
Abstract
Intramuscular hemangiomas (IMH) are benign vascular tumors of the skeletal muscles. These tumors are uncommon in the head and neck region and usually affect the trunk and extremities. IMH of the masseter and trapezius muscles have been reported in the head and neck region. However, the sternocleidomastoid is extremely rare. In the current case report, we described a 25-year-old man with a rare case of intramuscular hemangioma involving the sternocleidomastoid muscle and reviewed the relevant literature. Contrast-enhanced computed tomography was initially obtained and showed a slightly hyperdense soft tissue mass. Head and neck magnetic resonance imaging (MRI) demonstrate a well-delineated hyperintense lesion on the T2 sequence suggestive of a soft tissue hemangioma. Subsequently, angioembolization using onyx was performed, followed by surgical excision of the mass under general anesthesia. Histopathological examination of the mass showed vascular proliferation within the skeletal muscles, and fatty tissue with an abundance of capillaries, which are consistent with capillary type intramuscular hemangioma. The patient was followed up in the clinic until the wound healed. Three months after surgery, no recurrence was observed. Preoperative angioembolization contributed to the success of IMH surgery by reducing morbidity, facilitating complete excision, and decreasing the risk of recurrence.
Introduction
Hemangiomas are endothelium-derived neoplasms composed of vascular spaces that emerge from endothelial cells. During the first year of life, hemangiomas are frequently discovered in infants, and these lesions tend to achieve involution as they grow. 1 A unique type of hemangioma is known as intramuscular hemangioma (IMH). It is a benign vascular lesion found in the skeletal muscles of the trunk, upper and lower extremities, and to a lesser extent, in the head and neck region.2,3 Intramuscular hemangiomas account for less than 1% of all hemangiomas. 4 Only 15% percent of intramuscular hemangiomas occur in the head and neck regions. Masseter and trapezius muscles are frequently mentioned in the reports, while IMH of the mylohyoid and sternocleidomastoid (SCM) muscles are rare, along with other head and neck muscles.5,6 Intramuscular hemangiomas typically present as painless masses that develop slowly with distinct boundaries. 7 Radiological evaluations using magnetic resonance imaging (MRI) and computed tomography (CT) are critical for identifying IMH. 8 This case report described a rare case of sternocleidomastoid IMH managed with preoperative angioembolization followed by complete surgical excision. A review of the literature for similar cases of SCM IMH was also performed and discussed.
Case Report
We present a 25-year-old man with an insignificant medical and surgical history, who was referred from primary health care to our ENT head and neck clinic for the evaluation of a neck mass. He complained of a left neck mass that started 2 years prior and was stable in size. The complaint was not preceded by a history of infection or trauma. There were no other symptoms, and the patient denied pain, alterations in size, skin changes, night sweats, weight loss, loss of appetite, or fever. Examination revealed a triangular mass in the left posterior neck over the upper third of the sternocleidomastoid muscle area. The lesion measuring 3 cm × 4 cm, was firm and non-tender, with no skin changes. No enlarged cervical lymph nodes were palpated. The rest of the ENT examination, along with the cranial nerves and fiberoptic flexible nasopharyngeal scope, were unremarkable. Blood results were also unremarkable. Contrast-enhanced computed tomography showed a slightly hyperdense soft tissue mass in the upper one-third of the sternocleidomastoid muscle, deep into the skin (Figure 1A). Head and neck MRI demonstrates a well-delineated soft tissue lesion with query infiltration into the surrounding SCM. The lesion was isointense in the cervical muscles on the T1 sequence (Figure 1B) and hyperintense on the T2 sequence (Figure 1C). The post-gadolinium study showed a strong enhancement with some heterogeneity and persistence of signal voids of the intralesional vessels with the impression of soft tissue hemangioma (Figure 1D). The selected management option of surgery preceded by angioembolization was explained to the patient, and consent was obtained. Angiography revealed a well-defined left posterior paravertebral slow-flow cervical venous malformation supplied mainly by the left occipital artery. One day prior to surgery, embolization through angiography was performed using onyx, with an uneventful post-embolization course. The patient underwent surgery the next day with a horizontal neck incision following the skin lines over the mass. The mass was found immediately after the thinned subcutaneous tissue was dissected from the surrounding tissues. The lesion was hypervascularized with multiple perilesional vessels, infiltrating the surrounding SCM with a cut-off muscle that was removed along with the mass to ensure complete excision and decrease the chance of recurrence (Figure 2). The intraoperative bleeding was mild and reasonable. A medium-sized drain was inserted before closure and maintained under negative pressure. The patient recovered smoothly and was discharged on postoperative day (POD) one after drain removal. Histopathological examination of the mass showed vascular proliferation within the skeletal muscles and fatty tissues with an abundance of capillaries, consistent with capillary type intramuscular hemangioma (Figure 3). The patient was followed-up in the clinic. The wound healed without problems and there was no recurrence 3 months after surgery. Preoperative angioembolization contributed to surgical success by decreasing the operation time and blood loss, and facilitating dissection and excision of the mass to decrease the chances of recurrence.
