
Abstract
Nodular fasciitis is a benign myofibroblastic and fibroblastic proliferative lesion that can be found in the subcutaneous tissue, muscle, and fascia. It is frequently observed in young adults aged 20 to 40 years and less commonly in pediatric patients. Rapid growth, high cellularity, and remarkable mitotic activity of this lesion could lead to misdiagnosis as a soft tissue sarcoma. Here, two cases of nodular fasciitis in the preauricular area in pediatric patients were reported. Nodular fasciitis in the preauricular area in a pediatric patient is rare. It could be confused with soft tissue sarcoma. However, nodular fasciitis should be suspected in a pediatric patient with a rapidly growing mass in the head and neck region. Surgical excision should be performed to confirm the histopathologic diagnosis when clinical diagnosis is uncertain and there is possibility of malignancy.
Introduction
Nodular fasciitis is a benign myofibroblastic and fibroblastic proliferative lesion occurring in the subcutaneous tissue, muscle, and fascia.1-6 It occurs mostly in the upper extremities, followed by the trunk, lower extremities, and head and neck.1,7-9 Nodular fasciitis can appear at any age but is frequently observed in young adults aged 20 to 40 years and less commonly in pediatric patients.4,9,10 Rapid growth, high cellularity, and remarkable mitotic activity of this lesion could lead to misdiagnosis as a soft tissue sarcoma.2,3,5,7,11 Here, two cases of nodular fasciitis in the preauricular area in pediatric patients were reported.
Case Reports
Case 1
