
Abstract
Amputations of the earlobe after a human bite are rare. But when they appear, they present a challenge for the plastic surgeon, due to its reconstruction since the earlobe is anatomically built only from skin and cartilage. In these cases, the retro auricular flap represents a perfect solution for reconstruction. We will present a 25-year-old man with amputation of the lower half of the earlobe, caused after a human bite injury. We have decided to reconstruct the amputated part of the auricle in 3 (acts) with a retro auricular flap. The skin is removed from the amputated part of the auricle and the (cartilage part) is implanted in the pocket created in the retro auricular region. Then in the second act, the retro auricular flap is raised with the previously implanted cartilage graft. By contrast, in the third act, the retro auricular flap is separated and the auricle defect is closed. The second defect is covered with a full skin graft. The reconstruction in 3 acts, delay procedure, of the auricle defects with retro auricular flap represents a satisfactory and very acceptable solution for the patient, not only from the reconstructive aspect but also from the aesthetic aspect.
Introduction
Although ear lobe amputations after human bites are rarely present, they are not only accompanied by functional and psychological consequences for the patient but also have aesthetic consequences. They are also a challenge for reconstruction since the earlobe as an anatomical structure consists from the outside only of the skin and of the cartilage, without the presence of subcutaneous fatty tissue.
The difficulty of reconstitution is mainly related to the unique anatomical structure of the auricle, with fine skin covering, thin and elastic cartilage, and small size vessels responsible for its perfusion.1,2 Baudet et al reported a case of successful ear replantation using a novel technique. Reattachment was accomplished by excising the posterior skin of the amputated part and making large fenestrations in the cartilage to allow better contact of the anterior skin to the underlying vascular bed. In addition, a postauricular flap was elevated. The anterior skin was then sutured to the amputated stump of the ear and the postauricular flap. 3
Other authors describe successful cases of the
Case Presentation
A 25-year-old man with the amputation of the earlobe as a result of a human bite, after a conflict in the car park. The patient comes to the Emergency Center with amputation of the lower half of the left earlobe. The patient did not have the amputated part with him, but after we asked for it, a family member of the patient went to the scene, took it, and brought it to the emergency center (Figure 1). We put this part in a container with a cold physiological solution. Since it was about a bite wound, which is characterized by a high potential for infection due to the presence of a large number of bacteria in the human mouth, with the consent of the patient, we decided to perform the reconstruction of the amputated earlobe with retro auricular flap with delay procedure, in 3 acts.

Amputation of the lower half of the left earlobe after a human bite.
Initially, in the first act, in the operating room of the emergency center, we removed the skin part and de-skinned the amputated part of the ear leaving only the cartilage part. Then we make an incision of about 2 cm in the auriculo-mastoid groove and prepare the skin in the retro auricular part to create the pocket where the amputated auricular cartilage will be placed. The skin is prepared at the subcutaneous level, without subcutaneous adipose tissue so that this skin part is as thin as possible and corresponds to the normal skin of the earlobe. The edges of the pocket are made parallel to the edges of the amputated part of the earlobe (Figure 2). At the end, the cartilage graft is inserted into this pocket, while the wound is closed with direct sutures. Likewise, the auricular defect is closed with direct situational sutures. The patient is prescribed an antibiotic (oral), to protect the wounds from possible infection, and an analgesic.

