
Abstract
Significance Statement
We describe a rare occurrence of nodular fasciitis which was initially presented as submandibular lymphadenopathy. Since nodular fasciitis is often misdiagnosed as soft-tissue sarcoma, this case highlights the importance of morphology, location, and histology in newly diagnosed head and neck masses to distinguish between malignant and benign tumors.
Main Text
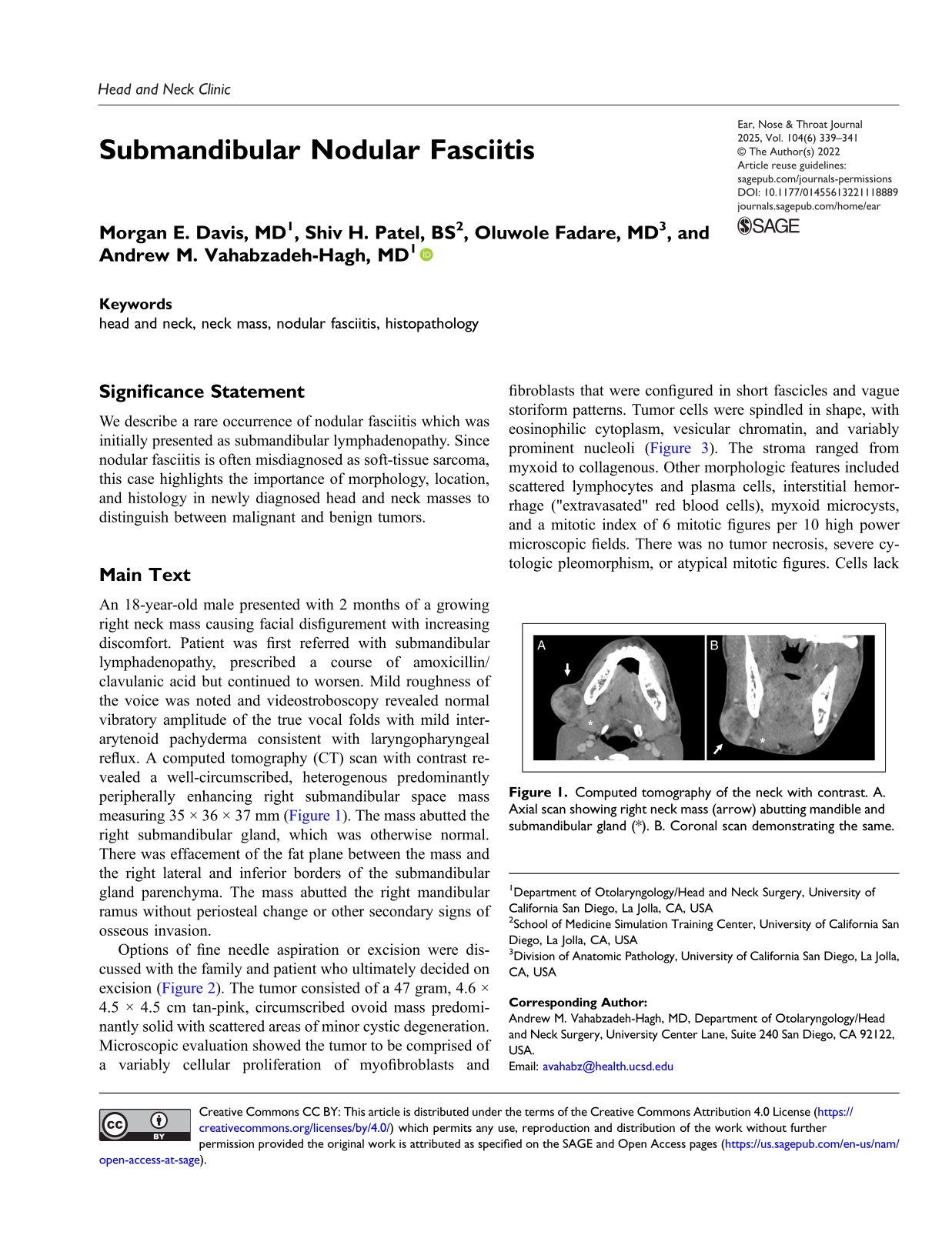
An 18-year-old male presented with 2 months of a growing right neck mass causing facial disfigurement with increasing discomfort. Patient was first referred with submandibular lymphadenopathy, prescribed a course of amoxicillin/clavulanic acid but continued to worsen. Mild roughness of the voice was noted and videostroboscopy revealed normal vibratory amplitude of the true vocal folds with mild interarytenoid pachyderma consistent with laryngopharyngeal reflux. A computed tomography (CT) scan with contrast revealed a well-circumscribed, heterogenous predominantly peripherally enhancing right submandibular space mass measuring 35 × 36 × 37 mm (Figure 1). The mass abutted the right submandibular gland, which was otherwise normal. There was effacement of the fat plane between the mass and the right lateral and inferior borders of the submandibular gland parenchyma. The mass abutted the right mandibular ramus without periosteal change or other secondary signs of osseous invasion. Computed tomography of the neck with contrast. A. Axial scan showing right neck mass (arrow) abutting mandible and submandibular gland (*). B. Coronal scan demonstrating the same.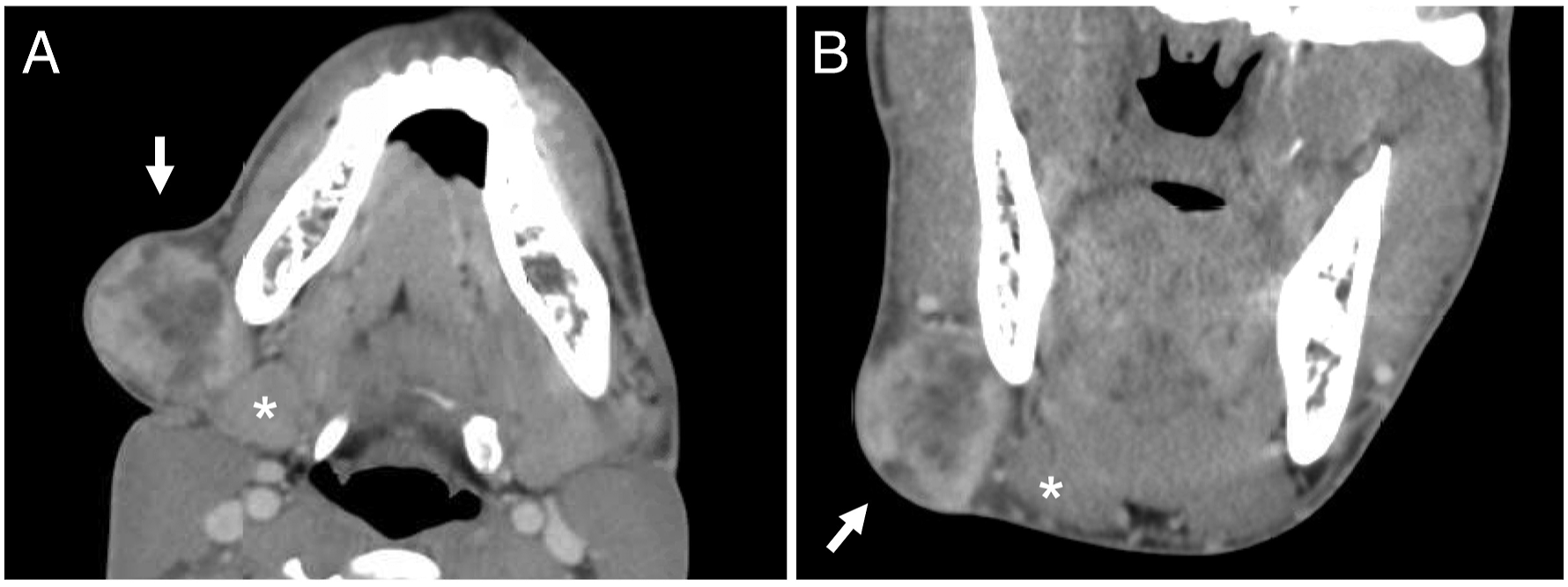
Options of fine needle aspiration or excision were discussed with the family and patient who ultimately decided on excision (Figure 2). The tumor consisted of a 47 gram, 4.6 × 4.5 × 4.5 cm tan-pink, circumscribed ovoid mass predominantly solid with scattered areas of minor cystic degeneration. Microscopic evaluation showed the tumor