
Abstract
Objectives
Sinonasal squamous cell carcinomas are rare and aggressive tumors. Curative therapy includes surgery and radiotherapy, with high risk for local morbidity and impaired quality of life. The objective of this study was to analyze a large cohort of patients with sinonasal squamous cell carcinoma on treatment morbidity and oncological outcome.
Methods
Patients with sinonasal squamous cell carcinoma (n = 75) treated at a tertiary referral center between 2008 and 2019 were identified. In patients with curative treatment intent (n = 70), a chart review and analysis on patient and tumor characteristics, morbidity, and oncological outcome was performed.
Results
Mean follow-up was 59 months. Primary curative therapy was surgery alone (n = 18), surgery with radiation (n = 25), and primary (chemo)radiation (n = 27). Forty-two (60%) patients suffered from treatment-related morbidity; most frequent symptoms were dry nasal mucosa (20%), nasal obstruction (14.3%), and vision impairment or loss (11.5%). Patients with early disease had less morbidity (51.4 vs 71.1%; P = 0.09), a lower recurrence rate (27% vs. 48.5%; P = 0.08), and better overall survival (92.5% vs. 71.1%; P = 0.01).
Conclusion
Treatment-related morbidity is common after curative treatment of sinonasal squamous cell carcinomas. Early disease is beneficial in terms of occurrence and severity as multimodal treatment and recurrence can more likely be avoided.
Keywords
Introduction
Squamous cell carcinoma (SCC) is the most frequent malignancy in the nasal cavity and paranasal sinuses and a rare disease, characterized by its aggressive growth. Symptoms are usually unspecific and include impaired nasal breathing, ulceration, recurrent epistaxis or may even be absent in early stages, resulting in a locally advanced stage at diagnosis and consecutively impaired prognosis. 1 -4
For treatment in non-metastatic disease, surgery is the preferred and recommended modality providing good overall survival (OS). 4 -6 Complete tumor resection with negative surgical margins is essential and associated with better prognosis regarding survival. 7 -9 Over the last decade, endoscopic endonasal surgery in suitable patients has proven to be equal to an open approach, yielding lower complication rates and a shorter timespan to postoperative radiotherapy. 1,8,10,11 The efficiency of definitive and adjuvant radiation therapy has also been established. 12 -14 However, many patients require multimodal therapy, especially in case of locally advanced tumor stage or insufficient surgical margins. 5,6 Studies comparing treatment modalities found multimodal concepts to be favorable in terms of local control and OS. 4,15,16 In contrast, high T and N+ status at diagnosis are associated with worse long-term OS. 2,15 As the rarity of these tumors hinders prospective treatment studies, most analyses focus on survival rates and studies evaluating the morbidity in these patients are scarce. The aim of this study was therefore to analyze a large patient cohort with sinonasal SCC on treatment-related morbidity and oncological outcome.
Patients and Methods
Ethical considerations
All procedures were in accordance with the ethical standards of the national research committee and with the 1964 and 2002 Helsinki declaration. The institutional and regional review board (Inselspital, Bern University Hospital, Switzerland, reference number KEK-BE 002/2015) granted approval to conduct the study.
Patients and Data Acquisition
A retrospective chart review of all patients with histologically confirmed SCC located in the nasal cavity and paranasal sinuses was conducted. Patients discussed in the multidisciplinary tumor board of the Head and Neck Cancer Center, Inselspital, Bern University Hospital between 2008 and 2019 were included. Only patients with curative treatment intent and a follow-up period of at least three months were included in the analyses. Collected data contained patient characteristics, pre- and postoperative staging according to the Union for International Cancer Control (UICC) TNM Classification 7th edition (2010), treatment and follow-up. Morbidity was evaluated during the routine clinical assessments as reported by the patients without the use of a dedicated questionnaire.
Statistical Analysis
The follow‐up time was calculated starting by the date of the primary treatment and not censored at a predefined time point. Kaplan–Meier curves and log‐rank test were used to depict and compare the variables regarding time‐to‐event endpoints, respectively. Multivariate Cox's proportional hazards regression models with variables yielding P < 0.1 in univariate analyses were generated to evaluate possible prognostic factors for progression-free survival (PFS) and OS. Backward elimination was used to identify potential independent factors with a cut-off p < 0.05. Disease characteristics and morbidity of treatment groups were compared using the chi-squared test. Analyses were performed with JMP (version 14.0; SAS Institute GmbH, Heidelberg, Germany) and SPSS (version 23.0; IBM, Armonk, NY, USA).
