
Abstract
Fungus ball is a common disease encountered in rhinology departments. As it usually affects immunocompetent patients, other systemic diseases occurring concurrently with fungus ball have not been reported often. Recently, we encountered a patient who was diagnosed with fungus ball in the maxillary sinus and underwent endoscopic sinus surgery. During the surgery, fungus ball-like materials were sucked out and a maxillary sinus mucosal biopsy was performed. The post-operative pathologic report demonstrated that there were many plasma cells; the patient underwent several additional tests in our hematologic department. Finally, he was diagnosed with monoclonal gammopathy of undetermined significance (MGUS). In the present report, we summarize our experience with this patient and share the lessons that we have learned from this case.
Introduction
Fungal spores are present in the surrounding air and the respiratory mucosa is continuously exposed to fungal spores. However, fungal spores rarely behave as pathogens in the sinonasal cavity of healthy individuals. 1 It has been reported that fungal rhinosinusitis is encountered in about 10% of patients requiring sinonasal surgery.1,2 Fungal rhinosinusitis can be classified into the invasive and non-invasive forms based on the presence or absence of microscopic fungal hyphae within the tissues. Invasive fungal rhinosinusitis is usually considered in immunocompromised patients; non-invasive rhinosinusitis includes fungus ball and allergic fungal sinusitis.1,3 Fungus ball does not invade the sinus mucosal tissues; the removal of the fungus ball by endoscopic sinus surgery (ESS) is adequate for treating most cases. Recently, we encountered a patient with fungus ball in the maxillary sinus. After surgery, pathologically, many plasma cells were reported in the sinus mucosa in which the fungus ball was present; we decided to transfer the patient to the hematologic department. He underwent hematologic evaluation, and finally, the diagnosis of monoclonal gammopathy of undetermined significance (MGUS) was confirmed. Although we have previously reported many cases of fungus ball, this was the first time that a concurrent diagnosis of MGUS based on sinus mucosal tissues was made in our institute. Therefore, we introduce this case and review the pathological characteristics of fungus ball reported in previous literature.
Case Report
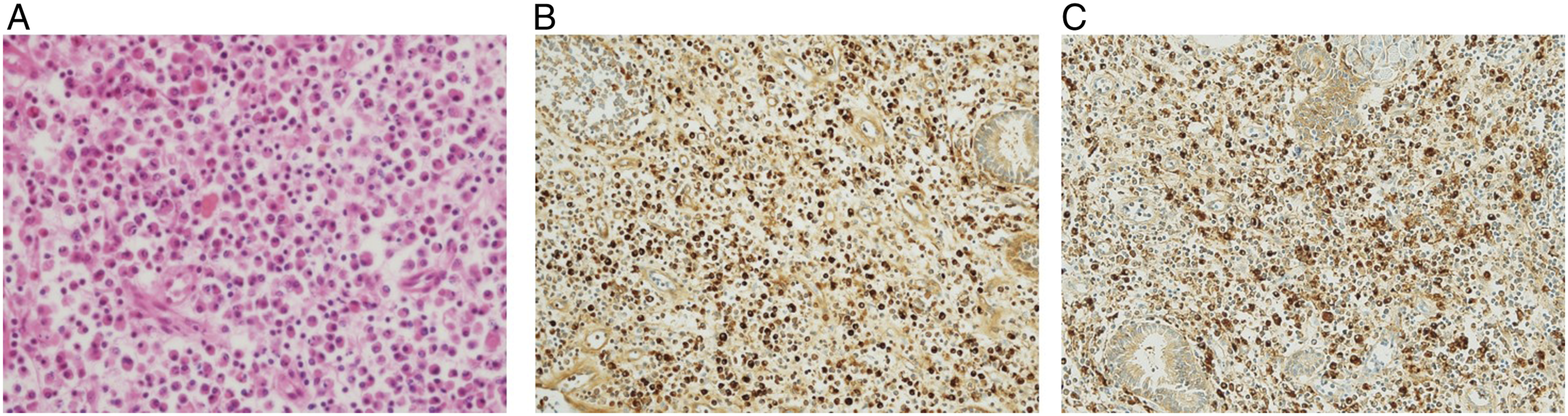