to be comprised of a variably cellular proliferation of myofibroblasts and fibroblasts that were configured in short fascicles and vague storiform patterns. Tumor cells were spindled in shape, with eosinophilic cytoplasm, vesicular chromatin, and variably prominent nucleoli (Figure 3). The stroma ranged from myxoid to collagenous. Other morphologic features included scattered lymphocytes and plasma cells, interstitial hemorrhage ("extravasated" red blood cells), myxoid microcysts, and a mitotic index of 6 mitotic figures per 10 high power microscopic fields. There was no tumor necrosis, severe cytologic pleomorphism, or atypical mitotic figures. Cells lack immunoreactivity for MUC4, S100, beta-catenin, and pancytokeratin, this phenotype excludes a variety of differential diagnostic considerations, and in conjunction with the observed morphology and location lead to a diagnosis of nodular fasciitis. Perioperative images of the mass. A. Preoperative image of the mass along the submandibular and perifacial regions. B. Intraoperative image of the mass prior to mass resection. C. Excised mass next to a measuring ruler. Representative image from case (hematoxylin and eosin preparation; original magnification, 100X): Spindled proliferation with a storiform architecture. The lower right field shows myxoid microcysts, interstitial hemorrhage, and inflammation.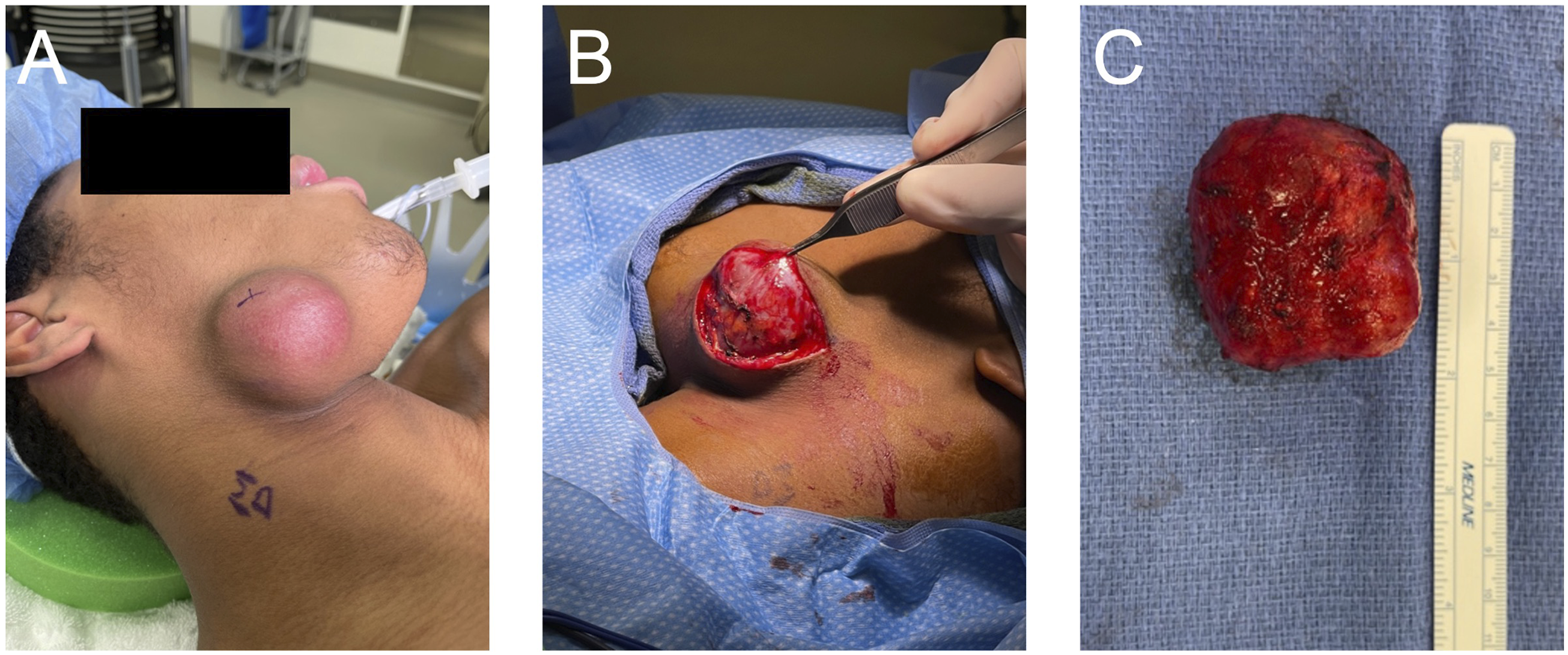
Nodular fasciitis is a rare benign soft tissue tumor that typically presents as a solitary subcutaneous mass in the extremities and head and neck region. 1 The differential diagnosis for a solitary neck mass is quite broad including neurofibroma, leiomyoma, epidermal cyst, basal cell carcinoma, keloid, desmoid tumor, Kaposi sarcoma, fibrosarcoma, dermatofibroma, sarcoidosis, as well as infectious etiologies such as tuberculosis lymphadenitis. Nodular fasciitis is a result of fibroblast and myofibroblast proliferation that is hard to distinguish from soft-tissue sarcomas. 