
Abstract
Objectives:
We compared the functional outcomes of fat myringoplasty and areolar tympanoplasty through a small postauricular incision in patients who underwent transcanal endoscopic ear surgery (TEES).
Methods:
The study included patients who underwent myringoplasty or type I tympanoplasty using TEES in our Department of Otolaryngology between April 2016 and May 2019. The patients were divided into 2 groups according to the type of graft material used, which was selected based on the available amount of subcutaneous fat and the surgeon’s experience.
Results:
In total, 63 patients received fat tissue grafts (group A) and 77 received areolar tissue grafts (group B). The median operative time was significantly longer in group B (132 minutes) than in group A (65 minutes); perforations were significantly larger in group B than in group A (61.0% vs 29.7% of the eardrum surface). The postoperative air conduction threshold, air–bone gap, and speech reception threshold values were significantly lower than the preoperative values in both groups. The graft success rate did not significantly differ between groups A (96.8%, 61/63) and B (96.1%, 74/77). In group A, the perforation was > 35% of the eardrum surface in 27.0% (17/63) of the patients; the graft success rate was 100% (17/17). In the remaining 46 patients (perforation > 35%), the graft success rate was 95.7% (44/46); this difference was not statistically significant.
Conclusions:
Transcanal endoscopic ear surgery increases the usefulness of fat myringoplasty for the repair of perforations > 35% of the eardrum surface. Postauricular fatty and areolar tissues are suitable for this simple and rapid technique, which yields excellent outcomes.
Introduction
Modern tympanoplasty techniques were designed in the 1950s with the introduction of operating microscopes. 1 The reported graft take rate in tympanoplasty varies considerably ranging from 60% to 100% in adults.2,3 To improve the take rate, different techniques, and graft materials have been used to close membrane perforations.4,5
Minimally invasive surgeries have gained popularity and endoscopic ear surgeries were introduced in the 1990s. 6 The combination of thin rigid otoendoscopes and full high-definition camera systems has brought about a less-invasive transcanal approach to the middle ear with clear and high contrast views. 7 Transcanal endoscopic ear surgery (TEES) provides a wider view of the surgical field, increased visibility around target objects, and less hidden space.
Tympanoplasty (myringoplasty) is a standard surgical procedure used to repair the tympanic membrane (TM) and improve hearing status. This study compared the functional outcomes of fat myringoplasty and areolar tympanoplasty from a small postauricular incision in patients undergoing TEES.
Materials and Methods
Ethical Considerations
Approval for this retrospective analysis of data from a prospectively maintained database was provided by local clinical governance departments.
Case Selection
This study was conducted between January 2016 and December 2019 at our Department of Otolaryngology Head and Neck Surgery. Patients who underwent myringoplasty or tympanoplasty through TEES were enrolled. Patients were excluded if they underwent mastoidectomy or tympanoplasty other than type 1, if they had ossicular chain defects or cholesteatoma or if they missed the regular follow-up visits. Cases of myringosclerosis with large or marginal perforation were not excluded.
All operations were performed under general anaesthesia by the same surgeon (C.-F. Hwang). The patient data were collected by reviewing the medical records saved in our hospital. The TM perforations were divided according to 4 TM quadrant sizes (Saliba’s subdivision) as shown in Table 1. 4 The patients were divided into 2 groups according to the type of graft used in tympanoplasty, which was selected according to the amount of subcutaneous fat and experience of the surgeon.
Comparison of Subject Data in the Fat and Areolar Tissue Groups.
