
Abstract
Malignant proliferating trichilemmal tumor (MPTT) is a dermal adnexal tumor originated from the external root sheath of hair follicles. In this article, we reported a rare case of auricular MPTT in a 65-year-old male with gradually enlarging and bleeding mass on the right auricle measuring 30 × 20 × 12 mm in size and detailed the surgical strategy for therapy. The diagnosis of MPTT was established primarily by histopathological observation with abrupt keratinization, cytological atypia, abnormal mitoses, and infiltrating margins. Following extensive excision, no recurrence was noted for 14 months. We also discuss its clinicopathological features, differential diagnoses, and treatment methods and review the relevant literature in this regard.
Introduction
Proliferating trichilemmal tumors (PTTs) are rare dermal adnexal tumors derived from the outer root sheath of hair follicles 1 and were first described in 1966 by Wilson-Jones. 2 They usually arise on the scalp of women.1,3,4 Although most PTTs are benign, they have the potential for malignant transformation. When characterized by cytological atypia, abnormal mitoses, and infiltrating margins, they are defined as malignant proliferating trichilemmal tumors (MPTTs, also termed malignant proliferating trichilemmoma).3,5 MPTT is very rare, with only a few hundred cases have been described in the English literature.5,6
Here, we present the first detailed surgical report for an MPTT of the auricular helix, thereby raising the awareness of this rare tumor. We also review its diagnosis and treatment.
Case Report
A 65-year-old man presented to the ENT department with a 4-year history of a gradually enlarging bleeding mass on the right auricle without history of trauma, insect bite, or primary cancer. There was no history (personal or family history) of malignancy. The patient had diabetes mellitus, hypertension, and uremia (post-renal transplantation status) and consuming insulin, valsartan, cyclosporine, and mycophenolate mofetil on a daily basis. On physical examination, a 30 × 20 × 10 mm non-tender, rough, and dark-colored mass with irregular borders was observed on the right auricular helix (Figure 1A). Complete excision of the mass was performed, and frozen biopsy showed a cutaneous adnexal tumor with cancerous risk. Considering the post-operative shape of the auricle, we performed an extended excision with 0.5-mm surgical margins of normal skin and cartilage (Figure 1B). He was then followed up for 14 months, and no recurrence has been noted till date (Figure 1C). (A) The clinical view of the malignant proliferating trichilemmal tumor on the right auricular helix. (B) Post-operative view of the right auricle. (C) The status of right auricle after 14 months.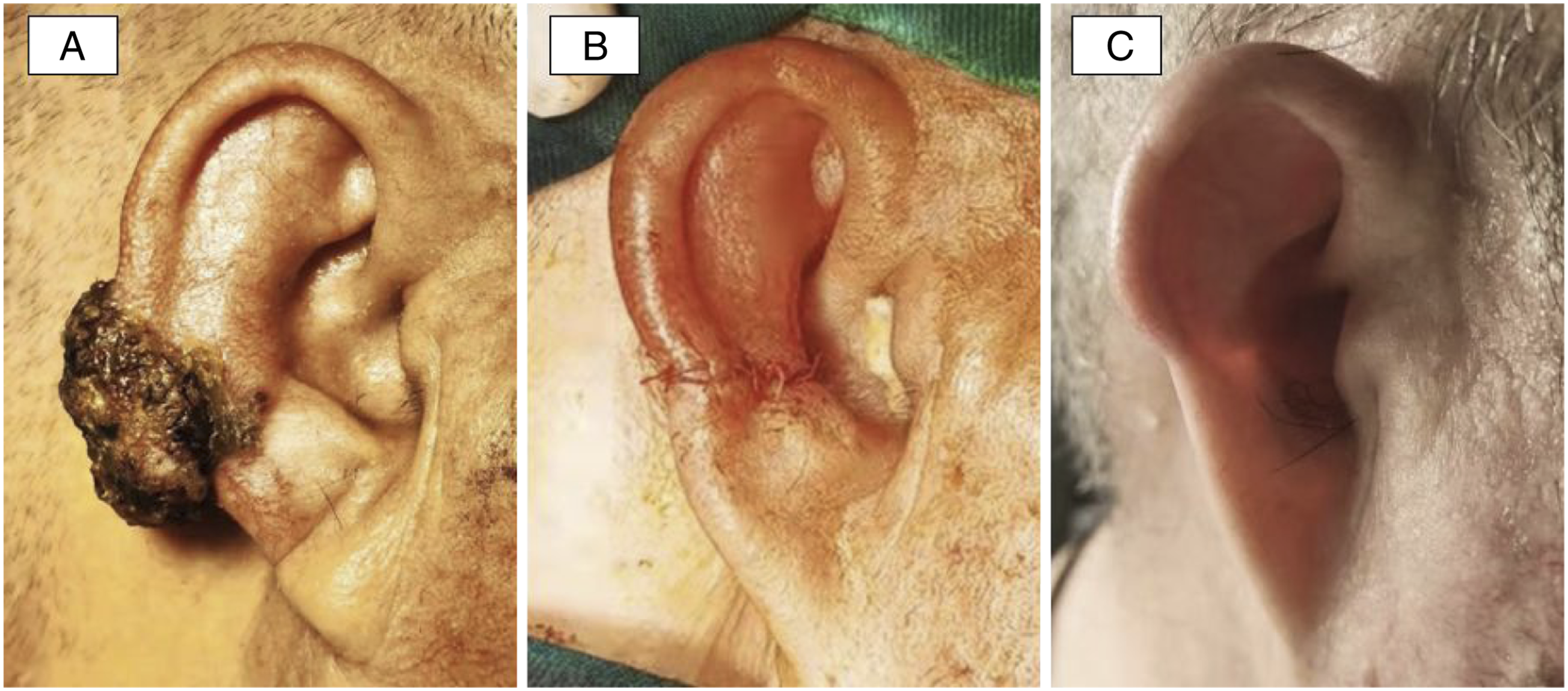
