
Abstract
Aim:
The aim of this study is to investigate whether there is a difference in the anatomical success of the graft and the functional gain of hearing as a result of the medial or lateral surface application of the temporalis muscle fascia graft.
Materials and Methods:
Seventy-three patients who underwent tympanoplasty (myringoplasty) type 1 surgery due to tympanic membrane perforation between December 2017 and December 2019 were included in this study. The gender and age of the patients during this study were determined. Preoperative tympanic membrane perforation types were grouped as central, marginal subtotal, and total. Airway pure tone average threshold values were evaluated preoperatively at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz.
Findings:
Seventy-three patients were included in the study. Medial surface of the temporalis muscle fascia was placed onto the manubrium mallei of the malleus with over-underlay method in group 1 (n = 37) and similarly, lateral surface of the temporalis muscle fascia was placed onto the manubrium mallei of the malleus with over-underlay method in group 2 (n = 36). After tympanoplasty, it was seen that 79.5% of the grafts were intact. Graft success was lower in total perforations than other types; 51.7% of the patients with intact graft were group 1, and there was no significant relationship between graft success and groups. As a result of the assessment made in terms of hearing gain, a statistically significant change was detected in the hearing in the postoperative sixth month compared to the preoperative period in both groups.
Conclusion:
In this study, we demonstrated that there is no difference in terms of the anatomical success of the graft and the functional gain of hearing with type 1 tympanoplasty surgery.
Introduction
Tympanoplasty is a surgical procedure used to repair tympanic membrane (TM) perforation, and modern tympanoplasty was firstly described by Zöllner and Wullstein in 1952. 1 Persistent tympanic membrane perforations can occur as a result of chronic otitis media, trauma, or complications of the tympanostomy tube. A number of methods that can be easily performed in a short time without the need for myringoplasty have been described in the treatment of minimal TM perforations, and successful results can be obtained with these methods. 2 -6 Surgical treatment is the treatment of the perforations that are bigger and cannot be achieved with these methods. The aim of surgery is to eliminate middle ear disease and increase hearing by closing perforation in the eardrum.
In tympanoplasty, the aim of the repair of tympanic membrane perforation is to use the most suitable graft material that has high durability and does not adversely affect the hearing results. Nowadays, there is a tendency to use many different materials such as temporalis muscle fascia (TMF), allograft and xenograft conchal or tragal cartilage, and vein graft for graft repair in TM. 7 Temporalis muscle fascia grafts are easily available, inexpensive, compatible with the patient’s own tissue structure, easily formed with flexible structure, and are the most commonly used graft materials that do not have vibration-limiting effects caused by the arrival of sound waves to the tympanic membrane. 8 Temporalis muscle fasciae are protective layers like other fasciae in the body, the sequential structures of endomysium, perimysium, and epimysium, and they do not require arterial nutrition. 9 These fibrous structures are fed by diffusion from both surfaces by adjacent arterial structures such as TMF, pericardium, pleura, and peritoneum. 10 -12
There is not a consensus among the otorhinolaryngologists, especially those who are interested in otology, about whether there is a difference between the medial or lateral administration of TMF or not. At the same time, there is not a similar study in the literature performed with this method. Our aim is to determine whether there is a difference in terms of the anatomical success of the graft and functional gain of hearing as a result of the medial or lateral surface application of the TMF in type 1 tympanoplasty (myringoplasty) surgery.
Materials and Methods
The present study was approved by the clinical ethics committee of Erzincan Binali Yıldırım University (accession number: 33216249-604.01.01-E.16584). All the participants provided signed informed consent before they were subjected to the research procedures.
Seventy-three patients who underwent tympanoplasty (myringoplasty) type 1 surgery due to TM perforation in the Otorhinolaryngology Department of Erzincan Mengücek Gazi Training and Research Hospital between December 2017 and December 2019 were included in this study. The gender and age of the patients during the study were determined. Preoperative tympanic membrane perforation types were grouped as central, marginal subtotal, and total. Airway pure tone average (PTA) threshold values were evaluated preoperatively at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz.
The lateral surface of the TMF (true temporalis fascia is also known as deep temporal fascia) contains skin, subcutaneous tissue, and the medial surface contains temporalis muscle. In this study, we named the surface of the TMF on the side facing the muscle as medial, and the surface on the side facing the skin as lateral (Figure 1). Patients were classified as group 1 and group 2.
