
Abstract
The Solitary Fibrous Tumor (SFT) is a rare mesenchymal neoplasm that arises mainly from the pleura. The sinonasal tract is generally not affected by SFT, and less than 100 cases have been reported in the English literature to date. We report an extremely rare SFT of the nasal cavity and paranasal sinuses extending into the anterior frontal fossa through the floor of the anterior skull base. To our knowledge, this case is the fourth SFT of the sinonasal tract involving the anterior frontal fossa in the world. Meanwhile, the tumor, measuring 13 × 6 cm in images, is the largest SFT of the sinonasal tract compared to previously reported cases. Three surgical procedures, including a transcranial one, were performed for the patient to achieve complete removal of the tumor. The diagnosis of SFT was established primarily by immunohistochemical positivity for CD34, STAT6, and negativity for S-100 protein. We emphasize the possibility of recurrence in SFT, and close follow-up is necessary with the help of nasal endoscopy and imaging approaches.
Introduction
The Solitary Fibrous Tumor (SFT) is a rare neoplasm that is histopathologically generally thought to be a benign spindle cell neoplasm of mesenchymal origin, first described in the pleura by Klemperer and Rabin in 1931. 1 Although most SFTs typically arise in the pleura, several of these tumors have been reported in a wide variety of extrapleural sites such as the abdomen, extremities, head and neck region, liver, and urogenital tract. SFTs of the sinonasal tract are extremely rare, and to date, less than 100 cases have been reported in the English literature. We have recently admitted a rare case of extrapleural SFT of the nasal cavity and paranasal sinuses, which is of special significance because the tumor extends into the right frontal area. Persistent clinical manifestations were observed even though the third resection had been performed on the patient. Previous literature has not described such a case, most of them presenting postoperatively uneventful SFTs that scarcely affected the anterior frontal fossa. Meanwhile, to the best of our knowledge, it is the fourth SFT of the nasal cavity and paranasal sinuses involving the anterior frontal fossa and the largest SFT of the sinonasal tract (measuring 13 × 6 cm) reported so far in the world. Therefore, we present the rare case in this paper, combined with a review of the comprehensive sinonasal SFT of 67 cases with available information,2–47 adding additional experience to the management of SFT for similar situations.
Case report