A 74-year-old man presented to the otorhinolaryngology department of our institute with a history of nasal discharge for several years. He had previously been diagnosed with hypertension and hypercholesterolemia. The rest of his medical history was unremarkable. The nasal endoscopic examination revealed no definite nasal discharge in both nasal cavities. Paranasal sinus computed tomography (PNS CT) was performed; the right maxillary sinusitis showed a high-density core and calcification, which was suggestive of fungus ball (Figure 1A). An ESS was planned under general anesthesia. During the ESS, fungus ball-like materials were removed and a maxillary sinus mucosal biopsy was performed. According to the post-operative pathologic report, fungal ball-like materials were reported to represent the fungus (Figure 1B). Additionally, the mucosal sample was reported to show “too many plasma cells (Figure 2A) and positive immunohistochemical staining results for the kappa and lamda light chain (Figure 2B, C).” We transferred the patient to the hematologic department of our institute, where he underwent several tests, including serum protein electrophoresis, serum immunofixation electrophoresis, and bone marrow biopsy. The hematologic evaluation yielded the following results: serum β2 microglobulin level, 2.34 mg/L; random urine β2 microglobulin level, 0.16 mg/L; and serum M-protein level, 0.6 g/dL. The results of the bone marrow biopsy showed that plasma cells constituted 4% of the total proportion of cells observed, and no definite evidence of plasma cell tumors such as plasma cell myeloma was found. The patient was finally diagnosed with MGUS. Until three years after the final diagnosis, he has not developed any other hematologic malignancy or sinonasal diseases. Fungus ball in right maxillary sinus: (A). Paranasal coronal CT demonstrates suspicious lesion of fungus ball in right maxillary sinus. (B). Pathological image confirming the lesion was corresponding to the fungus ball (magnification, 40×). Histopathologic evaluation of fungus ball–affected sinus mucosa: (A). Many plasma cells are identified in the affected sinus mucosa. (B). Immunohistochemical staining result for positive kappa light chain in the affected sinus mucosa. (C). Immunohistochemical staining result for positive lambda light chain in the affected sinus mucosa (magnification, 200×).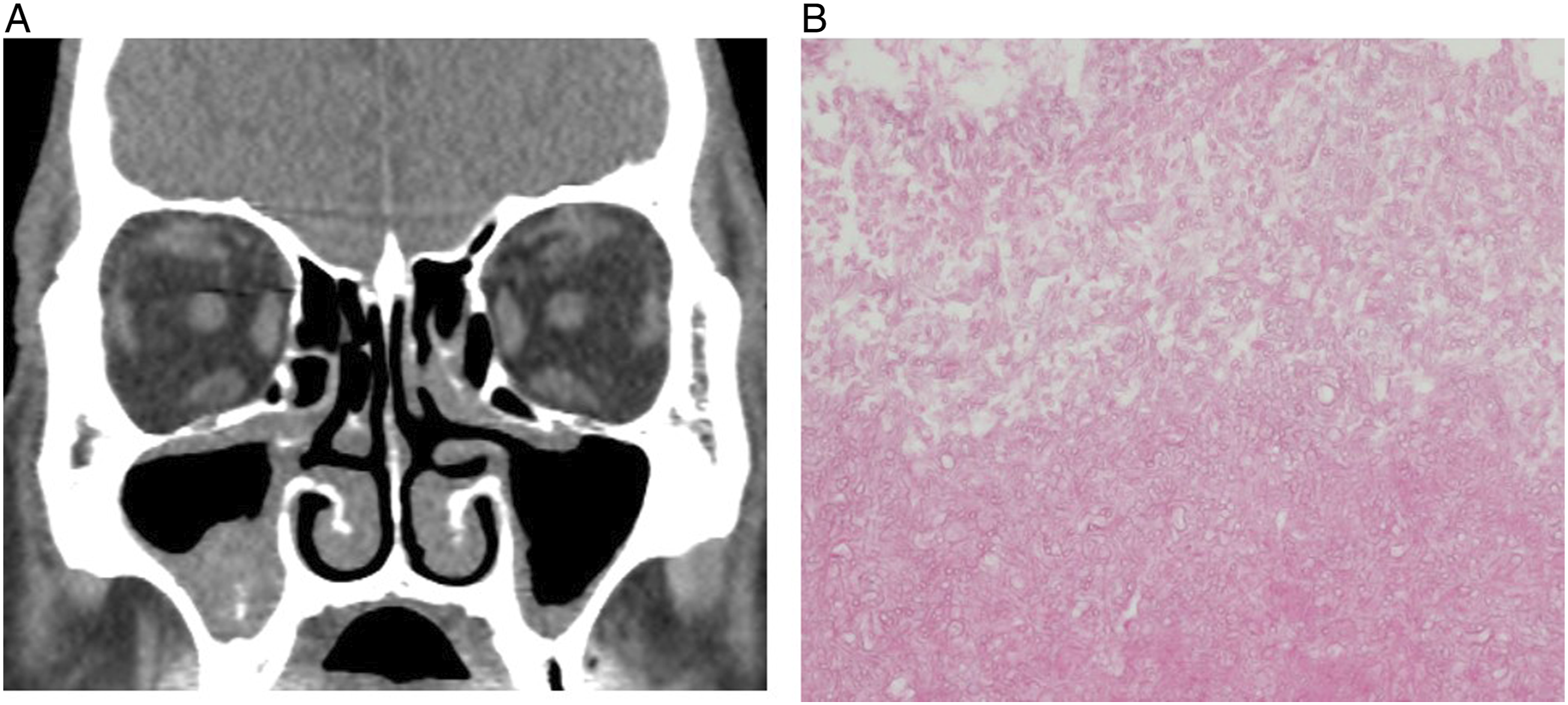
Discussion
Fungus ball in the paranasal sinuses is defined as the non-invasive accumulation of dense fungal material in the sinus cavity; the maxillary sinus is the region that is most commonly affected by this condition. The most common clinical presentation of fungal ball is non-symptomatic, with non-specific symptoms, such as nasal obstruction, purulent nasal discharge, facial pain, and chronic cough. 4 Therefore, fungal ball is usually diagnosed incidentally during imaging studies. The presentation of this condition in a characteristic computed tomography (CT) scan includes typically heterogeneous opacities associated with a metal-dense spot in the involved sinus cavity. Our patient showed no specific symptoms; opacification with metal density limited to only the unilateral maxillary sinus, as observed in the PNS CT analysis, was the evidence for the diagnosis of fungal ball.