A 13-year-old female visited the otorhinolaryngologic clinic for a mass in the right preauricular area for several months which recently showed rapid growth. She had no history of trauma at the lesion. On physical examination, a 2 × 2-cm, nodular, hard, non-tender, pinkish mass was observed in the right preauricular area. The mass was not responsive to oral antibiotics administered for several days. In facial bone computed tomography (CT), a 2 × 2-cm, slightly enhanced, well-demarcated, round, necrotic mass was revealed at the subcutaneous layer in the right preauricular area (Figure 1). Thus, considering a benign or malignant tumorous lesion, surgical excision was performed. (A) A 2 × 2-cm, nodular, hard, non-tender, pinkish mass is observed in the right preauricular area. (B) Facial bone computed tomography reveals a 2 × 2-cm, slightly enhanced, well-demarcated, round, necrotic mass at the subcutaneous layer in the right preauricular area.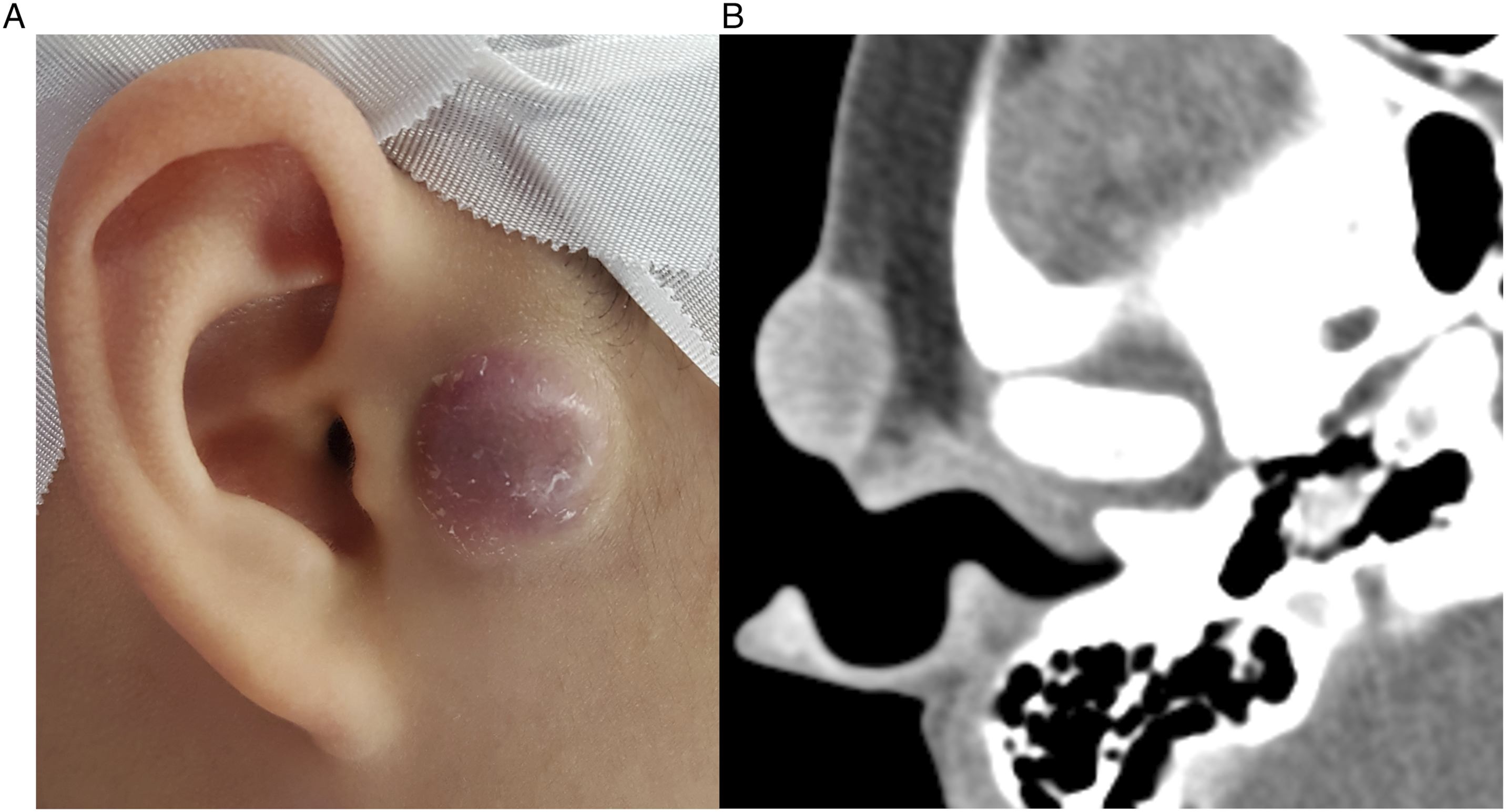
In surgery under local anesthesia, a skin flap was elevated, and a 2 × 2-cm, white mass was well defined from the surrounding tissue and completely removed. On histopathologic evaluation, spindle cell neoplasm with high cellularity was observed. However, highly cytologic atypical cells were absent. Immunohistochemical staining showed positivity for smooth muscle actin (SMA) and negativity for CD34, S100, and desmin. Thus, nodular fasciitis was diagnosed. At 6 months after surgery, the wound had healed well and there was no recurrence.
Case 2
A 7-year-old male visited the otorhinolaryngologic clinic for a mass in the right preauricular area due to rapid growth in the 2 weeks prior. He had no history of trauma at the lesion. On physical examination, a 2.5 × 2.5-cm, nodular, hard, non-tender, pinkish mass was