
Abstract
Proliferating pilar tumors are rare, benign, exophytic neoplasms, which can closely resemble a squamous cell carcinoma. We describe a patient with a large benign exophytic tumor on the scalp that had been slowly growing over 10 years. While this class of benign follicular tumors is rare, the standard of care is typically excision with clear histologic margins. In this case, this large scalp tumor was surgically excised with clear margins/permanent section margin control using “Slow Mohs” technique, with subsequent repair using a skin substitute dressing, followed by a delayed skin graft.
Keywords
Introduction
Proliferating pilar tumor (PTT) is a rare, benign, exophytic tumor that may sporadically proliferate from a preexisting trichilemmal cyst. 1 These tumors can also arise de novo and they may clinically resemble a squamous cell carcinoma. 2 PTTs are benign follicular tumors that are classified under infundibular and/or isthmic differentiation, where the infundibular epithelium is indistinguishable from adjacent epidermis. 2 It is characterized histologically as a partially cystic and solid lesion with increased keratinocyte size, abrupt keratinization, and the absence of a granular layer. 2 They are more commonly observed in women over the age of 40, and 90% of cases are located on the scalp. 3 Rarely, PTTs may differentiate into a malignant neoplasm, with the potential for metastasis.1,2 Wide local excision is the standard of care due to the potential for recurrence and risk of malignant transformation. 1 As these tumors have the potential to grow large and lead to a significant surgical defect, the use of excision with margin control, such as Slow Mohs micrographic surgery technique, has the potential to be tissue-sparing.
Case report
A healthy 77-year-old woman presented with a 5-cm pink, dome-shaped, eroded exophytic tumor, over her right parietal scalp that had been slowly growing for 10 years (Figure 1). The tumor was excised under local anesthesia, using a Slow Mohs technique with permanent section margin control. The entire tumor was resected en bloc, with 8-mm lateral margins, and deep margins down to pericranium (Figure 2). A Xeroform (Covidien, Mansfield, MA) bolster dressing was secured over the wound and the patient was referred to a plastic and reconstructive surgeon to discuss options for closure.
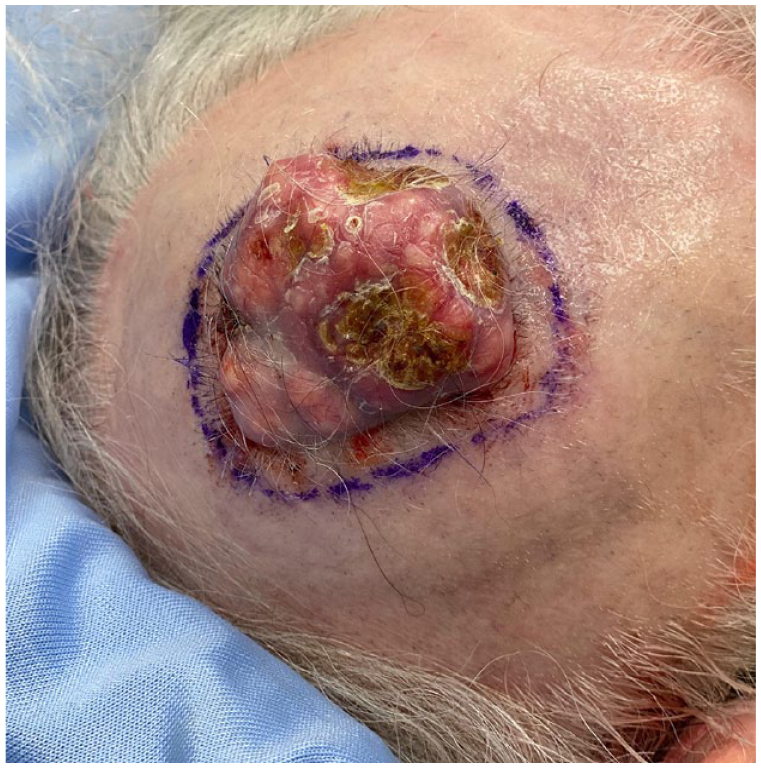
Pre-excision of PPT.