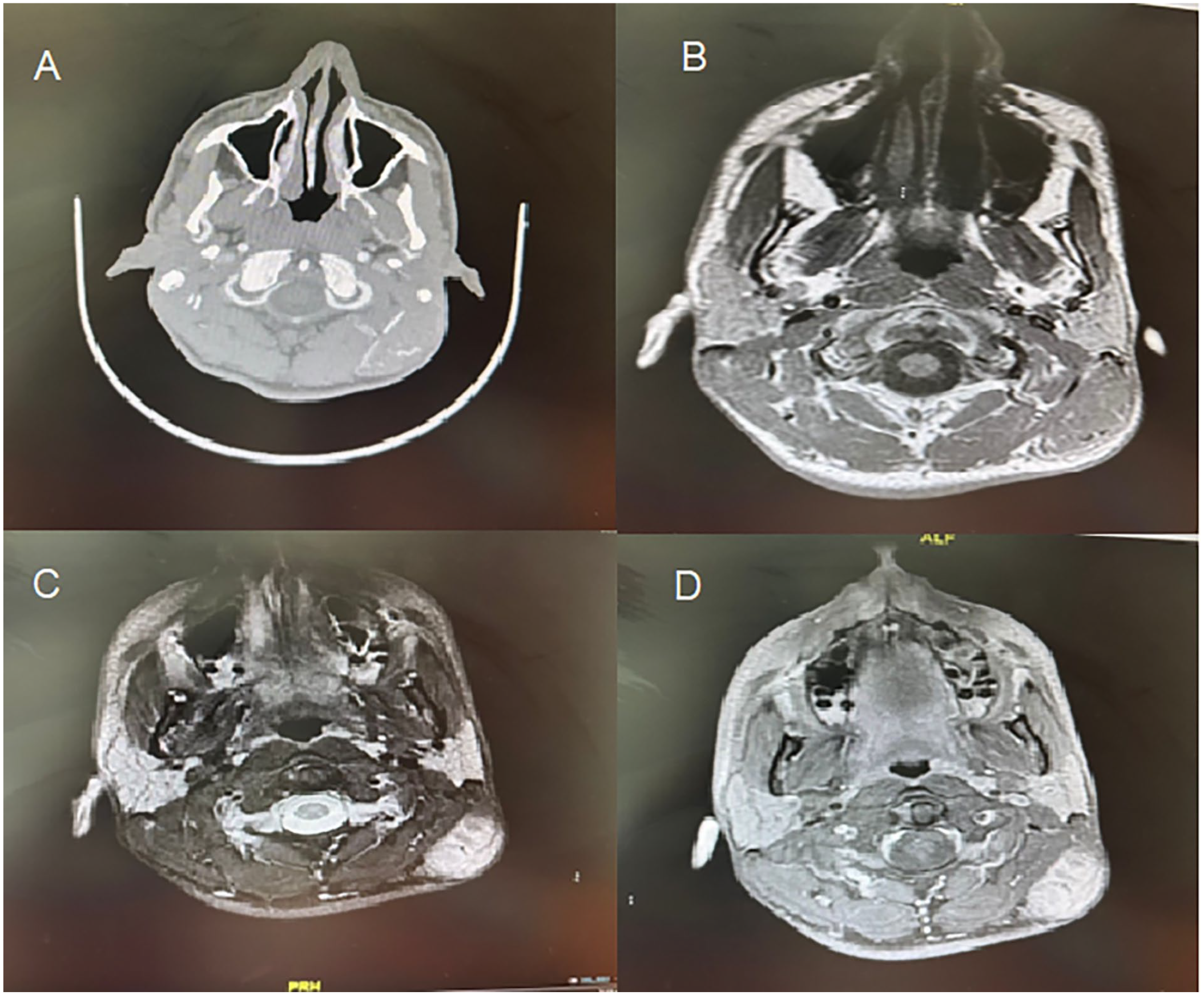
(A) Contrast-enhanced CT (axial cut) demonstrating slightly hyperdense soft tissue mass in the upper one-third of the left SCM. (B) MRI T1-weighted image (axial cut) demonstrating isointense mass in the left SCM. (C) MRI T2-weighted image (axial cut) demonstrating hyperintense mass in the left SCM. (D) Gadolinium-enhanced MRI (axial cut) demonstrating strong enhancement with some heterogeneity in the left SCM.

