
Abstract
Endoscopic sinus surgery presents significant visuospatial challenges to surgical trainees. The convoluted maze-like nature of the paranasal sinuses makes sinus surgery particularly challenging to master. The challenges are compounded by a visual disconnect as surgeons are moving their hands in a three-dimensional (3D) space while viewing at a two-dimensional screen. To date, residents practice endoscopic techniques in cadavers and in the operating room, which are limited by cost and patient safety, respectively. Given these challenges and constraints, surgical simulation is an attractive method of training for endoscopic sinus surgery.
Both low- and high-fidelity simulators have been widely used in the education of healthcare workers and their value has been strongly established.
1
Simulators that present the user with complex and immersive scenarios by providing realistic conditions are considered high-fidelity. In contrast, task trainers with limited functions that meet only selected requirements for practicing procedural skills are considered low-fidelity.
2
In recent years, several high-fidelity simulators, including cadaveric models, have been validated, but their cost and availability limit their use.
3
-6
Low-cost models and task trainers reproducing anatomy with silicone and other materials were developed and validated as a cost-conscious alternative.
3,7
-9
A high-fidelity 3D printed simulator has been described and validated by Alwani et al with good results,
10
but no standalone low-cost, low-fidelity, 3D printed sinus surgery simulator has been described in the literature to date. The objective of this study was to test the utility of a set of novel standalone low-fidelity, low-cost, 3D printed models of the nasal cavity to simulate sinus surgery (Figure 1). 3D Computer aided designs and still images from the 4 sinus surgery simulator stations depicting the associated tasks. (Station 1) cutting, (Station 2) grasping, (Station 3) angled cannulation, and (Station 4) advanced cutting.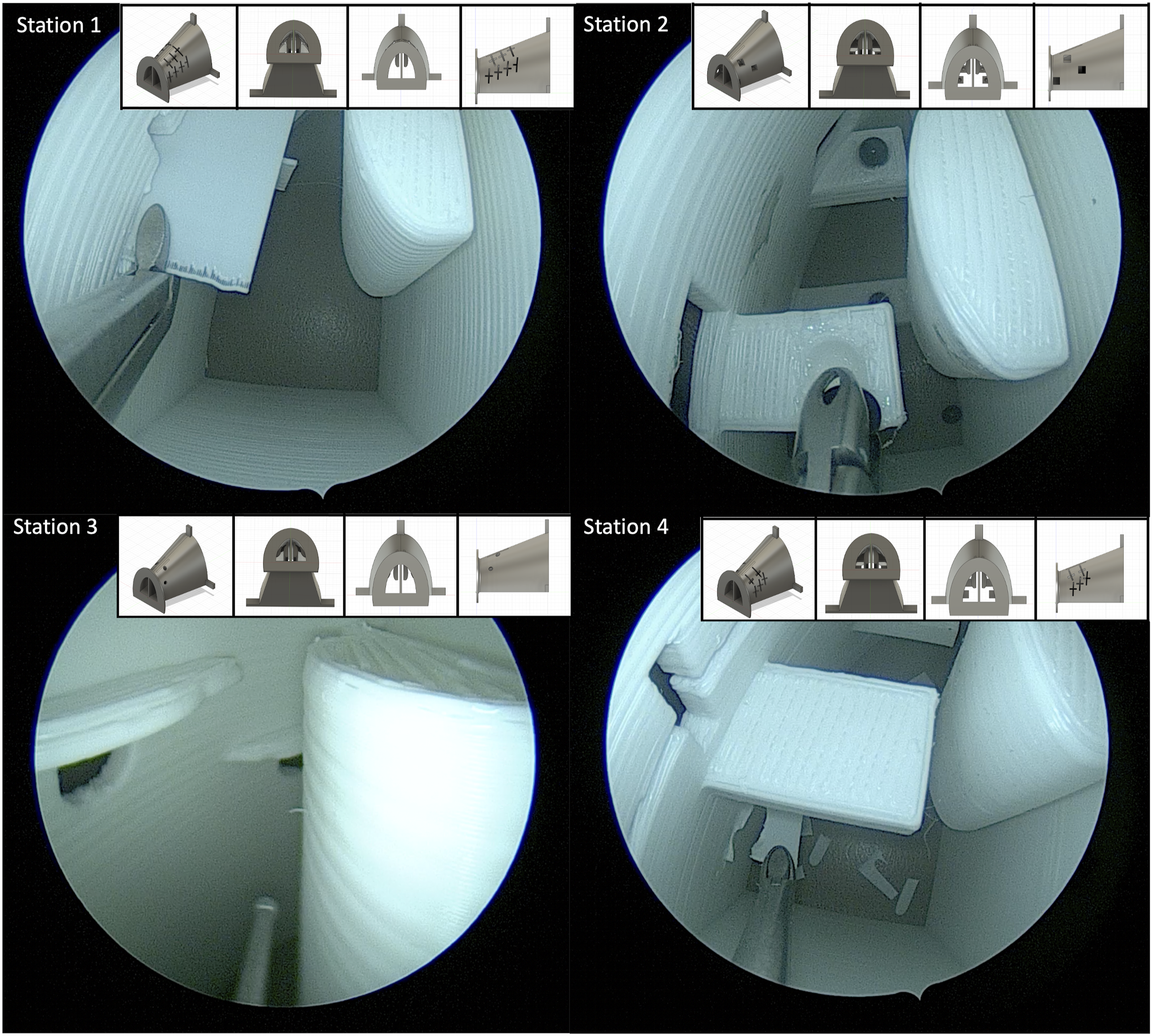