Defect post-excision.
Permanent section pathology revealed a keratinizing tumor with symmetrical architecture and a circumscribed, pushing border. There were multiple areas of abrupt keratinization, cystic ulceration, and calcification, consistent with a benign proliferating pilar (trichilemmal) tumor (Figures 3 and 4).

Hematoxylin and eosin stain showing the smooth pushing edge of proliferating pilar tumor at 20× magnification.

Hematoxylin and eosin stain showing the abrupt keratinization of proliferating pilar tumor at 200× magnification.
Two weeks later, examination revealed desiccated periosteum with no granulation of the wound bed. The outer cranial table was burred to spongy bone (diploë) and covered with a collagen-glycosaminoglycan biodegradable matrix (Integra) (Integra Life Sciences, Princeton, NJ) (Figure 5). After 6 weeks, once the biodegradable matrix had fully vascularized, a split thickness skin graft was taken from the thigh and applied to the granulated wound bed. A tie-over bolster was then applied for 7 days. The skin graft adhered well and healed without any complications. The patient was happy with the final functional and cosmetic result, and there was no sign of recurrence of PTT at 7 months’ follow-up (Figure 6).

Wound bed with Integra application.

Healthy scar at 7 months’ follow-up.
Discussion
Most cases of benign PTTs located on the scalp involve patients who tend to be female and over the age of 55 years, with a few reports of patients being in their 20s.4–15 The average size of the tumors was approximately 5 cm in diameter.4–15
This case report is congruent with the typical patient profile for a benign PTT. Slow Mohs technique with meticulous, mapped, and oriented permanent section margin control, was used to excise the tumor, with histologic examination by a pathologist. A wide excision (with variable margins) is the standard procedure for removing benign PTTs according to the current literature, with over 75% of the case reports opting for this method.4–9,11–14 There are no formal recommendations for margin size and depth in removal of either benign or malignant PTTs. Consequently, the margin size among these cases tended to be arbitrary and considered to be surgeon dependent, with some stating 1 cm is sufficient while other articles proposed that 2 cm is ideal as a precaution to avoid local recurrence.4–9,11–14 Benign PTTs typically grow in size between 2 and 10 cm in diameter, but they have the potential of growing as big as 25 cm; by adding an additional margin size this will only create a larger defect and thus a more difficult closure. 3 In one report, radiotherapy was used to clear several small nodules on the scalp that were considered unresectable, after previous surgical removal. 10
Mohs micrographic surgery utilizes precise frozen section histologic margin control to remove skin cancers while maximizing tissue preservation. 16 “Slow Mohs” technique with mapped permanent section margin control was chosen for this large scalp PTT to ensure clear margins, preserve healthy tissue, and shorten the procedural time for the patient. There are few case reports of Mohs surgery for PTT in the literature. Tierney et al. 15 described Mohs surgery for a PTT, but due to the large defect size, a tissue expander was used for reconstruction. Alarcón et al. 5 described two cases of PTT treated with Mohs surgery, both with free margins after the second stage.
Complete excision of PTT is essential to avoid tumor recurrence. Rarely, PTT has the potential for malignant transformation, with ulceration, bleeding, rapid growth, infiltration into the outer cranial table, and potential metastases to the cervical lymph nodes. 4 Mohs micrographic surgery with frozen sections, or a modified Slow Mohs technique with permanent sections, has the advantage of histologic margin control for the removal of scalp PTT. Mohs surgery preserves functionally and aesthetically important scalp tissue, by examining all histologic margins, identifying any potential subclinical extensions of PTT, thereby reducing the risk of PTT recurrence. 16
Footnotes
Authors’ note
This work was presented at the Atlantic Provinces Dermatology Association Conference in June 2023 in Saint John, New Brunswick, Canada.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Informed consent was obtained by the patient, both in the form of verbal and written consent. This includes both patient information and images to be published for the educational purposes of this case report.