Intraoperative excised mass from the left sternocleidomastoid muscle measuring 3 x 4 centimeters.
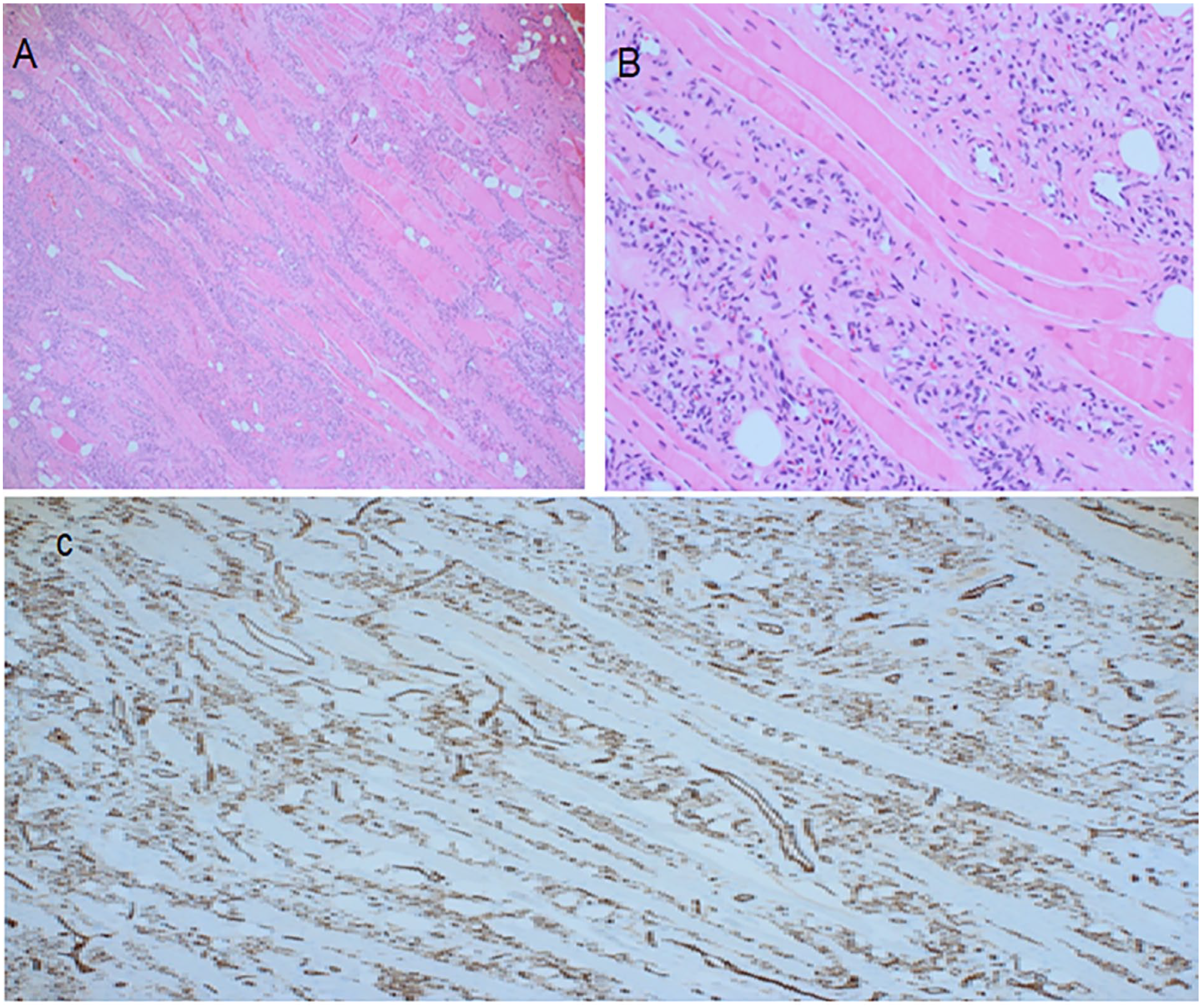
(A) A low power of H&E-stained section showing vascular proliferation between skeletal muscle fibers. (B) High magnification showing blood vessels proliferation between muscle fibers, some are containing red blood cells. (C) Immunohistochemical stain for CD31 antibody highlighting the endothelial cells of numerous blood vessels.