Results
Patients and Primary Treatment
Clinicopathological Characteristics of the Study Population.
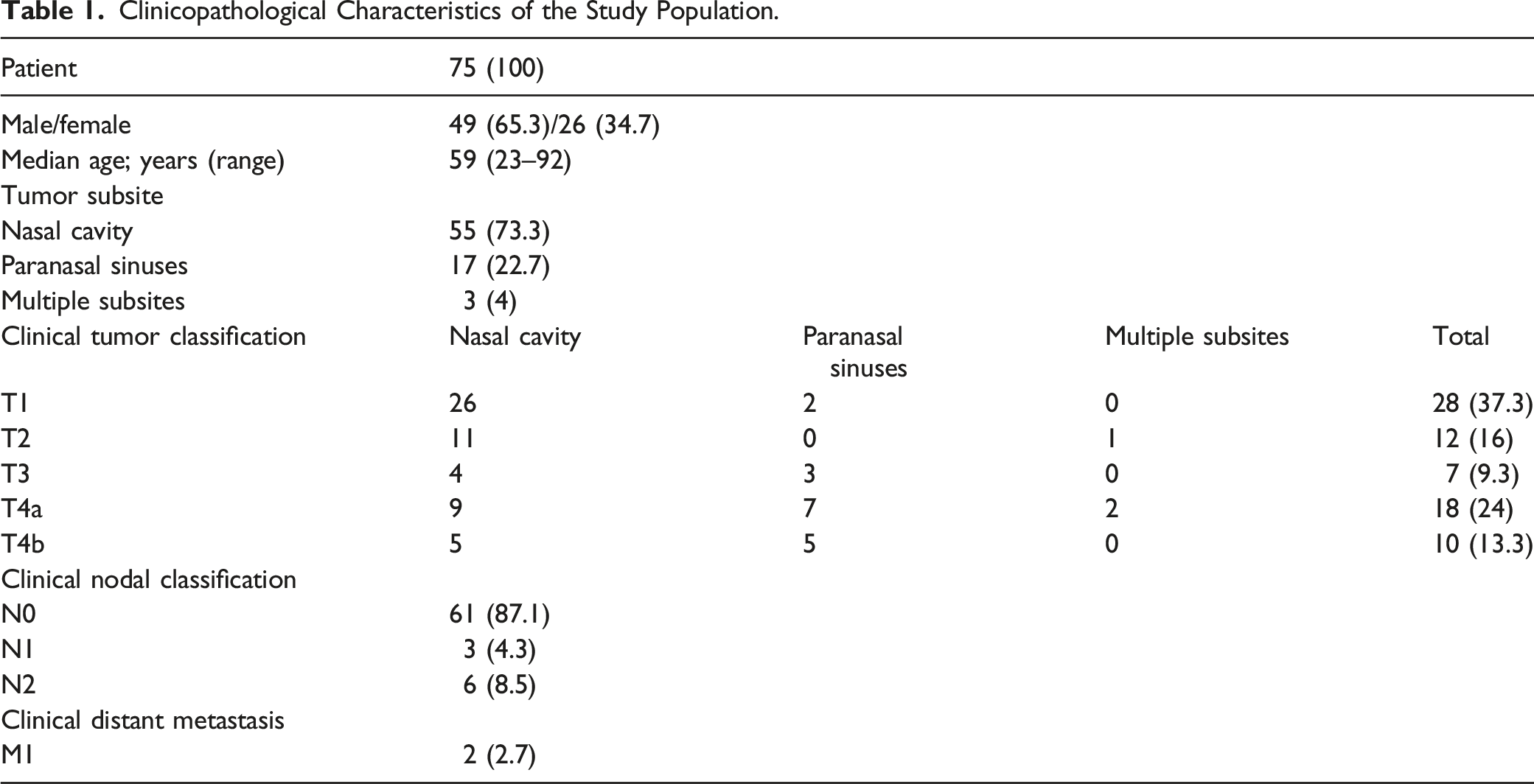
Thirty-eight patients were diagnosed with advanced disease (UICC stage III, IVA, or IVB), 55.3% (n = 21) of these tumors were located in the nasal cavity; 39.5% (n = 15) in the paranasal sinuses; and 5.3% (n = 2) in multiple subsites. Mean follow-up was 59 months (SD: 45.9; range 3–167, median 50.5).
