
Abstract
Keywords
A 78-year-old man presented with a 2.0 × 1.5 cm2 recurrent cutaneous basal cell carcinoma of the left postauricular sulcus. Clear margins could not be obtained via MOHS due to marked subclinical extension. He was taken to the operating room for excision of 2/3 of his left auricle including the entire middle and lower thirds, left superficial parotidectomy, and wide local excision of his left postauricular and upper neck skin. The final tissue defect measured 8.0 × 9.0 cm2 and was covered with a supraclavicular island flap. Pathology revealed perineural invasion, so he subsequently underwent 60 gray of adjuvant radiation.
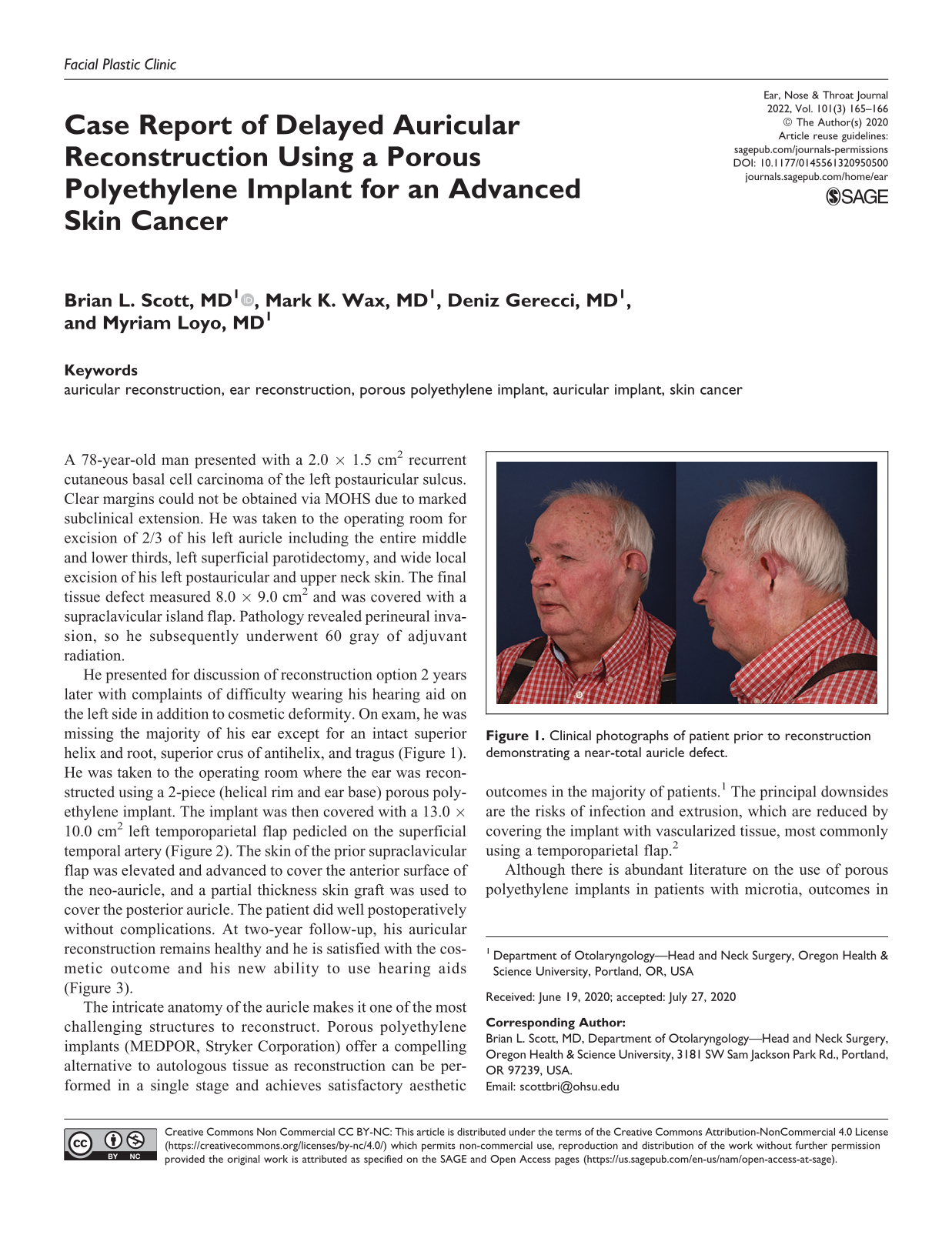
He presented for discussion of reconstruction option 2 years later with complaints of difficulty wearing his hearing aid on the left side in addition to cosmetic deformity. On exam, he was missing the majority of his ear except for an intact superior helix and root, superior crus of antihelix, and tragus (Figure 1). He was taken to the operating room where the ear was reconstructed using a 2-piece (helical rim and ear base) porous polyethylene implant. The implant was then covered with a 13.0 × 10.0 cm2 left temporoparietal flap pedicled on the superficial temporal artery (Figure 2). The skin of the prior supraclavicular flap was elevated and advanced to cover the anterior surface of the neo-auricle, and a partial thickness skin graft was used to cover the posterior auricle. The patient did well postoperatively without complications. At two-year follow-up, his auricular reconstruction remains healthy and he is satisfied with the cosmetic outcome and his new ability to use hearing aids (Figure 3).