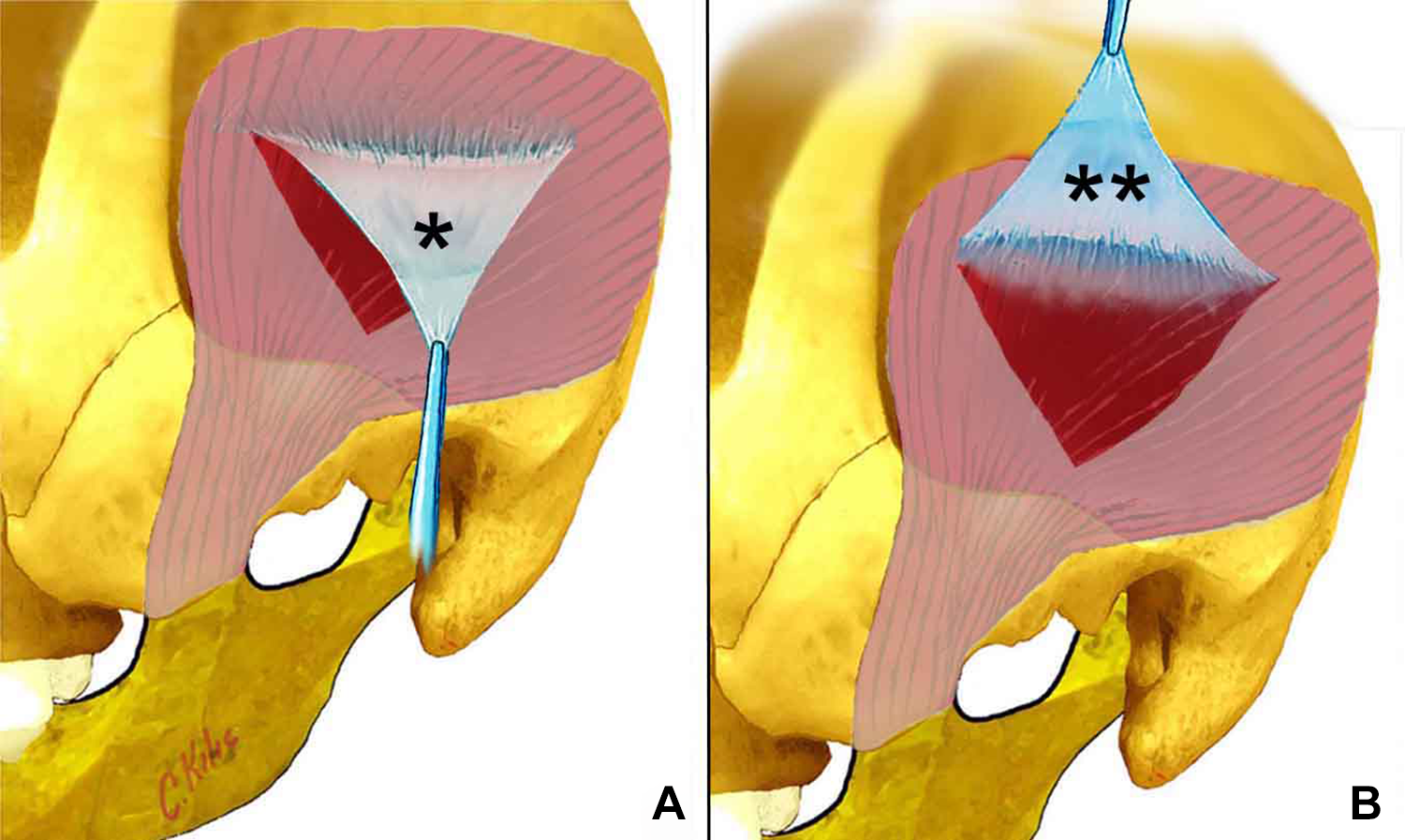
A, Lateral surface of the temporalis muscle fascia. B, Medial surface of the temporalis muscle fascia.
We performed tympanoplasty type 1 with retroauricular or endaural incision approach under general anesthesia in all patients. We uniformly dissected all 2 surfaces of the TMF, we did not leave any tissue on both surfaces of the fascia, and then we proceeded. After administering tympanomeatal flap elevation to group 1, the medial side of the TMF graft was placed onto the manubrium malle of the malleus, and the lateral side was placed under the membrane with over underlay method. Similarly in group 2, the lateral side was placed on the manubrium mallei of the malleus, and the medial side was placed under the membrane residue.
It was investigated whether there was a relationship between postoperative graft administration, graft inactivity, and age, sex, and type of perforation. Compared to the preoperative period, all patients were evaluated for airway pure tone audiometry (PTA) hearing thresholds at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz postoperatively.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) software package version 20.0 (IBM Corp). Descriptive statistics parameters were calculated. Descriptive statistics as number, percentage, mean, and standard deviation were used for data analysis. Statistical analyzes were performed using the Mann-Whitney U test and to the χ2 test examine differences between the groups. Value of P < .05 was defined as statistically significant.