Primary Treatment.
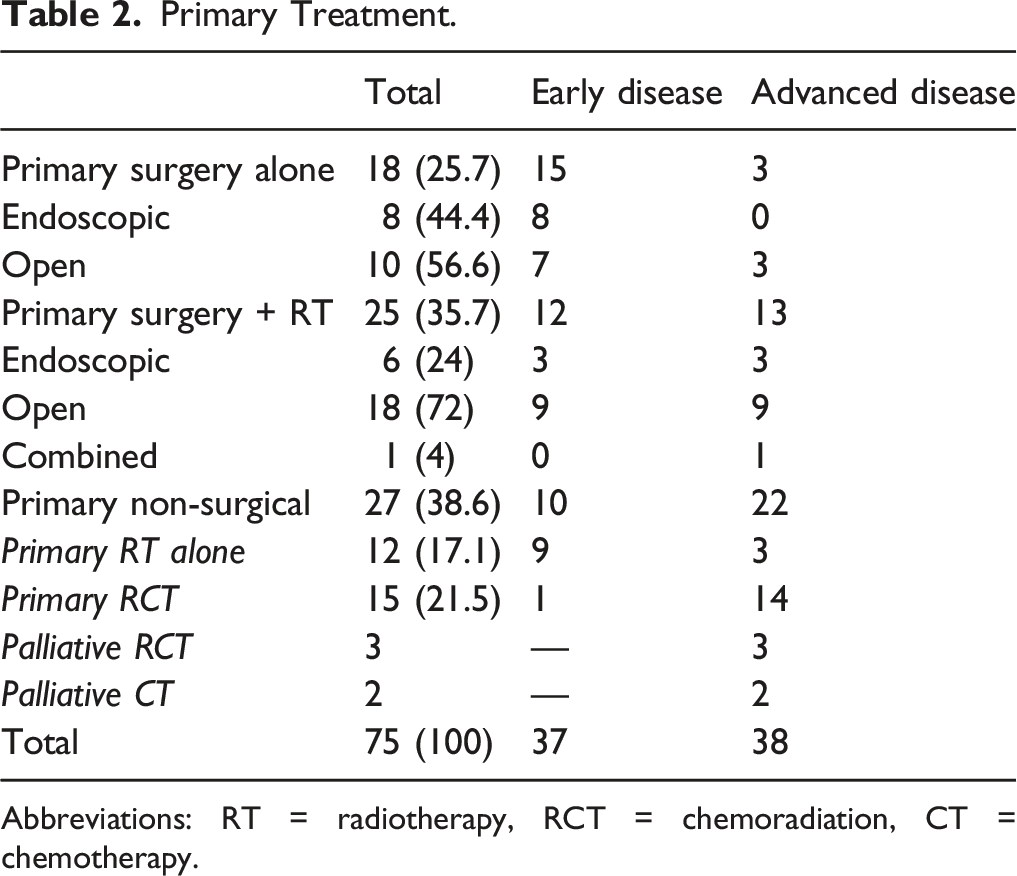
Abbreviations: RT = radiotherapy, RCT = chemoradiation, CT = chemotherapy.
Of the 43 patients with primary surgery, 14 (32.6%) were selected for an endoscopic and 28 (65.1%) for an open approach. One patient had a combined approach. Patients selected for an endoscopic surgery had mainly early disease (78.6%, n = 11/14). Patients with open surgery had early disease in 57.1% (n = 16/28) and advanced disease in 42.9% (n = 12/28).
Patients with endoscopic surgery had a lower rate of postoperative radiotherapy administration (42.9% vs. 64.3%; P = 0.208). The rate of R0 margin was similar in both groups (endoscopic: 28.6% vs. open: 35.7%; P = 0.8).
Treatment- And Disease-Related Morbidity After Curative Treatment
Frequency of Specific Morbidities at Last Clinical Follow-Up After Curative Treatment.