2 The prevalence between men and women is equal and typically nodular fasciitis is diagnosed between 20 and 40 years of age while children only make up 10% of total cases. Although nodular fasciitis is most common in the extremities, around 16% of the cases are seen in the head and neck region, with children having a higher prevalence. The etiology of nodular fasciitis is still unclear, but there is some evidence that nodular fasciitis develops after a preceding trauma or infection. Studies have also linked recurrent USP6 gene rearrangements to nodular fasciitis supporting its classification as a benign neoplasm. 3,4 The most common course of treatment is surgical excision, but regression of the lesion has been reported following corticosteroid injection. 5 For complex nodular fasciitis cases where excision is higher risk and morbid, radiotherapy may be considered. 6
In the past, similar cases of nodular fasciitis have been reported. A retrospective review found 15 cases of head and neck nodular fasciitis over the course of 20 years at a tertiary pediatric care center. 1 While most nodular fasciitis cases are relatively straightforward to manage, one report showed an 82-year-old diagnosed with nodular fasciitis invading the trachea causing shortness of breath. 6 Management of this patient was difficult because excision would have required a laryngectomy which was not favorable in this case.
Here, we demonstrate a unique case of submandibular nodular fasciitis. A reminder of a favorable diagnosis in this young demographic. Given how rare nodular fasciitis is and its similarities to soft-tissue sarcoma, it can be challenging to diagnose. This case highlights the importance of a thorough work-up in newly diagnosed head and neck masses, assimilating knowledge of the location and morphology of the mass, cross sectional imaging, and histology to distinguish between a benign and malignant mass.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.