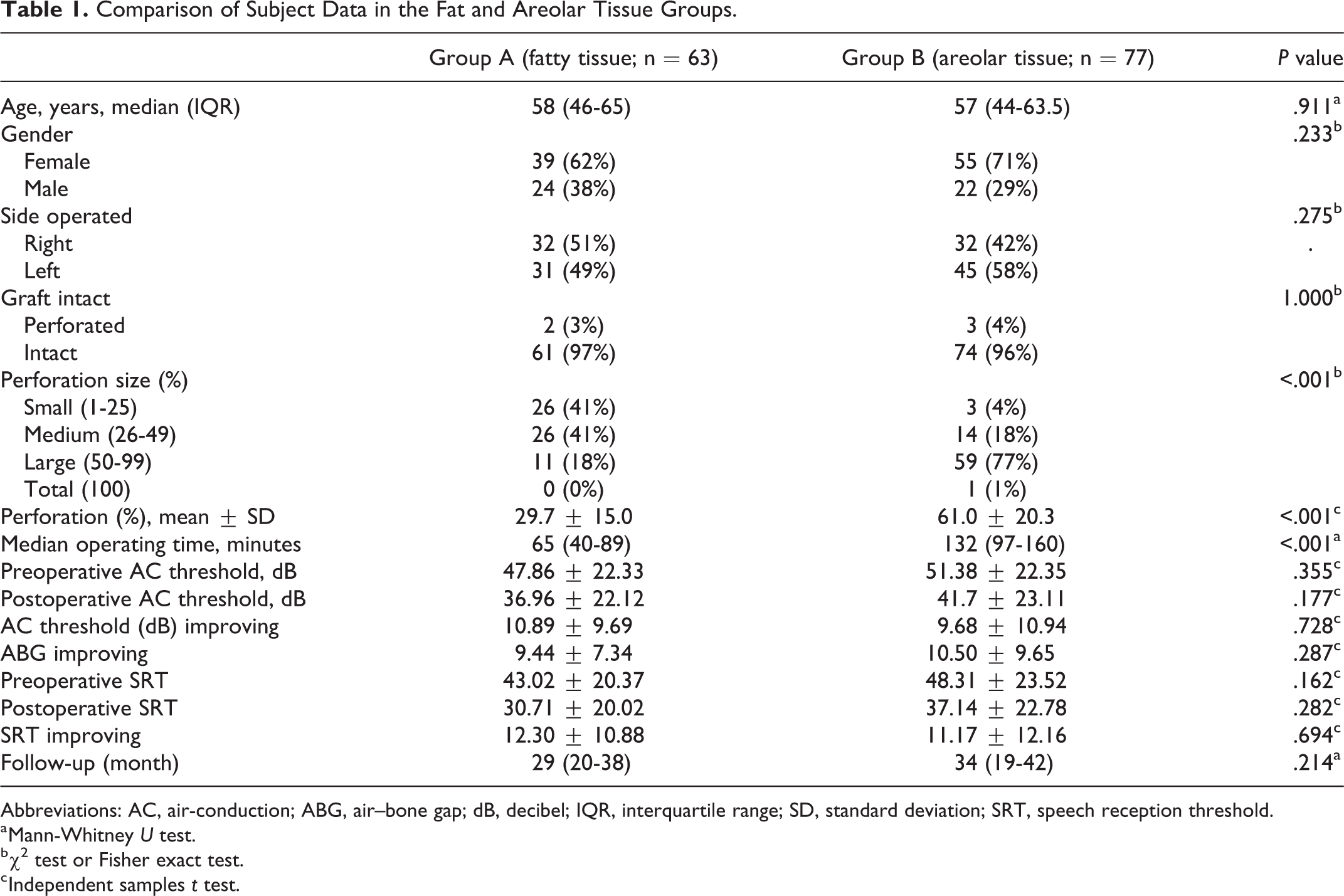
Abbreviations: AC, air-conduction; ABG, air–bone gap; dB, decibel; IQR, interquartile range; SD, standard deviation; SRT, speech reception threshold.
a Mann-Whitney U test.
b χ2 test or Fisher exact test.
c Independent samples t test.
Surgical Techniques
In group A, a 1 cm postauricular incision was made, and subcutaneous fat approximately twice the size of the perforation was harvested by sharp dissection with scissors (Figure 1). Fat myringoplasty was performed with TEES under general anaesthesia. After circumferential de-epithelialization of the margins of the perforation, absorbable gelatin sponges were placed into the middle ear through the perforation to support the fat graft in cases with medium or large perforations, but not in those with small perforations (Figure 2). Then the fat graft was inserted through the perforation as an hourglass-shaped plug. Care was taken to obtain close contact between the fat graft and the TM through TEES.