Discussion
Neck masses frequently present a diagnostic challenge with a wide variety of differential diagnoses including infection, inflammation, or neoplasia. In certain cases, when the diagnosis remains uncertain after radiological and pathological investigations, an excisional biopsy is required. Although certain lesions can be safely observed, others require further attention and investigation, particularly when the diagnosis is unclear or a neoplastic process is considered. 9 Intramuscular hemangioma (IMH) is a benign vascular tumor that accounts for less than 1% of all hemangiomas. It typically develops in the chest wall and lower extremities, while uncommon to be found in the head and neck region.10,11 IMH was first described by Liston in 1843 as a benign congenital tumor restricted to lower extremities muscles. 12 These tumors are more frequently diagnosed in adolescents and young adults, with no sex predilection. 10 Although the cause of IMH is not well understood, it is believed to be a congenital tumor that develops from embryonic remnants, same as congenital arteriovenous malformation.13,14 Pathologically, Hemangiomas are classified into 3 types: small vessel or capillary, large vessel or cavernous, and mixed. When a lesion encompasses a combination of different vessel types, it is known as a mixed-type hemangioma. 15 The most prevalent types of intramuscular haemangiomas in the head and neck region are capillary type hemangiomas, which encompass 68% of all cases, followed by cavernous and mixed hemangiomas, which constitute 19% and 5% of all IMH in the head and neck region, respectively. 15 In the literature, 12 case reports, including the present case of IMH involving the sternocleidomastoid (SCM) muscle, have been reported. Two of the 12 case reports lacked clinical information; thus, they were excluded. The average age of the 10 included cases was 40.8 ± 17.1 years (Table 1).6,9,16 -22 However, of the reported 10 cases of IMH in the SCM, 6 were cavernous type (Table 1).
All Published Case Reports of Intramuscular Hemangioma in the Sternocleidomastoid.
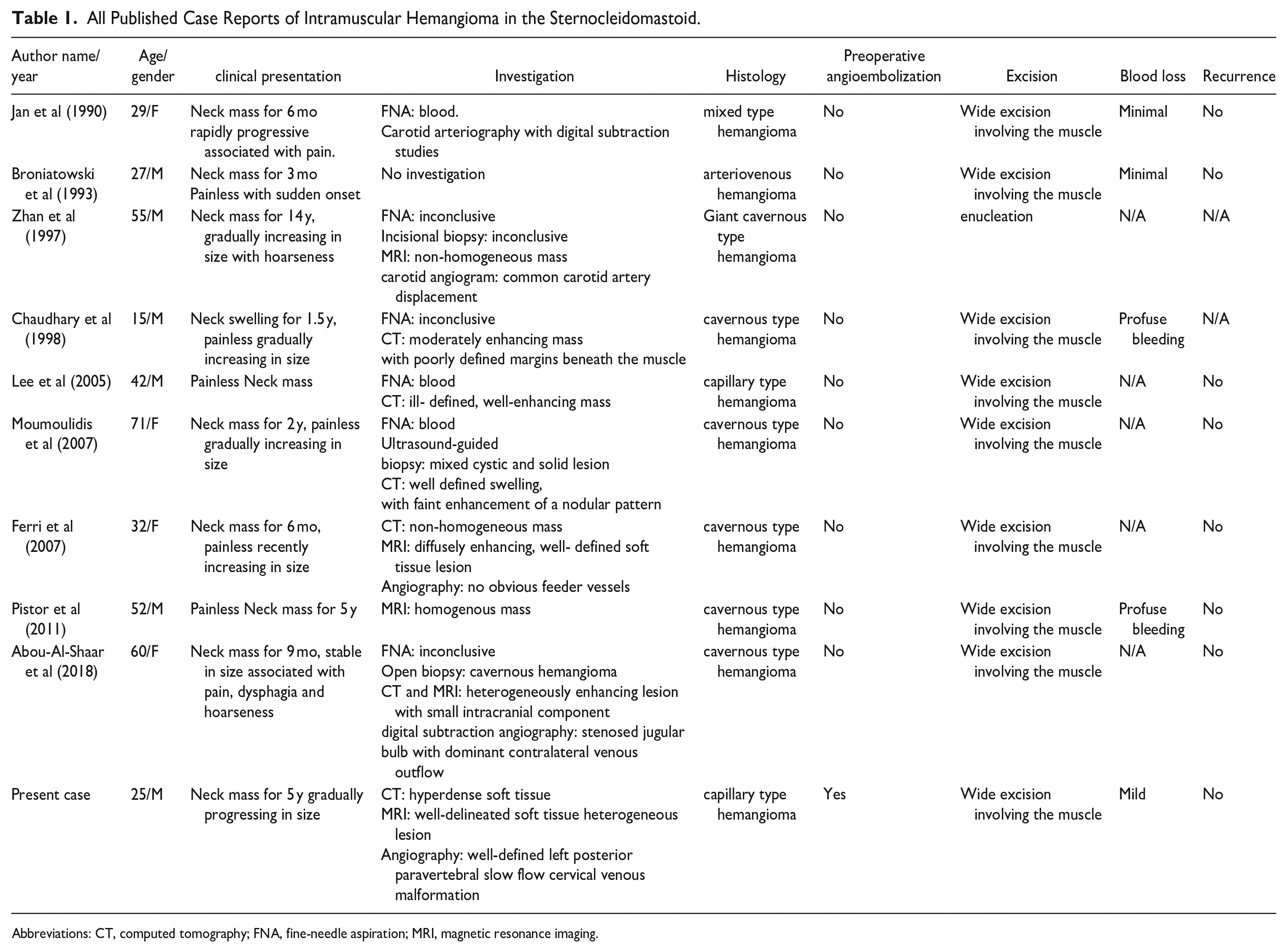
Abbreviations: CT, computed tomography; FNA, fine-needle aspiration; MRI, magnetic resonance imaging.
IMH usually presents as a well-defined, localized, soft, mobile, fluctuating mass. 16 Diagnosis of IMH requires thorough history taking and physical examination and is usually depicted by radiological investigations. MRI has been reported to be superior to CT for identifying intramuscular hemangiomas, defining their extent, and distinguishing between normal muscles and intramuscular hemangiomas. 