The retro auricular pocket creation in which the de-skinned cartilaginous graft is inserted.
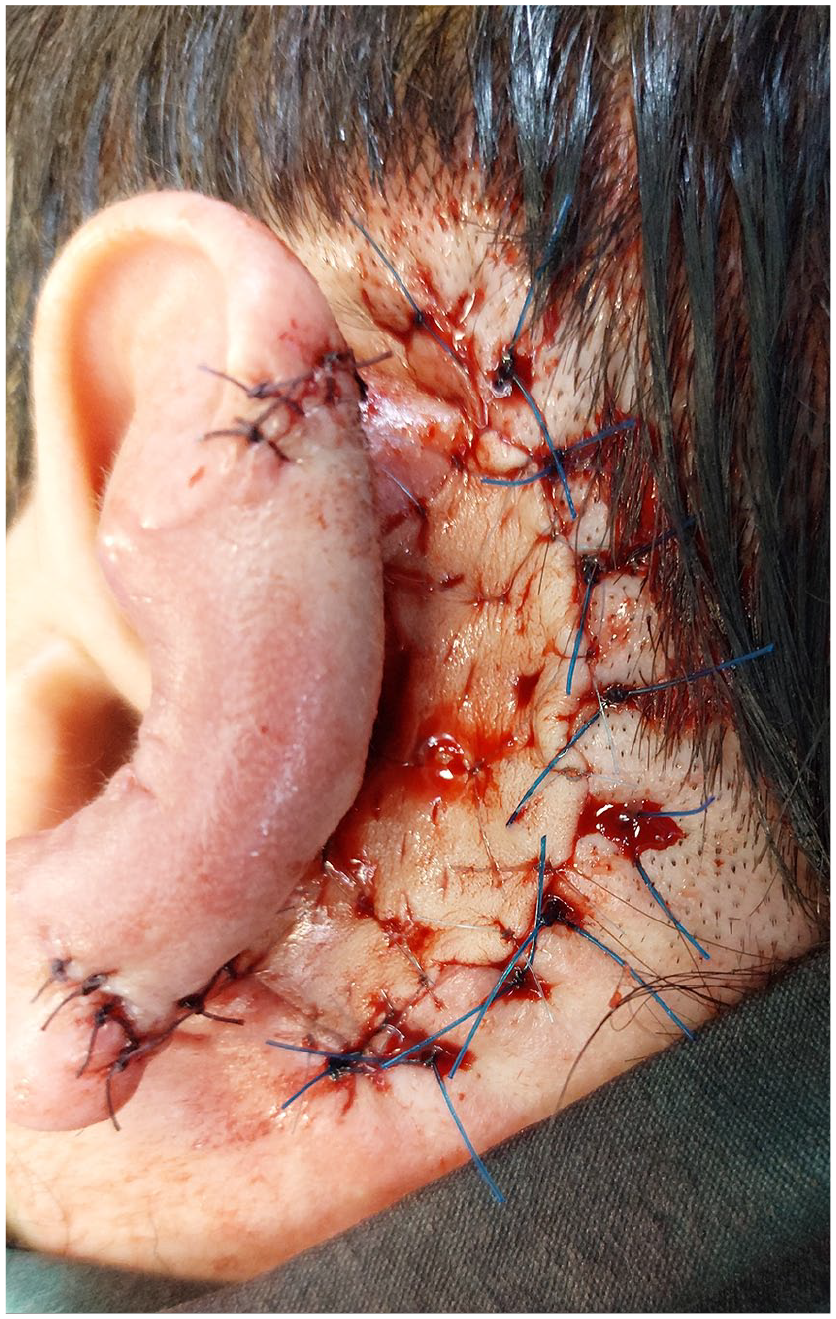
After 3 weeks, in the second act, after marking, we begin to raise the retro auricular flap after marking the skin in the retro auricular part to the same size as the auricular defect. Together with the flap, adjacent to it, the auricular cartilage graft, implanted earlier, also rises. Then the edges of the auricular defect are excised, removing the skin parts to expose the cartilage partially. First, the cartilage implanted in the retro auricular flap is sutured with the (cartilage) of the auricular defect, and then the anterior skin edges of the flap are sutured with the anterior skin of the auricular defect, to enable the covering of the (cartilage) parts with the retro auricular flap (Figure 3). The postoperative course was good, without complications.

Appearance of the retro auricular flap with which the auricular defect is covered.
After 4 weeks, in the third act, the retro auricular flap is separated, with which the auricular defect is covered (the front and back part of the amputated cartilage). The secondary defect (retro auricular wound) is covered with a full skin graft, taken from the inside of the left arm (Figure 4). The wound on the left arm is closed with direct sutures. Even in this case, we had no postoperative complications, with a well-vascularized retro auricular flap and acceptance of the complete skin graft. With this reconstruction of the amputated earlobe with retro auricular flap, we have achieved a satisfactory aesthetic result that is also acceptable to the patient (Figure 5).
Separation of the retro auricular flap and coverage of the secondary defect with a full skin graft.

Earlobe’s appearance was 4 months post-op.
Discussion
It should be taken into consideration that the reconstruction of traumatic defects of the earlobe is not easy for the plastic surgeon because the earlobe is anatomically made of thin skin and thin and elastic cartilage. Therefore, finding an adequate reconstructive tissue material that satisfies the aesthetic demands of the patient represents a challenge for the reconstructive surgeon. A good reconstructive solution offers retro auricular flap, reconstruction performed in separate acts of operation. Also, when earlobe defects are the result of a human bite, it should be taken into account that they are colonized with bacteria from the human mouth. Therefore, this possibility of infection has prompted us to perform the reconstruction of the amputated earlobe through retro auricular flap in 3 stages.
The use of retro auricular skin flap for the reconstruction of auricle defects was described since the beginning of the last century when Gillies in 1920 originally proposed the retro auricular skin flap. 7 Over the years, many operative techniques have been described for the complete reconstruction of the auricle, such as Tanzer in 1959 who described the use of costal cartilage graft. 8 Godwin et al present a patient, who had two-thirds of his external ear bitten off and was treated successfully by replacing the part as a composite graft. The segment replanted was minimally trimmed but inset to allow maximal soft tissue apposition at the skin edges. 4 Kyrmizakis et al present 2 cases, 1 of a partial and 1 of a total traumatic auricular amputation, both caused by human bites. The technique of ear reattachment as a composite graft, with the partial burial of the amputated part in the post-auricular region, as first described by Baudet, was followed in both cases. It is a simple technique, without the need for microsurgery, and produces excellent aesthetic results. 9 As well Hajebian et al describe a case of a pediatric total auricular avulsion following a dog bite, and effective reconstruction which can be achieved using a 2-stage technique of native cartilage lamination via posterior auricular pocket formation and placement of a skin graft. 5
Conclusion
In conclusion, our technique for reconstructing auricle defects with retro auricular flap in 3 acts, delay procedure, after a human bite represents a good reconstructive solution, perhaps long in time, but with a very satisfactory reconstructive outcome and to be accepted by the patient. This technique fulfills the reconstructive requirements both in the aesthetic and psychological aspects of the patient, avoiding the possibility of infection from the initial contamination of the wound with the bacterial flora of the human mouth.
Footnotes
Author Contributions
Both authors declare that we have made a significant contribution to the naming, conception, design, and completion of this article.
Data Availability Statement
All data of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written consent from the patient was obtained in this article.