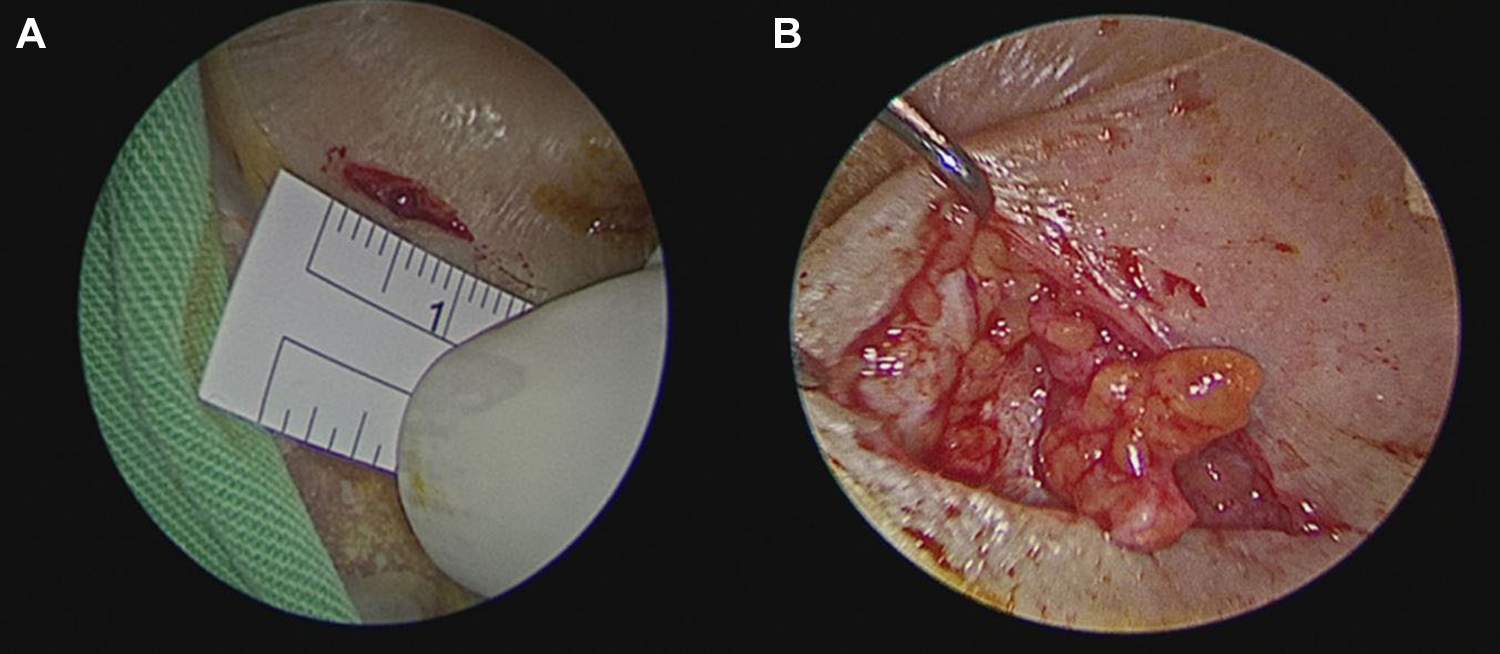
A, A 1 cm postauricular incision was made. B, Subcutaneous fat approximately twice the size of the perforation was harvested by sharp dissection with scissors.