observed in the right preauricular area. The mass was not responsive to oral antibiotics administered for several days. In neck CT, a 2.5 × 2.5-cm, slightly enhanced, well-demarcated, round, necrotic lesion was revealed in the right preauricular area. In neck magnetic resonance imaging (MRI), a same sized, well-demarcated, round, necrotic lesion was revealed in the right preauricular area with low signal on T1-weighted imaging and high signal on T2-weighted imaging (Figure 2). In a fine needle aspiration biopsy guided by ultrasonography, a few clusters of spindle cells with inflammatory background were reported. Considering nodular fasciitis and other benign or malignant tumorous lesions, surgical excision was planned because the mass did not regress, and histopathologic confirmation was necessary. (A) A 2.5 × 2.5-cm, nodular, hard, non-tender, pinkish mass is observed in the right preauricular area. (B) Neck magnetic resonance imaging reveals a same sized, well-demarcated, round, necrotic lesion in the right preauricular area with low signal on T1-weighted imaging and (C) high signal on T2-weighted imaging.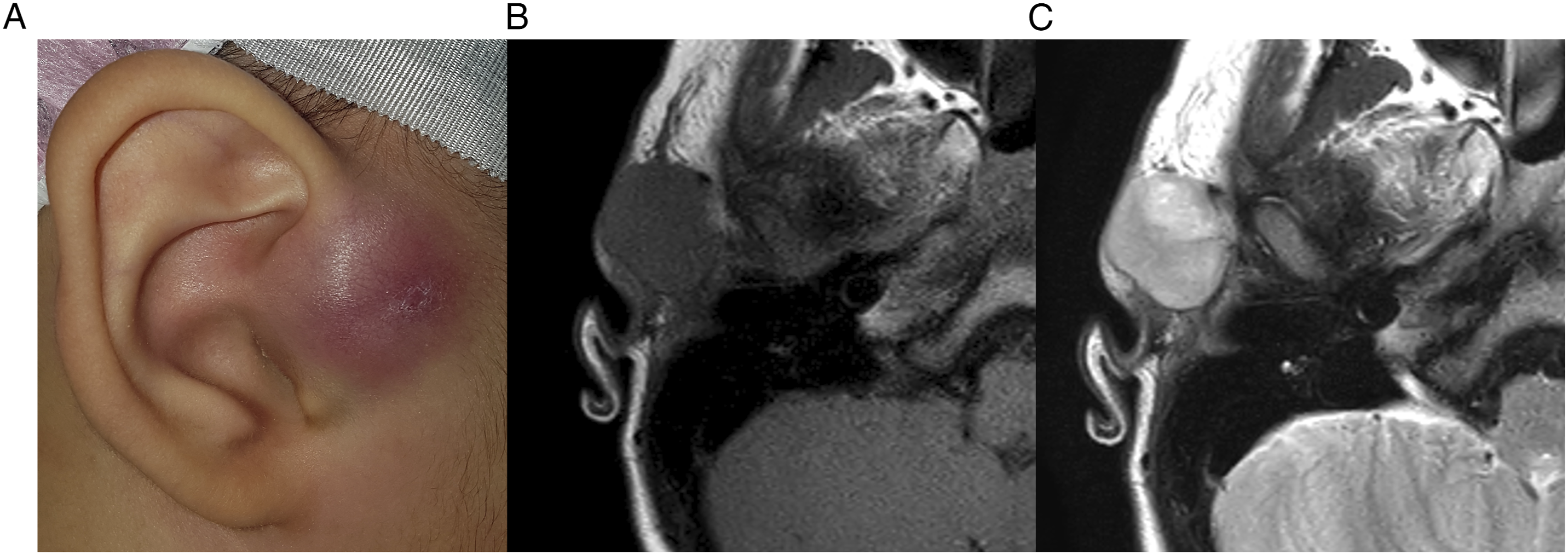
In surgery under general anesthesia, a skin flap was elevated, and a 2.5 × 2.5-cm, white mass was well defined from the surrounding tissue and completely removed. On histopathologic evaluation, hypercellular growth of fibroblasts and prominent mitotic activity with inflammatory cells were observed. Immunohistochemical stain showed positivity for SMA and negativity for CD34, S100, desmin, and beta-catenin. Thus, nodular fasciitis was diagnosed. At six months after surgery, the wound had healed well and there was no recurrence.