A 47-year-old man was admitted to the ENT department. The patient presented with a 3-month history of progressive intermittent epistaxis, to which, however, he did not pay attention. He also complained of watery rhinorrhea for a month, with no headache, nasal obstruction, nasal discharge, hyposmia, decreased visual acuity, ear symptoms, or history of trauma. Nasal endoscopy revealed a large mass was filling bilateral nasal cavities. Computed tomography (CT) demonstrated a large mass in bilateral nasal cavities, occupying bilateral ethmoid sinuses, extending into bilateral anterior frontal fossa through the floor of the anterior skull base with predominance on the right side. A magnetic resonance imaging (MRI) scan showed a cystic tumor originating from bilateral nasal cavities measuring 13 × 6 cm, which involved bilateral ethmoid sinuses, bilateral anterior frontal fossa, and the left frontal lobe (Figure 1 A–E). The esthesioneuroblastoma for the preliminary diagnosis was taken into account by postoperative histopathology after surgical excision of the endoscopy. Further histopathological analysis demonstrated an unencapsulated tumor in the submucosa with patternless spindled to ovoid cells in a variably collagenous stroma (Figure 1 F). In immunohistochemistry, CD34, CD56, and CD99, while negative for PCK, SMA, and S-100 protein, were positive in tumor cells (Figure 1 G). Subsequently, the intracranial lesion of the patient was resected via a transcranial approach, followed by reconstruction of the skull base. Two postoperative histopathological examinations finally confirmed the diagnosis of SFT with positivity for CD34 and STAT6. Coronal (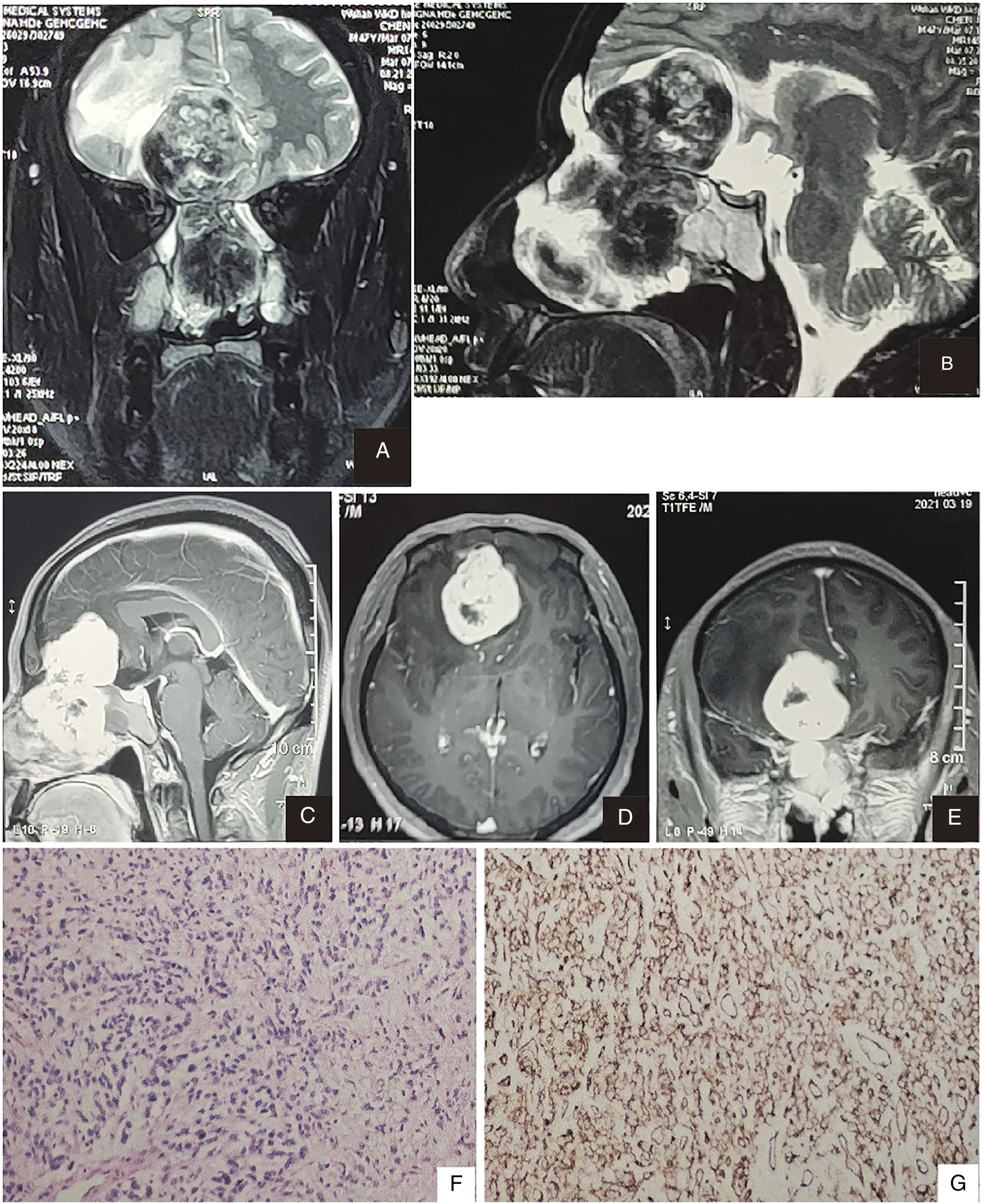
Three months after surgery, the patient, complaining of the same symptoms mentioned above, came to the ENT of our institution for further treatment. Electronic nasopharyngoscopy showed a large expansile tumor with a rough surface that occupied the upper part of the bilateral nasal common meatus. Local polyps and a deviated nasal septum were observed, while no masses of the nasopharynx were disclosed. A CT scan revealed a hyperdense mass (measuring 48 × 38 mm) with calcification and a poorly defined margin in the nasopharyngeal cavity. The tumor involved the frontal bone and the frontal lobe and destroyed the bony structures of the ethmoid sinus and nasal septum. Subsequently, the contrast MRI scan showed that the tumor invaded the area from the nasal septum to the bilateral ethmoid sinuses and the right frontal area. The tumor showed marked heterogenous contrast enhancement in the T1–weighted contrast-enhanced images, a hypointense signal on the T1-weighted images (T1WI) and the T2-weighted images (T2WI). The signals of obstructed secretions in the bilateral maxillary sinuses, ethmoid sinuses, and frontal sinuses were homogenous hyperintense in T2WI.