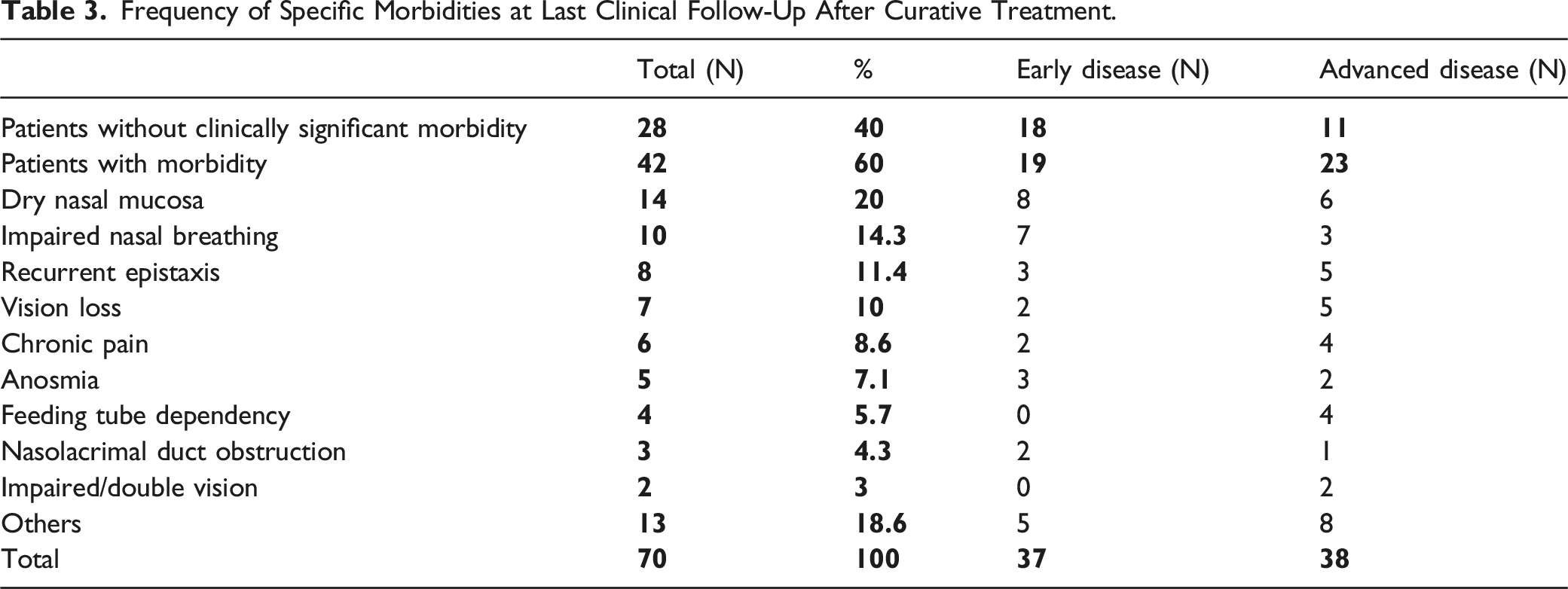
Morbidities listed as “others” include patients with other mild symptoms like rhinorrhea, halitosis, gastroesophageal reflux and dysphonia. Additionally, each one patient with previous radiotherapy developed an osteoradionecrosis of the maxilla, post-actinic pleural effusion, and laryngeal edema. One patient each developed tetraplegia and paraparesis in metastatic recurrent disease. Two patients died of local complications; one of a fatal bleeding out of the internal carotid artery and one of intracranial hypertension.