Discussion
Nodular fasciitis was first described by Konwaler et al in 1955 as subcutaneous pseudosarcomatous fibromatosis.1,9,11 It was renamed nodular fasciitis by Stout in 1961. 11 The etiology of nodular fasciitis is unclear.1,2,4,5,7,9,10,12,13 Although it was thought to be caused by trauma, most cases have no significant traumatic history. 13 Recently, nodular fasciitis has been reported to be associated with a myosin heavy chain 9 (MYH9)-ubiquitin-specific protease 6 (USP6) gene fusion, suggesting a clonal neoplastic origin.5-7,9 It has been reported to occur predominantly in males.7,11
Its prevalence in children is low, with only 10% of reported cases in pediatric patients. In pediatric patients, location of the lesion may be various, but it is most commonly reported in the head and neck. In a study with 15 pediatric patients with nodular fasciitis in the head and neck, the most common location was the maxillofacial region. 11 Nodular fasciitis appears as a solitary, tender, rapidly growing subcutaneous nodule rarely exceeding 2–3 cm in diameter. 1 It may show a red, pink, or mixed color. 4 Rapid growth of nodular fasciitis in the head and neck suggests malignancy, which often cannot be excluded by nonspecific imaging and pathology findings. 13 Nodular fasciitis may regress spontaneously for weeks to months. 14
The imaging findings of nodular fasciitis are variable and nonspecific.5,10,11 The mass may be centered within the subcutaneous tissue, more deeply located along deep fascia, or embedded in muscle. 11 It commonly shows moderate to marked enhancement on CT and MRI. 10 In MRI, a T1-weighted image shows low signal intensity, while a T2-weighted image shows high signal intensity.8,9 However, these findings in MRI are nonspecific. 8 In the head and neck, the lesion appears round or ovoid and mostly well defined. Linear extension of deeply seated lesions along the fascia, which is called “fascial tail sign,” suggests nodular fasciitis. 11 Lesions that grow along the fascia between the intermuscular septa form a “cloud sign” which only appears in nodular fasciitis. The “fascial tail sign” and “cloud sign” might be helpful to differentiate nodular fasciitis from other soft tissue lesions. 3
Histopathologically, nodular fasciitis shows proliferation of spindle cells in a myxoid stroma with capillaries and extravasated erythrocytes. 1 There may be abundant mitotic figures but atypia is not observed.1,5,10 Nodular fasciitis is classified into 3 subtypes of subcutaneous, intramuscular, and fascial, of which subcutaneous subtype is the most common.1,10 Nodular fasciitis can be distinguished from malignant lesions by lack of significant nuclear atypia, hypercellularity, cellular necrosis, or atypical mitotic activity on cellular staining. 6 On immunohistochemical staining, myofibroblasts are reactive to vimentin, actin, and CD68. Beta-catenin, S100, and cytokeratin AE1/AE3 can be used to rule out fibromatosis and neural and epithelial tumors. 5 Immunohistochemical staining is positive for SMA, vimentin, and occasionally focally for desmin and is negative for S-100, cytokeratin, and CD34. 1 Fine needle aspiration is rarely diagnostic but can reveal frequent mitoses, spindle cells, and low-grade atypia. 6
Treatment of choice is observation or complete resection.8,9,11 Conservative treatment such as observation is acceptable because many tumors regress spontaneously.1,13 Recurrence is rare,1,10-14 with low risk after excision of lesions in the trunk and extremities but increased risk for lesions on the face. 5
The differential diagnosis of nodular fasciitis includes other reactive lesions such as proliferative fasciitis and granulomatous disease; benign tumors such as fibrous histiocytoma, schwannoma, neurofibroma, dermatofibroma, inflammatory myofibroblastic tumor, and fibromatosis; and malignant tumors such as malignant peripheral nerve sheath tumor, dermatofibrosarcoma protuberans, and high grade sarcoma. 14 Nodular fasciitis is often misdiagnosed as a malignant tumor. 4
The present two cases of nodular fasciitis have clinical significance due to appearance in pediatric patients and location in the same region of the preauricular area. The masses grew rapidly, and malignancy could not be ruled out in preoperative evaluations. Definitive diagnosis was possible after surgical excision and pathologic analysis.
Nodular fasciitis in the preauricular area in a pediatric patient is rare. It could be confused with soft tissue sarcoma. However, nodular fasciitis should be suspected in a pediatric patient with a rapidly growing mass in the head and neck region. Surgical excision should be performed to confirm the histopathologic diagnosis when clinical diagnosis is uncertain and there is possibility of malignancy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Research Foundation of Korea grant funded by the Korean government (Ministry of Science and ICT; 2019R1F1A1062649).
Ethical Approval
The Institutional Review Board of the National Health Insurance Service Ilsan Hospital exempted the review of this study (NHIMC 2022-09-008).