Findings
Seventy-three patients were included in the study and 37 patients in group 1 had medial and 36 patients in group 2 had lateral side as over-underlay. Of all, 50.7% of the patients were female with the ages changing from 15 to 50, and the mean age was 27.3 ± 9.2. The audiometry results of the patients were as follows: the preoperative mean of audiometry was 27.4 ± 9.0 and the postoperative mean was 18.7 ± 10.7.
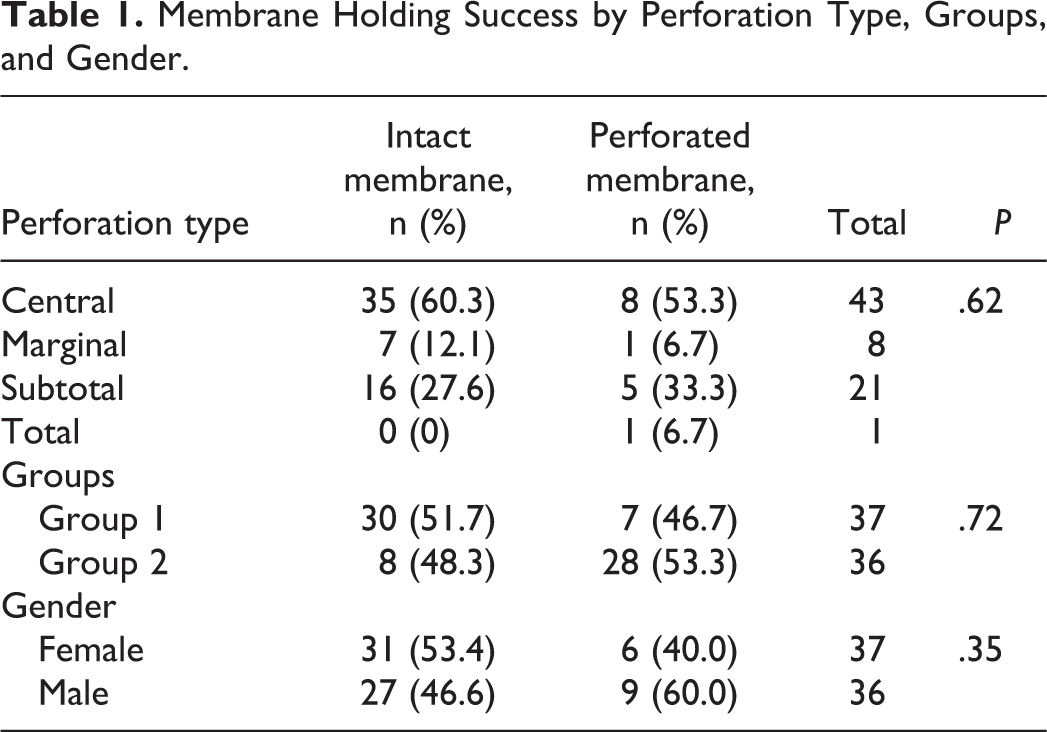
Control examinations performed at 6 months after tympanoplasty revealed that the graft was intact in 58 (79.5%) of 73 patients. When the graft success status was examined, 53.4% of the grafts that held belonged to female patients. There was no significant difference in holding rates by gender (P = .35).
When the graft success rates of the groups separated according to the surgical technique were examined, 51.7% of the grafts were group 1, and no significant relationship was found between the graft success and the groups (P = .72).
When the graft success was evaluated according to perforation types, graft success is the highest in central perforations and the lowest in total perforations. There was no significant relationship between perforation type and membrane inactivity (P = 0.62; Table 1).
Membrane Holding Success by Perforation Type, Groups, and Gender.