After tracheal intubation under general anesthesia, a nasal endoscopy approach was performed for tumor resection. The huge polypoid mass was identified, filling the nasal cavity with extension into the intracranial frontal area, and partial bone destruction of the skull base was observed. The mucinous secretions in the paranasal sinuses were eliminated without evidence of tumor invasion except for the sphenoid sinuses. The tumor was removed entirely, The specimen consisted of grayish-brown and unencapsulated tumor tissue measuring 5.0 × 3.5 × 2.0 cm in greatest size. On microscopy, the tumor showed moderate and cytologically homogenous proliferation of spindle cells with interstitial collagen deposits; no necrosis was observed. Spindle tumor cells were positive for CD34, CD99, Bcl-2, and STAT6 and negative for SOX-10 and Desmin. The proliferation index, Ki-67, was approximately 5%. All cells exhibited negativity for S-100 protein. On account of the above-mentioned results, the diagnosis of SFT without malignancy was determined.
Two months later, reexamination demonstrated chronic nasosinusitis and enlargement of the cervical lymph nodes compared to the previous. The patient also reported a weight loss of 3 kg although no local recurrences or metastases were observed. The patient rejected a recommended radiation treatment plan for unclear personal reasons. The patient was followed up by subsequent follow-up.
Discussion
SFT is usually described as a rare indolent neoplasm by published literature, almost all of them stating the hypothesis that SFT grows from mesenchymal rather than mesothelial tissue.2,48,49 SFT can occur at any anatomic site of the body, commonly the pleura and peritoneum. It originates in the head and neck region with a percentage of approximately 5–27%. 45 However, the tumor rarely affects the nasal cavity and paranasal sinuses, from which, more exceptionally rarely, it arises extending into the anterior frontal fossa. To our knowledge, there are seven cases of sinonasal tract SFTs that cause erosion of the anterior skull base so far; only three cases have been described to infiltrate the anterior frontal fossa.5,15,30
Summary of sinonasal tract SFTs: epidemiological and clinical characteristics.