We performed a quality improvement study of 10 otorhinolaryngology residents (PGY1 - 5). All participants completed a self-assessment survey of 10 questions on their perceived sinus surgical skills using a 10 cm visual analog scale (VAS). The participants then rotated through 4 stations, each with different training modules developed by the authors (Figure 1). The stations were as follows: Station 1—cut 3D printed inserts that are loaded into the model in both horizontal and vertical orientations from the base to clear the nasal cavity from all “disease.” Station 2—use Blakesley forceps to grasp beads from ledges within the nasal cavity. Station 3—use angled instruments to cannulate openings hidden behind overhangs. Station 4—a more challenging version of Station 1 with inserts hidden behind overhangs, requiring angled endoscopy and instrumentation. After the training sessions, the participants repeated the same self-assessment survey.
All residents rated their post-intervention “overall sinus surgery skills” higher than pre-intervention. They rated simulations to provide more significant utility as an adjunct to surgical education after the intervention. All but one participant reported improved spatial awareness working with the endoscopes and surgical instruments. There was subjectively improved proficiency in using 0-degree and angled endoscopes as well as cutting, grasping, and curved instruments after the intervention. The simulations led to subjective improvements in spatial awareness, bimanual dexterity, and increased confidence in selecting correct surgical instruments. All but one senior resident reported utility for simulators in their education, stating that “their skills are past what the simulation provides.” This is reflected in the data when the analysis was stratified by level of training. Junior residents were far more likely to perceive improvement in their endoscopic skills with use of the simulator when compared to their senior counterparts (Figure 2). Graphic representation of (A) overall mean VAS results of the Self-Assessment Survey before and after simulation. Linear graphs were then stratified by resident training level: (B) junior and (C) senior. Error bars represent standard error of the mean. VAS (Visual Analog Scale). SAS (Self-Assessment Survey). Q (question).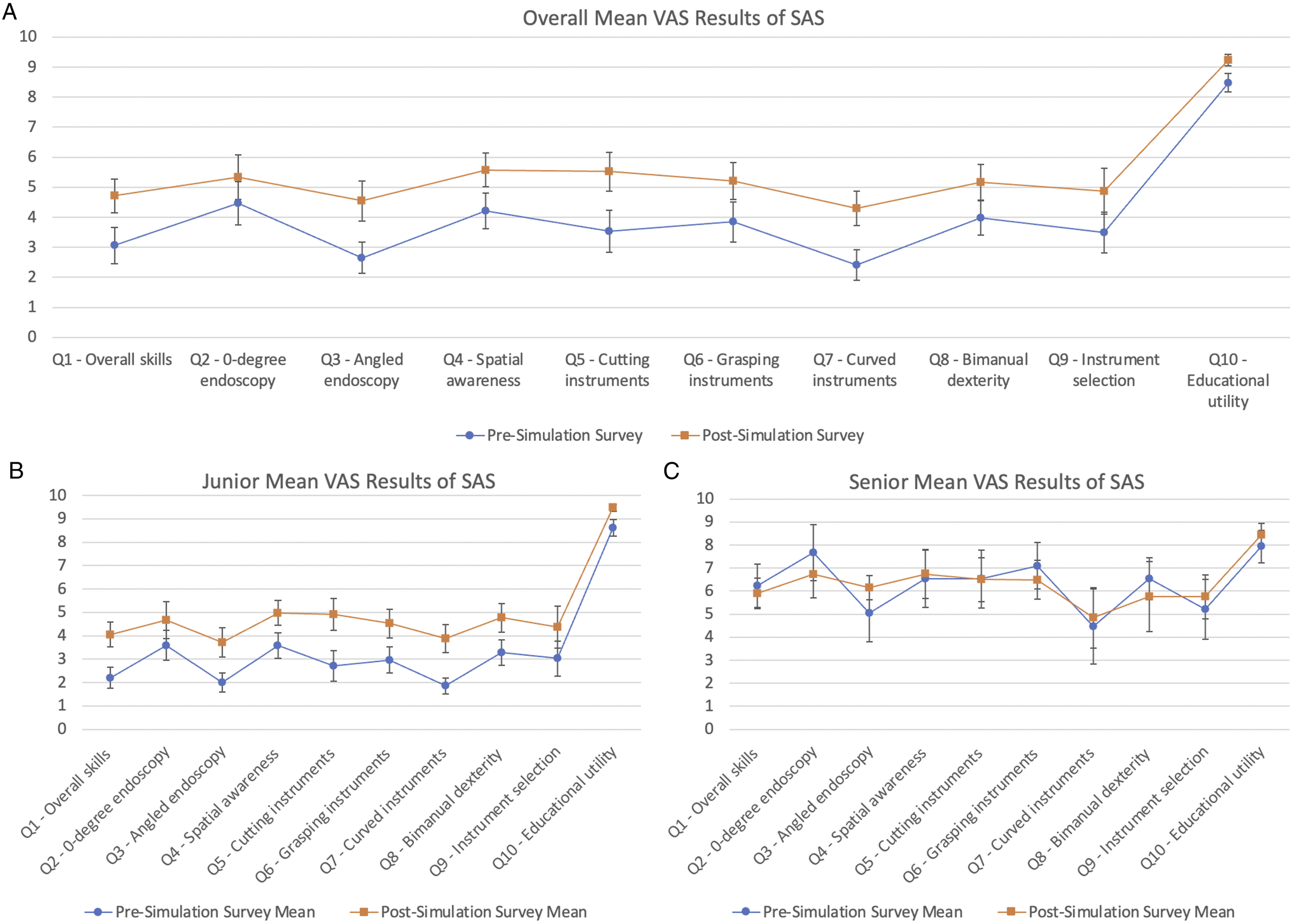