Patients with early disease had a lower rate of morbidity (19 of 37, 51.4%) compared to advanced disease (27 of 38, 71.1%) with no statistical difference (p = 0.09), as depicted in Figure 1. Especially severe morbidity like impaired or loss of vision, feeding tube dependency, and chronic pain occurred mainly or exclusively in patients with advanced disease (Table 3). Morbidity rates in early and advanced disease. (Early disease: Union for International Cancer Control stage I–II; advanced disease: stage III–IVb; RT = radiotherapy; RCT = chemoradiation; P = 0.09).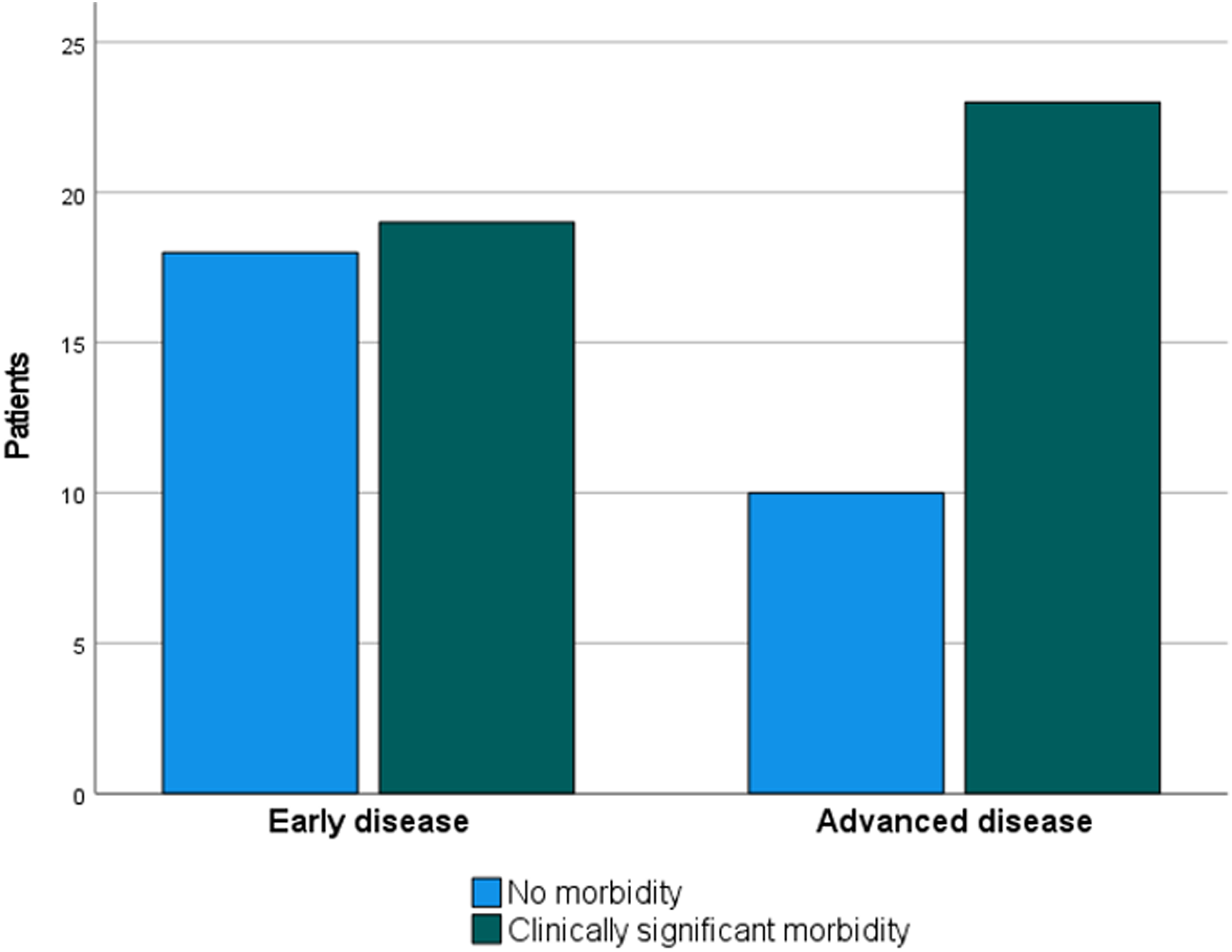
Recurrence, Salvage Treatment and Related Morbidity
Twenty-six of 70 curative patients (37.1%) had recurrent or persistent disease in the following pattern: local n = 11, loco-regional n = 4, regional n = 7, and distant n = 4. Patients in early disease had a lower recurrence rate (10 of 37, 27%) than in advanced disease (16 of 33, 48.5%; P = 0.08). The median time to tumor relapse was 6.5 months.
Salvage treatment included surgery only (n = 10), surgery + radiotherapy (n = 8), palliative chemotherapy (n = 7), and best supportive care (n = 1). Patients with recurrence had a higher rate of morbidity compared to patients without recurrence (19 of 26, 73.1% vs. 23 of 44, 52.3%; P = 0.07).