11 IMH MRI typically demonstrates a hypointense signal on T1-weighted images and a hyperintense signal with well-defined borders that can be distinguished from nearby normal muscles on T2-weighted images. 17 In most cases, fine-needle aspiration (FNA) tends to reveal only blood and is non-diagnostic. 11 Complete surgical excision is considered the best treatment choice for IMH because it is the only treatment option that is able to definitively exclude malignant transformation. 11 The tumor infiltrative ability of IMH necessitates the removal of normal muscles considerably beyond the gross margins of the tumor to avoid local recurrence of the tumor. 11 Prior to surgical intervention, angiography or a vascular study is beneficial, as it can provide clear details about the nature of the tumor, the blood supply, and the need for preoperative embolization. 11 Although preoperative angioembolization is helpful for reducing intraoperative bleeding and the associated morbidity, none of the reported cases of SCM IMH used preoperative angioembolization before surgery.11,18,19 Conversely, several cases of IMH in the head and neck region have been reported using angioembolization preoperatively. Broniatowski described a case of capillary-type IMH involving masseter muscle managed with preoperative angioembolization to control bleeding. 20 Rossiter et al. described a case of IMH of the strap muscle of a capillary that was fed by the superior thyroid artery managed by angioembolization preoperative to reduce intraoperative hemorrhage with no subsequent recurrence. 11 Garefis et al. reported a case of scalene muscle IMH fed by the branches of the costocervical and thyrocervical trunks that underwent angioembolization preoperative to control blood loss. 21 Aloyouny et al presented a case of zygomaticus muscle capillary-type IMH and suggested that hemangiomas with no identifiable feeders could be managed with primary excision without preoperative embolization. 8 Additionally, Welsh et al and Rossiter et al. recommended that in cases of small muscle hemangioma or small-caliber feeding vessels, angioembolization is not indicated, and complete surgical excision is the best treatment.11,22
Conclusion
Complete surgical excision remains the treatment of choice for IMH. Preoperative angioembolization contributes to surgical success by reducing morbidity, facilitating complete excision, and decreasing the risk of recurrence.
Footnotes
Authors’ Note
The authors declare that this paper has not been presented at a meeting or conference.
Data availability Statement
Data available upon request at any time.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.