The main aim of any surgical simulation program is to accelerate the learning curve before a junior trainee begins performing in a real clinical scenario. Other low-cost task trainers to accomplish this have been described in the literature, and our current model incorporates similar tasks while possessing the ability to re-use and easily replace the product. One senior resident noted that compared to cadaveric dissections, the current 3D printed model was better to learn endoscopic dexterity and get accustomed to instruments by enabling repeat actions due to replaceable parts.
Our set of novel 3D printed models of the nasal cavity and paranasal sinuses to simulate sinus surgery tasks was well accepted by the resident cohort as a tool to improve basic endoscopic sinus surgery skills. Although residents of any level can benefit from refining their basic endoscopic skills set, this simulation model in its current version is best suited for junior residents to start learning basics of endoscopic technique to later translate into the operating room. The 3D models can serve as a low-cost, reusable tool to adjunct traditional residency education.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: WCY serves as a consultant for Aerin Medical and on the speaker’s bureau for Optinose Inc. AUL serves as a consultant for Lyra Therapeutics (Watertown, MA, USA), Medtronic (Dublin, IE), (Sanofi (Paris, France), and Stryker (Kalamazoo, MI, USA). AUL serves on the scientific advisory board for ENTvantage Dx (Austin, TX, USA) and Third Wave Therapeutics (San Francisco, CA, USA). AUL has served on advisory boards for AstraZeneca (Cambridge, UK) and Glaxo-SmithKline (Brentford, UK).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Approval was obtained by the quality improvement research committee. Verbal consent was obtained from all participants in this study.
Data Availability
All data associated with this study is reported in the manuscript. There is no additional supplemental material to report.