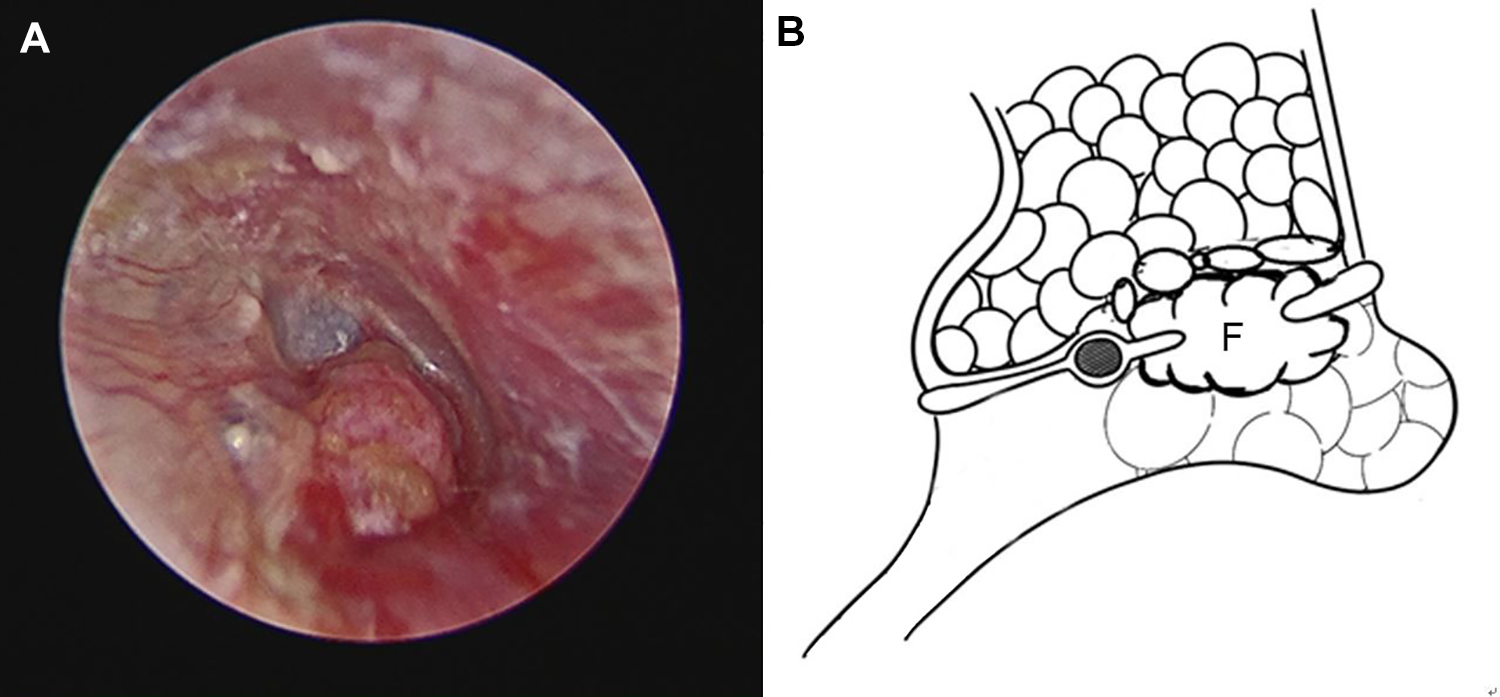
A, The fat graft was inserted through the perforation as an hourglass-shaped plug. B, Absorbable gelatin sponges were placed into the middle ear through the perforation to support the fat graft in cases with medium or large perforations. F indicates fat graft.
In Group B, the grafts were taken from the areolar tissue overlying the temporalis fascia by the same postauricular incision. Areolar tissue grafts were left to dry and reshaped before being placed in the TM. After elevating the tympanomeatal flap, they were placed with an over–under tympanoplasty. 5 The middle ear was packed with absorbable sponges. The dry areolar graft was placed lateral to the long process of the malleus and then medial to the remaining drum anteriorly. Then the ear canal was packed with sponges. All patients were routinely prescribed a course of oral antibiotics during the first postoperative week, with prescription of eardrops until the sponges had been absorbed.