It has been reported that although fungal material exists for long durations in the sinus cavity, the sinus mucosa shows little inflammatory change. This drives the notion that the complete surgical removal of the fungal material, usually by ESS, is a sufficient curative modality for this condition. 3 However, compared to the clinical review studies of fungus ball in sinonasal cavities, there have been very few studies evaluating the pathogenesis of the conditions associated with the immunologic or histologic changes in sinus mucosal tissues after fungus ball infection. A previous study reported that the number of plasma cells in the fungal ball–affected sinus mucosa was markedly higher than that in the contralateral inferior turbinate. 1 Interestingly, the number of plasma cells in the mucosa of the inferior turbinate of the fungal ball–affected side was also significantly higher than that in the contralateral inferior turbinate. 1 However, the numbers of eosinophils and neutrophils in the affected sinus mucosa did not increase. In contrast, another study reported that macrophage and neutrophil infiltration in the nasal mucosa of fungus ball patients was notably high. Compared to the nasal tissues from control patients, mild eosinophil infiltration and predominant macrophage and neutrophil infiltration were the characteristic findings in the nasal tissues from fungus ball patients. 5 However, both these studies are based on a very limited number of samples (fewer than 10), and this could be reason for these contradictory results. Therefore, currently, normal histologic changes in fungus ball–affected sinus mucosa remain debatable. However, we recommend that for patients with fungal ball, a pathologic review of all the affected sinus mucosa tissues be carefully performed. The pathologic review of the affected sinus mucosa tissues of our patient revealed the presence of many plasma cells; accordingly, we decided to perform further evaluations of plasma cell–associated hematologic diseases. Thus, the patient was diagnosed with a plasma cell–associated hematologic disease, MGUS, at the early stage and was carefully followed up. Large population-based studies regarding the histologic characteristics of fungus ball–affected sinus mucosal tissues need to be performed in the future; this may enable the detection of cues for the early diagnosis of other concurrent systemic diseases in patients with fungal ball.
Footnotes
Author’s Note
Informed consent was obtained from the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statements
The datasets generated during and/or analyzed during the current study are not publicly available due to the patient’s privacy but are available from the corresponding author on reasonable request.