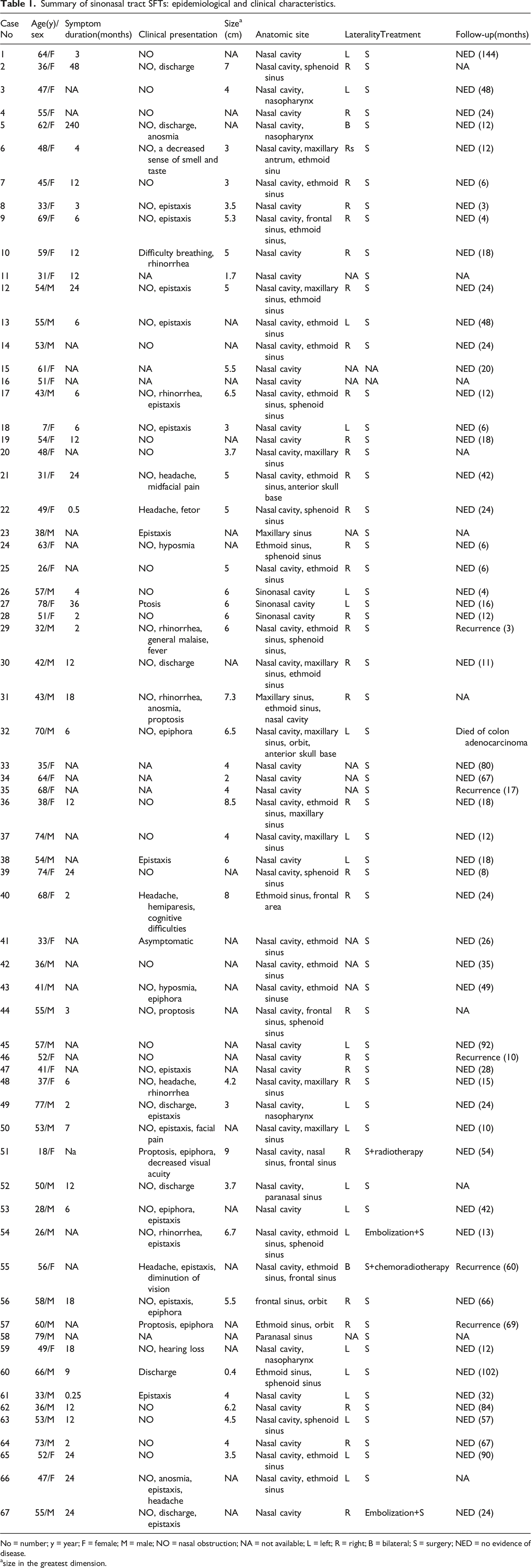
No = number; y = year; F = female; M = male; NO = nasal obstruction; NA = not available; L = left; R = right; B = bilateral; S = surgery; NED = no evidence of disease.
size in the greatest dimension.
The patients comprised 30 males and 37 females with an average age of 51 years (range 18–79 years). SFT generally occurring in adults can manifest at any age without a specific peak of age prevalence and significant sex difference considering all anatomic sites.43,45 Most patients clinically complained of nasal obstruction, commonly unilateral, epistaxis, and nasal discharge. Other symptoms such as rhinorrhea, hyposmia, epiphora, proptosis, and headache were often seen. The duration of symptoms ranged from 0.25 to 240 months, with an average of 17 months. Tumors ranged in size from 0.4 to 9.0 cm in the largest dimension with a mean size of 4.9 cm.
These clinical presentations are usually not enough to diagnose sinonasal tract SFTs. The clinical differential diagnosis should be considered, including hemangiopericytomas, nasopharyngeal angiofibroma, and nasopharyngeal carcinomas. 15 The pathologist should obtain the specific macroscopic, microscopic, and immunohistochemical characteristics of SFTs to make the correct diagnosis. Macroscopically, SFTs are described as white, pinkish, reddish, circular or oval, well-circumscribed, pedicled or sessile, unencapsulated, firm fibrous masses with gray to tan fibrous cut surfaces.4,15,42,47 Microscopically, SFTs are composed of plump spindle cells dispersed in a patternless pattern. In general, the alternation of hyper- and hypo-cellular areas within the collagenous stroma is observed. It is prominent that the vascular network consists of thick-walled branching vessels, and necrosis is absent.5,15,46
The morphological characteristics have been well described, but the diagnosis of SFTs cannot leave out the account of immunohistochemistry. Consistently, immunohistochemical analysis shows that SFT tumor cells stain positively for CD34, CD99, STAT6, Bcl-2, and vimentin and negatively for cytokeratin, desmin, epithelial membrane antigen, smooth muscle actin, and S-100 protein. In particular, STAT6 has recently become a reliable marker for the diagnosis of SFT. The nuclear expression of STAT6 is regarded as a reflection of the presence of fusion of the NAB2-STAT6 that results from a paracentric inversion on chromosome 12q13 and characterizes SFTs.45,50 Furthermore, strong and diffuse nuclear expression of STAT6 aids in the diagnosis of SFT with a sensitivity greater than 95%.51,52
Imaging evaluation before preoperative planning is vital and helpful for the diagnosis of SFT. For SFT of the nasal cavity and paranasal sinuses, a CT scan is the best choice of imaging modality for diagnosis, and MRI should be taken in the second. The CT scan provides a precise presentation of tumor extension and bone resorption, while the MRI scan can provide a more detailed view of tumor invasion in cases with orbit or endocranial extension. On CT, the tumor presents as a well-delineated isodense mass, usually having heterogenous contrast enhancement. Internal calcifications can sometimes be observed. However, these imaging features of CT scans are nonspecific for SFT. 53 MRI often shows a hypointense or isointense on T1WI and hypo- or hypertense on T2WI mass, with heterogenous contrast enhancement after gadolinium infusion administration. The predominant hyperintense in T2WI with strong gadolinium enhancement suggests SFT, which is unusual for other nasal lesions.43,54 Furthermore, marked enhancement in both CT and MR images is a typical feature of SFT attributed to its high vascularity.