Primary Outcome Measures
Hearing parameters included changes in air–bone gap (ABG) and speech reception threshold (SRT). The pure-tone averages (PTA) for bone conduction (BC) and air conduction (AC) at 0.5, 1, 2 and 4 kHz were calculated. Air–bone gap was calculated by subtracting BC PTA from AC PTA. Data collected included age, sex, side, perforation size, ABG, change in average hearing, and status of TM at 3 months. The postoperative status of the TM in weeks 1, 3, and 12 was recorded along with the results of audiological audiometry tests at week 12. Graft healing was considered successful if the TM was completely intact at the 12-month postoperative visit.
Statistical Analyses
All statistical analyses were performed using SPSS version 19 (IBM). Two-tailed P < .05 was taken to indicate statistical significance. Continuous variables are presented as the mean and standard deviation. Categorical variables are presented as frequency distributions. Continuous variables were compared using Student t test or the nonparametric Mann-Whitney test when normality could not be assumed. The χ2 test was used to compare proportions.
Results
In all, 140 patients were included; there was a male: female ratio of 1:2 and a median age of 57 years. The patients were divided into group A with fat tissue grafts (n = 63) and group B with areolar tissue grafts (n = 77; Table 1). There were no significant differences in the distributions of age, sex, closure rates of perforations, follow-up, and other hearing thresholds between the 2 groups (Table 1). The median operation time was significantly longer in group B (132 minutes) than in group A (65 minutes; P < .001); perforation size was also significantly larger (61.0% vs 29.7%). The postoperative AC threshold, ABG gap value, and SRT showed significant reductions in both groups compared to their respective preoperative values.
The graft success rates were 96.8% (61/63) and 96.1% (74/77) in groups A and B, respectively. With regard to perforation size, there were no significant differences between the 2 groups in terms of graft success rate (Table 2). None of the patients in either group experienced graft lateralization or blunting. The follow-up period ranged from 13 to 51 months, with an average follow-up of 31 months.
Complete Closure Rates According to Perforation Size.
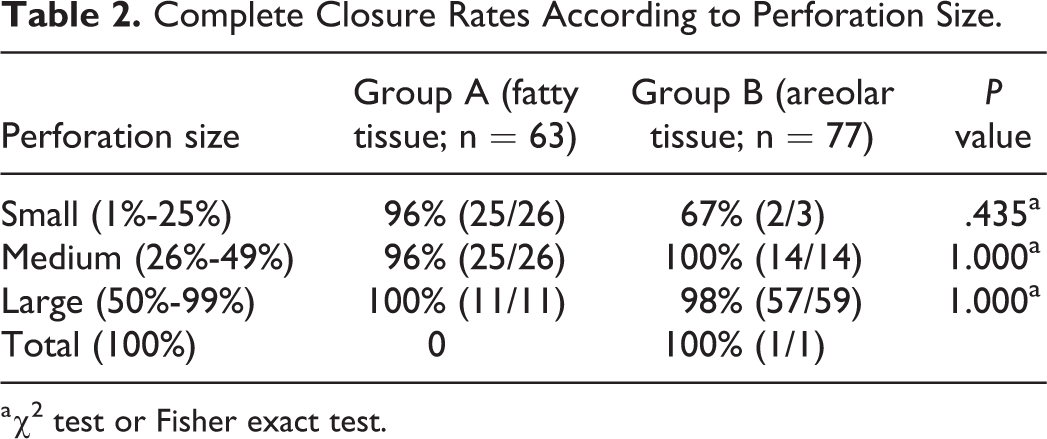
a χ2 test or Fisher exact test.
In group A (fatty tissue), perforation size was > 35% of the ear drum surface in 27.0% (17/63) of cases. The graft success rates were 100% (17/17) in those > 35% and 95.7% (44/46) in those < 35% and the difference was not significant.