On histopathological observation, the gross specimen was 30 × 20 × 12 mm in dimensions, dark yellow-to-red in color, and had a rough surface with soft, gray, and white-to-tan appearance. Microscopically, we observed lobular and trabecular structures, including cystic and amorphous eosinophilic keratin. Tumor necrosis, cytological atypia, and mitotic figures were also observed in some areas (Figure 2). Circle shape surrounds the epithelial nest. The triangle indicates central keratinization. Arrows point to regions of atypical mitosis (H-E stain, ×40).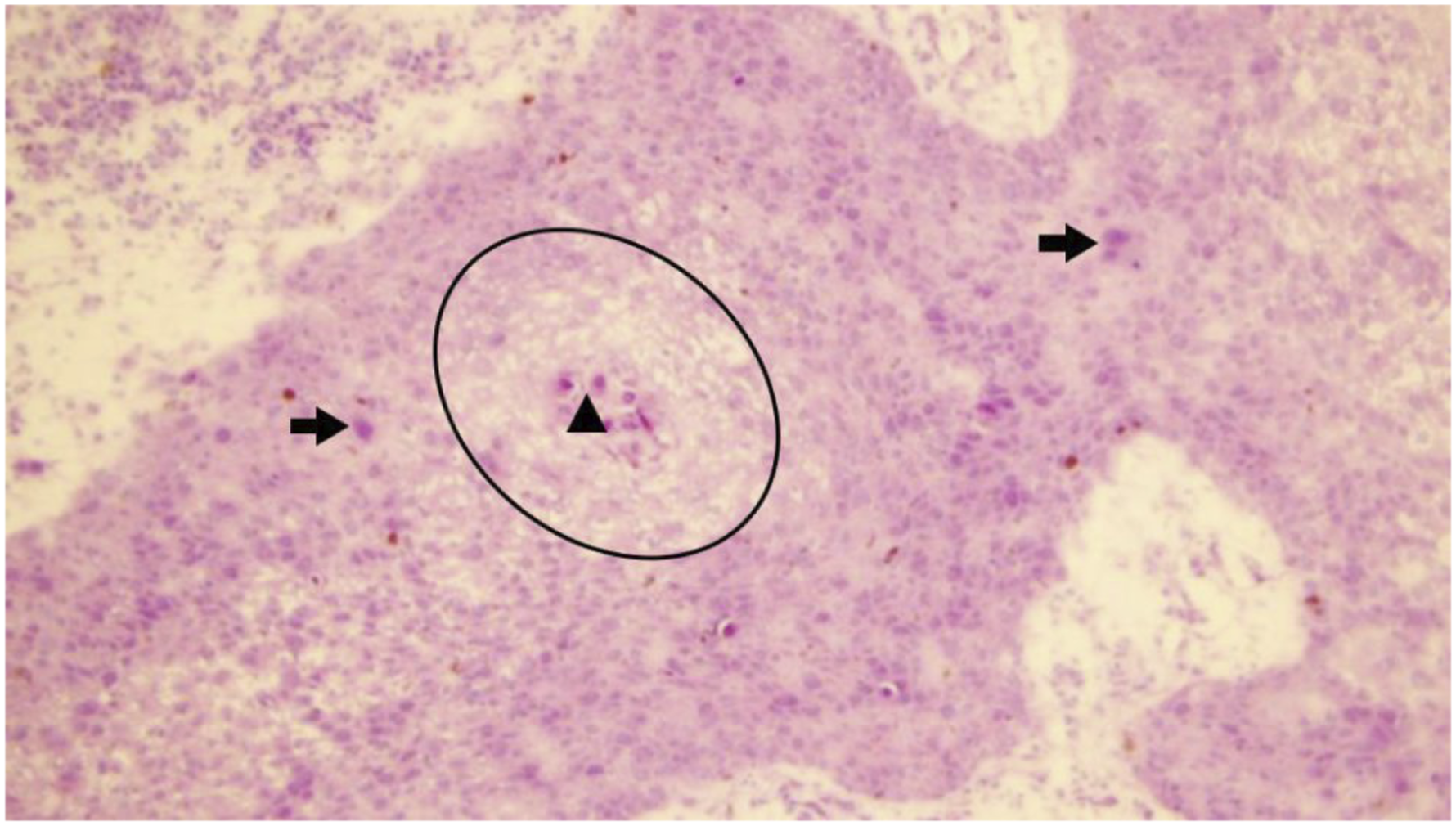
Discussion
Proliferating trichilemmal tumors usually appear on the scalp in the fourth to eighth decades of life in women. 7 Although the pathogenesis remains unclear, human papilloma virus, chronic inflammation, and trauma are known triggering factors. 1
Although most PTTs are benign, they have the potential for malignant transformation, and in this case are termed as MPTTs. MPTT accounts for <0.1% of skin cancer. 7 MPTT usually develops over preexisting benign proliferating trichilemmal cysts, although it can also occur de novo without a precursor lesion. 8 Since it originates from the external root sheath of hair follicles, it is very unlikely to develop from lanugo in bald men or from non-terminal hair follicles. 7
The diagnosis of MPTT is challenging and easily confused with that of squamous cell carcinoma (SCC) because of their similar malignant biological properties, location, and histology. Tejas et al. (2021) affirmed that no immunohistochemical marker is consistently and specifically expressed to reliably diagnose MPTT, although CD34 and Ki-67 phenotypes are of great utility in characterizing tumor behavior. 6 MPTT can be distinguished from SCC by histopathological examination owing to the presence of abrupt trichilemmal keratinization, lobular growth pattern of squamous epithelium with significant nuclear and cytoplasmic atypia, high mitotic index, and necrotic areas.7,9 Gallant et al. (2019) revealed that the sequencing data of SCC and MPTT are genetically distinct and could potentially be differentiated with a gene signature. 5 Pilomatrix carcinoma is another rare malignant hair follicle tumor that should be differentiated from MPTT. Pilomatrix carcinoma typically presents as a non-tender, firm dermal swelling in the head and neck regions, and they show proliferating atypical basaloid cells with an infiltrating border without multiple lobulated and bosselated expansive masses of squamous epithelium on histological examination.7,10