Clinical photographs of patient prior to reconstruction demonstrating a near-total auricle defect.
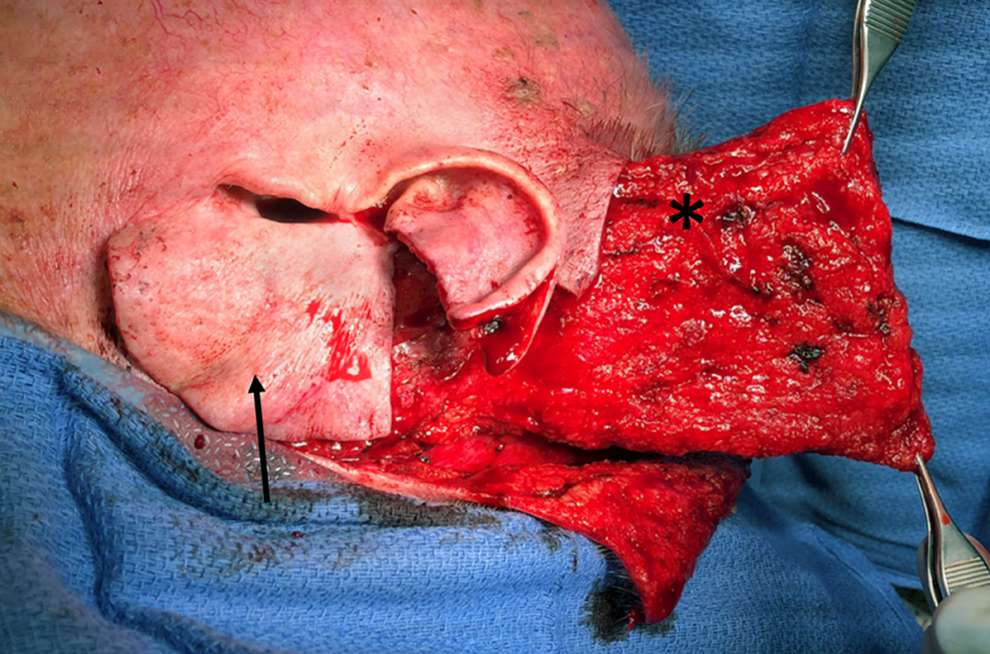
Intraoperative photograph demonstrating advancement of the prior supraclavicular skin flap (arrow) and elevation of a temporoparietal flap (asterisk).

Clinical photographs of patient at two years post-reconstruction using a MEDPOR porous polyethylene implant, advancement flap, and split thickness skin graft.
The intricate anatomy of the auricle makes it one of the most challenging structures to reconstruct. Porous polyethylene implants (MEDPOR, Stryker Corporation) offer a compelling alternative to autologous tissue as reconstruction can be performed in a single stage and achieves satisfactory aesthetic outcomes in the majority of patients. 1 The principal downsides are the risks of infection and extrusion, which are reduced by covering the implant with vascularized tissue, most commonly using a temporoparietal flap. 2
Although there is abundant literature on the use of porous polyethylene implants in patients with microtia, outcomes in patients with acquired deformities of the ear are scarce. 3 Our patient posed a particularly unique case as the ear and neck skin had been previously irradiated. Ionizing radiation is known to alter the vascularity of tissue, induce fibrosis, and leads to poor tissue healing.4-5 While it would be reasonable to hypothesize that radiation would lead to higher rates of auricular implant extrusion, poor skin graft take, or poor wound healing, there is insufficient data in the literature to draw conclusions. Our patient did not have any of these complications, despite the additional challenge of having to advance his prior supraclavicular flap to cover the anterior surface of the ear rather than relying on native skin.
We feel that this case is an important contribution to the literature as it demonstrates that porous polyethylene implants may still be a good option for auricular reconstruction despite prior radiation therapy to the surgical site and need for recruitment of non-native skin for implant coverage.
Footnotes
Authors’ Note
The patient provided written consent for publication of protected health information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.