According to the previously reported literature with available information, surgical resection, called the gold standard of treatment, has been performed in all cases, sporadically associated with adjuvant preoperative embolization or postoperative radiotherapy.37,40,41,46 Complete resection of the tumor with clear surgical margins is optimal. However, margins are often difficult to assess because the tumor in this anatomic region is frequently resected via an endoscopic surgical approach, a mini-invasive procedure with piecemeal resection; 47 and the surgeon must determine whether adequate resection has been achieved. Two or more procedures, even open or extranasal, may be used due to vital structures near the tumor of the sinonasal tract and the anterior frontal fossa. The patient here underwent three procedures, including a transcranial approach to achieve complete removal of the tumor. The tendency to excessive bleeding of the tumor should be closely monitored, and preoperative embolization may decrease bleeding.8,40 There is no therapeutic consensus for radiotherapy as an alternative treatment modality to be proved in more cases, and it can be an option for patients associated with positive surgical margins or recurrence.
Of the 67 cases summarized with available data, 51 patients presented no evidence of disease and ranged in follow-up duration from 3 to 144 months with an average of 33.2 months. A patient died from postoperative complications of colon adenocarcinoma five weeks after SFT resection, 24 and local recurrences were observed in 5 patients 3–69 months after resection.21,25,33,41,43 All cases documented no metastasis. It is hard to predict the prognosis of SFT in the nasal cavity and the paranasal sinus region since a low number of cases have been reported so far. The authors emphasized that malignant pathology does not indicate malignant clinical behavior and that recurrence and metastases were documented in several cases lacking atypical histological characteristics.24,45 Virtually, complete surgical resection, described as an important prognostic factor, can provide excellent outcomes for patients whose tumors do not contain malignant components.21,43 On the other hand, clinically close postoperative follow-up, utilizing nasal endoscopy and imaging approaches such as CT and MRI, is necessary because there are some SFTs of the nasal cavity and paranasal sinuses associated with recurrences, although in most cases present benign clinical behavior.
Conclusion
In this article, we present an extremely rare case of SFT located in the nasal cavity and paranasal sinuses, and it is the fourth SFT derived from this anatomic site with extension into the anterior frontal fossa through the floor of the anterior skull base reported in the English literature. In particular, it is the largest SFT of the sinonasal tract among the literature published to date. Three successive surgical resections were performed due to residual tumor following the primary surgery attributed to the large volume of the mass and vital neighboring structures. The diagnosis of sinonasal SFT requires a combined examination of nasal endoscopy, biopsy, immunohistochemistry, and imaging procedures. Complete surgical resection with negative margins is the golden standard of treatment. Although most SFTs appear to be indolent neoplasms, close follow-up should be performed due to the occasional emergence of recurrences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by the National Natural Science Foundation [No. 82073349]