Oncologic Outcome
Overall survival was 82.3% after five years and 69.2% after ten years. Patients diagnosed at stage I–II showed significantly better long-term OS than stage III–IVB (five-year survival 92.5% vs. 71.1%; P = 0.01, Figure 2). Long-term overall survival of patients with stage I–II vs. III–IVB.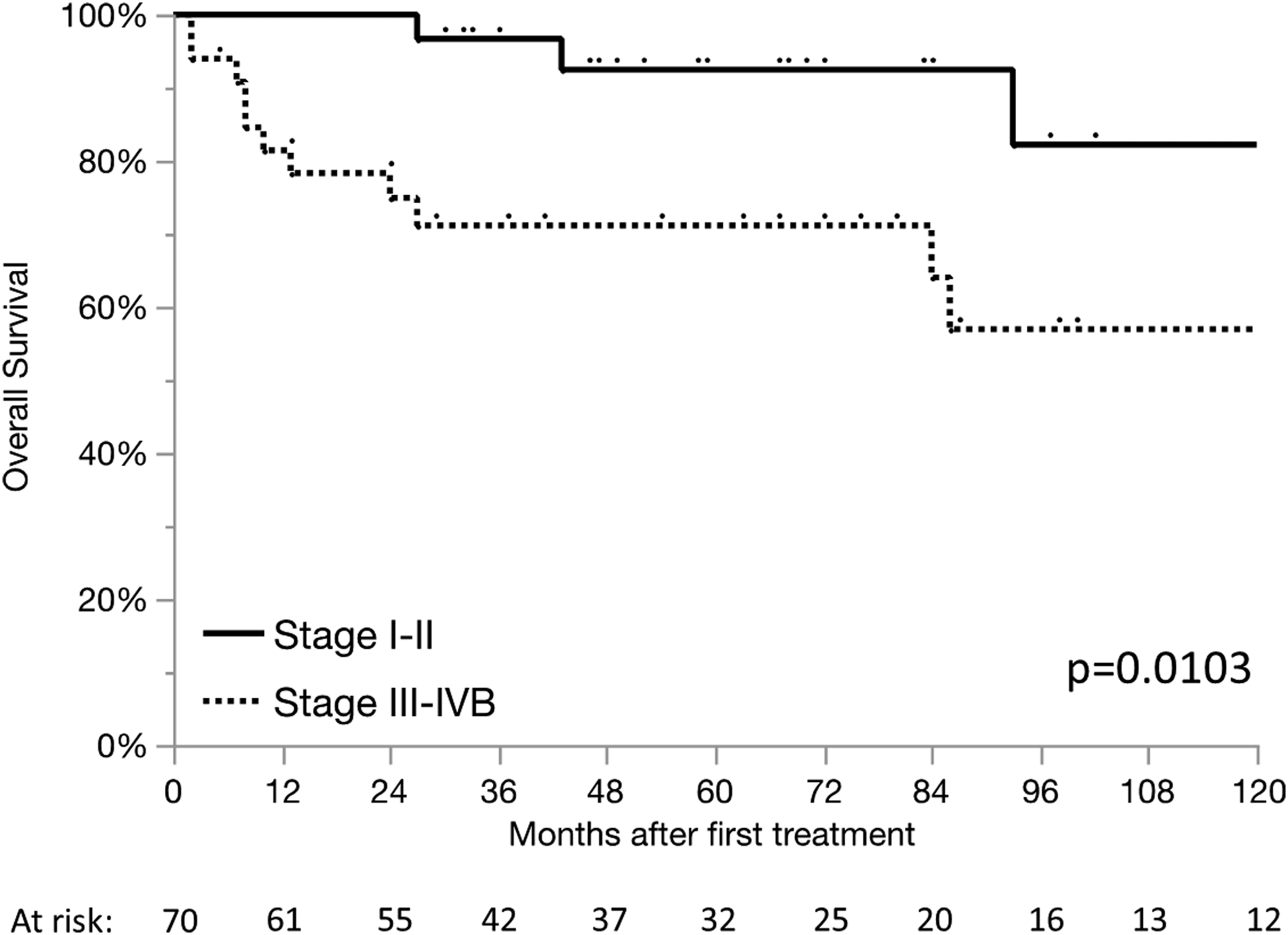
Uni- and Multivariate Analyses
Uni- and Multivariate Models for OS and PFS Before and After Backwards Elimination.