Discussion
No studies have compared auditory results and anatomical outcomes between the use of fat and areolar tissue grafts by TEES. Temporal muscle fascia is the most commonly used graft material. However, due to its instability, different types of graft are increasingly used in tympanoplasty. 8 An ideal alternative should be easy to harvest and readily available in the operative field. The postauricular fat and areolar tissue superficial to the temporalis fascia fulfils all of these requirements. Therefore, we harvested subcutaneous fatty or areolar graft tissue from the postauricular region. When sufficient subcutaneous fat tissue is not available to repair the ear drum, the surgeon harvests areolar tissue immediately via the same incision. Using TEES, both grafts showed excellent graft success rates and hearing outcomes.
Ringenberg introduced fat graft myringoplasty in 1962 as a simple, cost-effective, and minimally invasive surgical procedure. 9 The low utilization rate of fat grafts is due to its restricted indications. According to the literature, fat myringoplasty is indicated in cases with a perforation size not greater than 30% to 35% of the eardrum surface, central perforation, and absence of myringosclerosis. 10 The success rate for larger perforations is significantly lower than that for smaller perforations. 11 Cases with larger perforation size had significant lower success rates than those with smaller perforations. In the present study, success rate was similar between TM perforation sizes > 35% and <35%. Transcanal endoscopic ear surgery improved visualization of the tympanic cavity and allowed discovery of hidden disease. In our series, fat myringoplasty was a valid choice for perforations > 35% and even up to 80% using TEES (Supplemental Video).
The ear lobule is the most common donor site for fat grafts. Ear lobule fat is preferable to fat obtained from the abdomen or buttocks because it is denser and exhibits better epithelial and mucosal tympanic growth. 12 However, some patients complained of asymmetry of the bilateral ear lobes and inconvenience with regard to using earrings after the operation. Therefore, we modified our procedure and harvested the fat graft from the postauricular region. A drawback of this procedure is that patients with a lower body mass index may lack sufficient subcutaneous tissue.
Areolar connective tissue is a thin layer of fibers located immediately superficial to the temporalis fascia, which is easily identified before the temporalis fascia is harvested. Goodman first used areolar tissue for tympanoplasty in 1971; it has proven to be an excellent graft material.13,14 In addition to containing abundant collagen and reticular fibers, areolar connective tissue houses fibroblasts, plasma cells, adipocytes, mast cells, and macrophages necessary for successful graft incorporation. 15 Although areolar tissue is less substantial than temporalis fascia, our main concern was preservation of the fascia for later repair, if needed. Given the location of the areolar tissue in the operative field, ample material was available for the repair of extensive perforations.
The operative time was significantly longer in group B (areolar tissue) than in group A (fat tissue) because areolar tympanoplasty required elevation of the tympanomeatal flap via the transcanal approach, whereas fat myringoplasty was performed without elevation of the tympanomeatal flap. Furthermore, the perforations were significantly larger in group B than in group A; thus, it may have taken longer to de-epithelialize the margins of the perforations in group B. Long-term follow-up is necessary after tympanoplasty (myringoplasty) because reperforation may occur gradually. Indeed, success rates tended to be higher in short-term follow-up studies than in longer-term follow-up studies. 16 Given that TEES is a relatively new surgical approach, we have used this technique for fewer than 5 years. Our follow-up period was relatively short, which may explain our higher graft success rate. Both graft success rate and follow-up time did not significantly differ between groups.
This study had some limitations with regard to its retrospective design and the small number of patients. The types of grafts used were not random, and areolar tissue tended to be used in cases with larger perforations. The perforation sizes were significantly different between groups; therefore, the functional outcome findings may have been biased. Further prospective studies with larger sample sizes and long-term follow-up are required.
Conclusions
Application of TEES may reduce the contraindications for fat myringoplasty to repair perforations corresponding to >35% of the ear drum surface. Postauricular fatty and areolar tissues were suitable in this simple and rapid technique, which yielded excellent outcomes.
Footnotes
Authors’ Note
The data that support the findings of this study are available in the supplemental file.
Acknowledgments
The authors thank the staff of the Speech and Audiology Department of Chang Gung Memorial Hospital for their technical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Chang Gung Memorial Hospital (CMRPG8J1121 and CMRPG8G0242). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.