Since MPTT is very rare, there are no established guidelines for its treatment; however, surgical resection with a 1-cm margin is generally recommended. 6 Considering the post-operative craniofacial appearance, surgeons should carefully manipulate the resection margins. In our report, the MPTT was localized on the auricular helix, where there was a lack of subcutaneous tissue. Furthermore, the extensive excision caused high skin tension and increased the difficulty in suturing. This patient underwent extended excision with 0.5-mm surgical margins, and no recurrence has been noted for approximately 14 months. Some researchers have recommended aggressive therapeutic measures such as nodal dissection, radiotherapy, or chemotherapy, in addition to wide local excision; however, there are no randomized controlled studies demonstrating their feasibility and effectiveness of the former strategies.3,7 Even after complete excision, MPTTs can recur, thereby emphasizing the need for follow-up.
Conclusion
Malignant proliferating trichilemmal tumor typically presents as a rare and rapidly growing adnexal tumor. Histopathological examination is crucial for the differential diagnosis of MPTT, which is characterized by abrupt keratinization, cytological atypia, abnormal mitoses, and infiltrating margins. Extensive surgical resection is the recommended treatment, with close clinical follow-up for early detection of recurrence and metastases. As MPTT is extremely rare, our report adds to the knowledge on this condition. Further accumulation of data on MPTT is needed to unify the characteristics of the condition and identify the appropriate treatment strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by a grant from the Youth Medical Talent Training Program of Pudong Health Bureau of Shanghai (PWRq2020-50), the Academic Leader Program of Pudong Health Bureau of Shanghai (PWRd2018-05), the Scientific Research Program of Shanghai Municipal Health Commission (202140405), the Key Specialty Construction Project of Health Bureau of Shanghai (ZK2019C06), and the Talent Training Program of Pudong New Area Gongli Hospital (GLRq2020-01).
Research ethics and patient consent
This is a retrospective case report. Approval for the release of data for this project was conducted according to the World Medical Association Declaration of Helsinki and granted by the Ethical Committee of Shanghai Pudong New Area Gongli Hospital. This patient provided written informed consent.