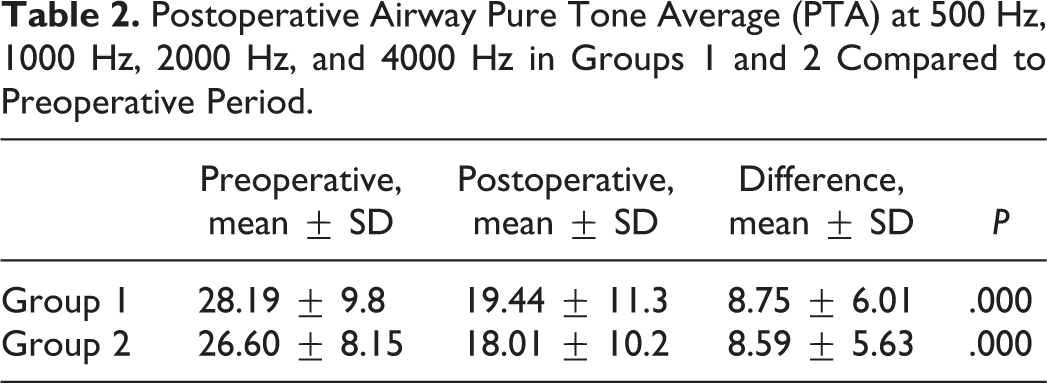
Airway PTA at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz was used as a criterion in evaluating the hearing gains of the patients and the results were evaluated preoperatively and at 6 months postoperatively. As a result of the assessment made in terms of hearing gain, a statistically significant change was detected in the hearing in the postoperative sixth month compared to the preoperative period in both groups (Table 2).
Postoperative Airway Pure Tone Average (PTA) at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz in Groups 1 and 2 Compared to Preoperative Period.
Discussion
The aim of tympanoplasty surgery is to obtain a healthy ear and functional hearing. Since the first tympanoplasty, different graft materials have been used to repair TM perforation. Today, temporalis fascia is the most preferred group among all grafts. 13 The fasciae are about 2 to 3 mm thick and are easily formable and diffusion-fed protective sheets without vascular structures. 9
In our study, the graft success rate of the temporalis fascia was found to be 79.5% in all patients. In the literature, success rates in tympanoplasties using temporalis fascia vary between 62% and 93.3%. 7,14 -16 Sheehy and Anderson reported successful results by 90.5%, Condy and Taylor by 82%, and Smith by 95.5%. 7 As a result of the study by Yılmaz et al, 14 the success rate of membrane holding was reported to be 82.4%. Gül et al 17 reported the graft success in temporalis fascia as 74.1% in their study.
Van Baarle et al 18 demonstrated a relationship between the age of surgery and graft success in one of their studies. They found that the rate of membrane retention was reduced in patients younger than 15 years and older than 45 years, and the best result was obtained between 15 and 45 years of age. The age range of the patients included in our study was 15 to 50, and we had 6 patients over 45 years of age. Therefore, no relationship could be established between age and graft success. Similar to our study, there was no significant difference between gender and graft success in a study by Yilmaz et al. 14
When the results of studies investigating the effect of the location of perforation on graft success are examined, graft success in central perforations is better than anterior and total perforations. 7 In our study, when the relationship between perforation location and membrane holding was evaluated, no statistically significant relationship was found, and graft success was highest in central perforation with 60.3% and lowest in total perforation. In their study Adkins and White 19 found that the success of membrane holding in total perforations were lower than others. Tatlıpınar et al 7 reported 80% success rate in central and posterior perforations in their study.
In the evaluation of functional gain after tympanoplasty, the gain of airway PTO between 500 to 4000 Hz was found to be 8.67 ± 5.78 dB. Yılmaz et al 14 found the PTO gain as 8.3 dB, Gül et al 17 as 7.7 dB, Van Baarle et al 18 as 10 dB, Khan 20 as 7 dB. In the study by Tatlıpınar et al, 7 the average threshold gain was reported as 9.86 ± 10.87 dB. The results of our study were evaluated in accordance with the literature. In our study, the medial or lateral sides of the TMF used in type 1 tympanoplasty surgery were applied separately, and the graft application and graft inactivity and graft take and air-bone gap closure were evaluated.
When the graft success rates were examined in group 1 and group 2, which were separated according to the surgical technique, they were found to be 51.7% in group 1 and 48.3% in group 2, and no significant relationship was found between the groups and graft success (P = .72). Similarly, in terms of functional gain, mean airway threshold gain was similar in both groups, and there was no statistical significance between them. We could not find a similar study in the literature. Therefore, no comparison could be made.
There were some limitations to this study. First, in the current study, patients were followed up to the sixth postoperative month. Evaluation of longer follow-up results such as 1 year will yield more valuable outcomes. Second, the tympanic membrane perforation sizes of the patients were variable. Perforation locations were specified, but no comparison was made according to perforation dimensions in the current study.
Conclusion
In our study, we observed that there is no difference in the anatomical success of the graft and functional gain of hearing as a result of the application of this method in type 1 tympanoplasty (myringoplasty) surgery. We have performed such a study to show our physicians who are interested in otology that the results of medial or lateral surface application of TMF are not different from each other and to contribute to the literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.