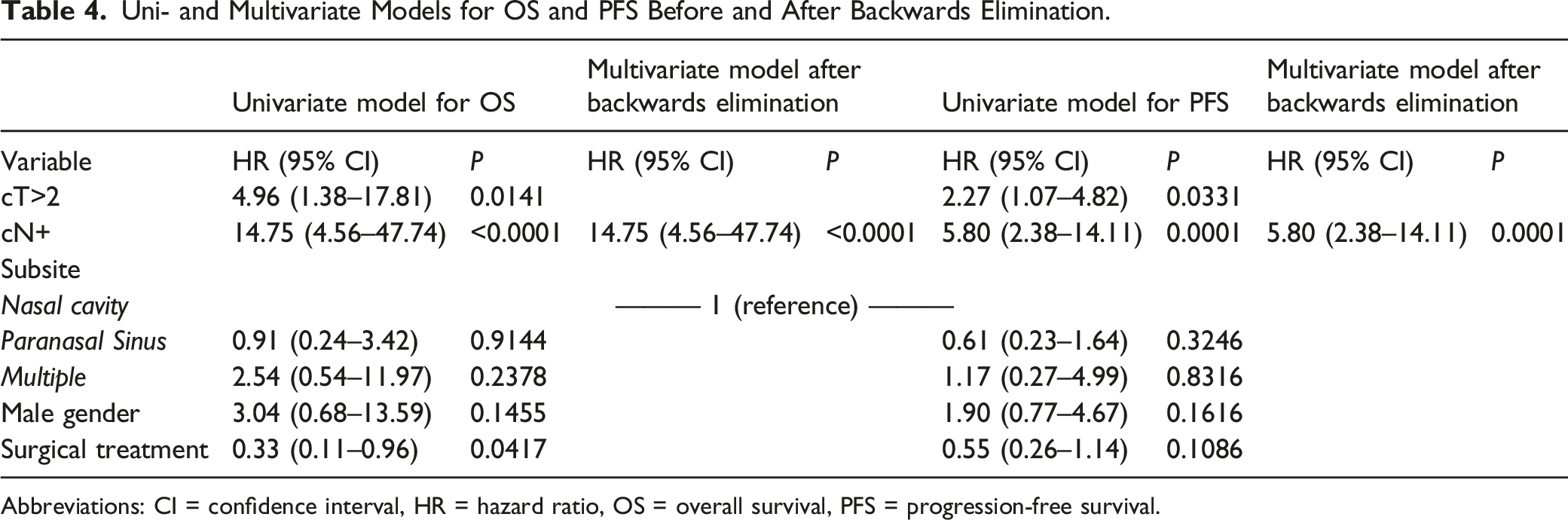
Abbreviations: CI = confidence interval, HR = hazard ratio, OS = overall survival, PFS = progression-free survival.
Discussion
Key Findings
This study includes 70 patients with sinonasal SCC, analyzed for treatment-related morbidity and long-term OS after curative treatment. Surgery ± adjuvant radiotherapy was selected as primary therapy in 61.4% of patients resulting in an OS of 82.3% after five and 69.2% after ten years. Univariate and multivariate analyses revealed cN+ status as an independent unfavorable predictor of OS and PFS. The majority of patients (60%) suffered from at least one treatment-related morbidity at the last clinical follow-up. Dry mucosa, impaired nasal breathing, and recurrent epistaxis were the most frequent mild symptoms while mainly patients in advanced disease suffered also from severe symptoms like vision impairment or loss (10%) and only single cases of severe or lethal treatment-related sequelae occurred.
