrink, contract, and change unpredictably after transplantation due to the irregular elasticity and fibrous tissue composition of TMF, which may lead to subsequent abscission and force people to seek a better choice of graft material.
Studies reported that applying the tragus perichondrium–cartilage complex in TMP repair could obtain good clinical results.13,14 The tragus perichondrium–cartilage complex has the highest survival rate among autologous grafts, reaching 92%–100%.3-15 This is the most widely used graft in tympanoplasty. However, autograft materials also have disadvantages. First, the donor site incision needs to be made separately, which deforms the donor site tissue, affecting its appearance. Second, there is a risk of wound infection after taking materials from the donor site. 16
With the development of otoendoscopic technology, otoendoscopic type I tympanoplasty is widely used because of its minimal invasion, cosmetic benefits, and shortened operation time. A study revealed that otoendoscopic surgery and the retroauricular approach could obtain a considerable closure rate. 17 Otoendoscopic surgery is more inclined to use tragus perichondrium–cartilage to repair the tympanic membrane. 18 The commonly used TMP repair material is autologous full-thickness tragus perichondrium–cartilage complex, which has easy access and strong stability. However, it also has a thick and hard texture, which affects the healing ability of a patient’s tympanic membrane.19,20
Cartilage can resist atrophy and absorption, becoming the preferred material. Zhao et al. believed, after reviewing the literature and applying cartilage technology in clinical practice, that after repairing the TMP with soft materials (such as TMF), it will be possible to perforate again once postoperative infection occurs and even necessitate secondary surgical repair. Cartilage is not prone to infection and reperforation after repairing the TMP because of its unique histological characteristics. The secondary perforation will not be too large, even if a postoperative infection does occur. The perforation site will gradually heal once the infection is controlled due to the presence of cartilage scaffolds. Moreover, using a perichondrium patch for repair, the base bed is more durable than the traditional TMF, and the success rate of tympanic membrane regeneration and crawling after surgery is high.21,22 In addition, cartilage grafts come from a wide range of sources and can be collected from the turbinate or tragus, mainly depending on the personal choice of the otologist. Özdemir et al. 23 used otoendoscopy to repair the TMP with tragus cartilage in 104 patients. The results revealed that a high repair success rate could be obtained regardless of the size and location of the perforation. According to the conclusion of the present study, there was no significant difference in the success rate of TMP repair between TMF and perichondrium–cartilage methods. There was a significant effect on postoperative hearing improvement regardless of the method used. However, the hearing improvement was better in the experimental group. There was no significant difference in surgical success rates between these two groups, which might be due to the experienced surgeon who had performed TMF surgery for a long time. However, the shape of the tympanic membrane was different between the two groups. Temporalis muscle fascia repaired membranes were intended to have adhered. In three meta-analyses,4,24 the results of cartilage and TMF reconstruction were similar in improving hearing and reducing the air–bone conduction gap. A study by Guler et al. 25 showed that the acceptance of perichondrium–cartilage was much better, and the increase in hearing ability was also higher than those receiving TMF treatment. Lee et al. 26 showed that the air–bone conduction gap in the group receiving perichondrium–cartilage island treatment was 5dB higher than those receiving TMF treatment. Hou et al. 27 revealed that otoendoscopic TMP repair with a perichondrium–cartilage island has a high healing rate of the tympanic membrane, and postoperative hearing improved more significantly than with TMF treatment, making it a more effective method of tympanic membrane repair. Previous studies showed that TMF repairing results in a better hearing threshold compared with cartilage but with limited improvement. 4 These inconsistent conclusions might be induced by the cases selected, the surgical skills of the surgeons, and the methods of obtaining materials. A large sample study should be used in the future. The present study showed that the postoperative AC hearing threshold of the experimental group was higher than that of the control group. It could be seen that hearing in patients receiving perichondrium–cartilage island treatment was better improved, and the operation time was shortened. The reasons supposed for these results are as follows: 1. During the operation, the perichondrium was routinely retained in the direction of the external auditory canal of the tragus cartilage (concave), the other side of the perichondrium was removed, and the convex cartilage complex was placed in the direction of the tympanic chamber. Its conical structure is more consistent with the physiological depression radian of the tympanic membrane. This structure means it can fit more closely and retain the lateral perichondrium, be conducive to the survival of chondrocytes, and accelerate the healing with the tympanic membrane residue. The cartilage is not susceptible to necrosis, which makes it easier to heal. Compared with previous studies, perichondrium–cartilage island repair was performed rather than with cartilage alone. Only a small piece of cartilage was reserved in the center of the perichondrium and skived as much as possible. The cartilage would be softened and absorbed after surgery, favoring blood vessel formation and preventing poor elasticity from cartilage-induced hearing disorders. 2. The perichondrium–cartilage island has good supporting and healing ability, strong anti-perforation ability, and the graft has a good natural shape. Only a small piece of cartilage tissue is needed. The incision is small, and the damage is small. Moreover, the perichondrium with cartilage is stable and easy to curl. The operation is more convenient and shorter than the TMF group. 3. Compared with perichondrium, cartilage has advantages in mechanical stability. Some scholars used cartilage with different thicknesses (1.0, .7, .5, and .3 mm), cartilage palisade, and perichondrium–cartilage island grafts of different sizes. A laser Doppler was used to examine the frequency response function of cartilage. Comparing different cartilage grafts from an acoustic point of view, .5 mm-thick soft bone island materials showed better vibration characteristics than cartilage plates or palisades. 28 The choice of TMP graft repair material should be based on its mechanical stability and acoustic transmission characteristics. Experiments have shown that cartilage island technology is conducive to improving acoustic characteristics. The .5 mm thick island graft showed a stronger decline in the first resonance frequency and an increase in amplitude. Island grafts exhibited better acoustic properties. 29
There was no difference in the amount of bleeding between the two groups. Although the incision for the TMF was larger, there was no thicker blood vessel, and the surgeon was highly skilled and experienced, so the amount of bleeding was small. The present study displayed that there was no difference in blood loss between these two groups and no difference in the success rate of tympanic membrane repair. However, due to the differences in the biological and physical properties of the materials, the recovery in hearing ability of the experimental group was higher than that of the control group. There was no significant blood loss between the two surgical methods. Patients were generally discharged from the hospital 3-4 days after surgery. Theoretically, the TMF group needed mastoid compression and bandaging due to the postauricular incision. However, there was no statistically significant difference in the length of hospital stay between the experimental group and that of the control group, which might have been due to fears of incision infections or surgical failures in the experimental group, forcing them to stay in the hospital for longer.
The stability and integrity of TMP repairs are important factors in evaluating the success of tympanoplasty. Otologists accept the use of tragus perichondrium–cartilage because it can maintain a good tympanic membrane shape and resist infection and middle ear negative pressure. 30
There were also several limitations in this study. First, it was a single-center analysis, so it should be tested for universality. Second, it was a small sample analysis that should be verified with a larger sample study.
Conclusion
In conclusion, using perichondrium–cartilage island and TMF under the otoendoscope for TMP repairs has good curative effects and improves patients’ hearing. The cartilage perichondrium–cartilage island repairing has a smaller incision, shorter operation time, and better hearing recovery. It is a more effective TMP repair method and is worthy of clinical popularization and application.
Footnotes
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Xuzhou key R&D plan for science and technology projects(KC20135) and Guiding project of medical scientific research of JiangSu Provincial Health Commission (Z2021016).
Ethics Approval
I confirm that I have read the Editorial Policy pages. This study was conducted with approval from the Ethics Committee of Xuzhou Central Hospital (XZXY-LJ-20180521-016). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.