Study cohort and treatment
Our study population is comparable to other large cohorts from single institutions, depending on selection of specific site and/or histology. 1,6,9,15,17 Analyses of larger patient cohorts were achieved recently with the United States’ national cancer database. 2,4,8 In this cohort, many patients were diagnosed at a locally advanced stage with no regional or distant metastases. Surgical resection was chosen as primary therapy in most cases, with 58.1% of additional adjuvant radiotherapy. Rationales for adjuvant therapy were positive surgical margins, advanced T stages or the presence of other histopathologic risk factors. In literature, surgery is the mainstay for primary therapy and multimodal therapy (including surgery) has been demonstrated as favorable for local control and OS. 2,15 Induction chemotherapy followed by surgery has been shown a viable option as well. 2,4
Morbidity
Sinonasal malignancies are located next to the skull base and may infiltrate critical structures like the orbit, cranial nerves, and blood vessels. Local tumor invasion and the importance of a resection with safe margins implicate an increased risk of treatment-related perioperative complications and morbidity. In this cohort, most patients suffered from local morbidity after curative therapy; most frequent were dry mucosa (20%), impaired nasal breathing (14.3%), or recurrent epistaxis (11.4%). A substantial number of patients also suffered from vision impairment or vision loss (11.5%), chronic pain (8.6%), or anosmia (7.1%). Few other studies report treatment morbidity and evidence is scarce. In a series of 109 patients with sinonasal malignancies since 1964, Mendenhall et al. (2009) reported severe complications in 30% of cases after radiotherapy and 26% in patients after surgery and adjuvant radiotherapy. 15 In radiotherapy, the advances from conventional to intensity-modulated radiotherapy (IMRT) technique reduced late toxicities significantly. 12,18,19 Subsequent to IMRT, Askoxylakis et al. (2016) reported dysgeusia or dysosmia (34.4%), ocular toxicity (34%), nasolacrimal duct obstruction (18%), and xerostomia (13.1%) as the most common late adverse events. 12
Decreased post-therapeutic quality of life has been demonstrated as poor prognostic factor for OS in head and neck cancer patients. 20 Minimizing treatment morbidity is an important aspect to be considered upon interdisciplinary discussion at the tumor board. Nevertheless, studies including health-related quality of life questionnaires in sinonasal cancer are rare. In a recent study, Philips et al. (2020) found an elevated level of anxiety and depression in patients with higher T status two years after treatment. 21 Patel et al. (2020) assessed treatment-related morbidity in a cohort of 129 patients with sinonasal malignancies of all histological subtypes and a follow-up of 42 months. In their cohort, 36% of patients required subsequent surgery for nasal obstruction or chronic sinusitis and a significantly higher incidence of complications after radiotherapy. While reduced perioperative complication rates for endoscopic surgery have been highlighted, 1,8,22 the comparison of subsequent morbidity is challenging due to the selection bias and the high number of patients receiving radiotherapy as adjuvant or salvage treatment.
Oncological Outcome
OS of the study cohort was 82.3% after 5 and 69.2% after ten years. Uni- and multivariate analyses highlight the negative impact of locally advanced tumors and lymph node infiltration on OS and PFS. In other studies, sinonasal SCC show a 5-year OS of 50–57%. 1,2,23 Local recurrence is a serious concern; Zocchi et al. (2020) reported an overall recurrence rate of 24% after ten years with a median time to recurrence of 14 months. 3
Limitations
For the evaluation of morbidity and its specific implications for the patient, a prospective assessment with a validated questionnaire would be the preferable methodology, for example, with the European Organization for Research and Treatment of Cancer quality of life questionnaire with its head and neck module. 24 To assess perioperative surgical complications, the Clavien–Dindo classification is the best choice. In this study, we focused on morbidity in the clinical follow-ups. Nevertheless, some morbidities may have been missed due to the loss of follow-up.
A systematic clinical and patient-reported evaluation of morbidity before and after treatment during the regular follow-ups seems to be the best approach to examine the association of morbidity and different therapeutic options.
As location, staging and patient preference all affect the choice of treatment modalities and the choice of surgical technique, a selection bias cannot be excluded. Further, tumors with advanced or complex infiltration patterns usually undergo radiotherapy when considered unresectable or when excessive morbidity after surgery is expected. Moreover, we acknowledge that retrospective design and cohort size limit the evidence that can be obtained by the analysis.
Clinical Applicability of the Study
We present a large single-institutional, in many cases long-term followed cohort of patients with sinonasal SCC and their treatment morbidity and oncologic outcome. Because these tumors are rare and often locally advanced at diagnosis, treatment-related morbidity is common but poorly investigated. We demonstrate that mild symptoms like dry mucosa, nasal obstruction, and epistaxis are common but also vision impairment or loss are sporadic adverse events in locally advanced tumors. Small tumors without neck infiltration have excellent long-term oncological prognosis and single modality treatment may spare such patients later treatment morbidity. Systematic evaluation of morbidity and quality of life assessments before treatment and during follow-ups appears the best approach to examine the effect of different modalities, although a selection bias cannot be eliminated.
Conclusion
Treatment of sinonasal SCC comprises a high rate of patients with local morbidity. Tumors with limited local and no regional extent have a good long-term prognosis. Early diagnosis with single-modality treatment reduces the risk for treatment-related morbidity. For further investigation of treatment morbidity and its effect on the patient quality of life, the use of dedicated questionnaires is preferable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.