
Abstract
Solitary fibrous tumors are well-recognized in the pleura and their occurrence in the nasal cavity is uncommon. They show a hemangiopericytoma-like vasculature, a “patternless pattern” of growth, and lesions characterized by both hypercellularity and hypocellularity. As a malignant form of SFT, mesenchymal neoplasm is extremely uncommon and poorly understood, although there are no established standards for making this diagnosis, it is nonetheless accepted. It can develop either de novo or within an already-existing benign SFT, and there are few published accounts of the cytopathologic characteristics of these tumors.
In this case, a patient complained of tenderness on the right nasal root and diplopia for six months. Here, we report on a case of malignant solitary fibrous tumors in the nasal cavity, which extended into the orbit, and review the radiologic and pathologic features.
Introduction
The solitary fibrous tumor (SFT) is seldom seen and was originally described as a “pleural tumor.”1,2 Most SFTs were likely regarded as hemangiopericytomas (HPCs) and are characterized by a branching, HPC-like staghorn vasculature.1,2 The cell which SFT originates from has not been definitively identified. Although SFTs are usually benign and slow-growing tumors, malignant SFTs have been most often described in the pleura and it is now recognized that these tumors may arise at any site. 2
The differential diagnosis between benign and malignant SFT uses data regarding the characteristics of cell lineages. The list of differential diagnoses becomes even more daunting when one includes site-specific tumors such as mesothelioma or sarcomatoid carcinoma in pleural tumors and “true” hemangiopericytomas of the sinonasal tract. It is probable that the most difficult differential diagnosis would be to distinguish between malignant SFT and benign SFT, and the criteria for malignancy are not standardized. Recently, malignant SFT is described by the World Health Organization Classification of Soft Tissue Tumors as “having features including hypercellularity, at least focal moderate to marked cellular atypia, tumor necrosis, four mitoses/10 high-power fields, and infiltrative margins.”3,4 These tumors occur in the extrapleural sites such as the peritoneum, mediastinum, and lungs. SFTs of the paranasal sinuses, though extremely rare, do occur. Previous studies have shown that SFTs of the pleura generally demonstrate a strong CD34 immunoreactivity, but separate tumors of the paranasal sinuses have not been analyzed.5,6 We treated a case of SFTs of the paranasal sinus and orbit.
Case report
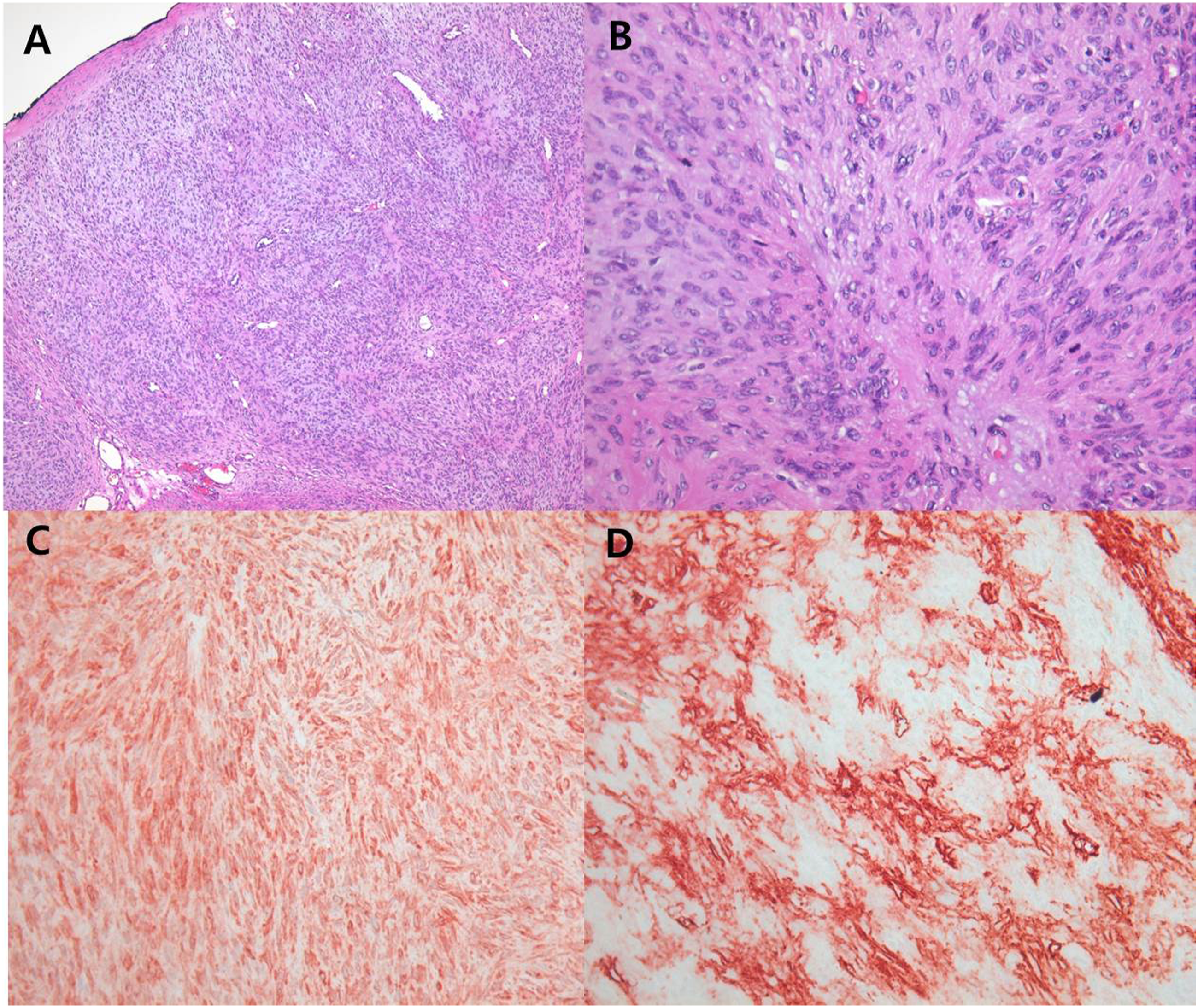
A 60-year-old female patient had a six-month history of diplopia with periorbital swelling. Computerized tomography (Figure 1(A) and (B)) and magnetic resonance imaging (Figure 1(C) and (D)) of the paranasal sinus and orbit were performed and the imaging studies revealed that a nasal mass filled the right anterior ethmoid sinus, 2.5x3.3 cm in size, and extended into the right maxillary sinus. The mass extended into the right medial orbital wall and the orbit with bony destruction. The right medial rectus muscle was found to be invaded and other external orbital muscles were displaced. The right cribriform plate showed a bony erosion but was not invaded intracranially (Figure 1(B) and (D)). The radiologic images were strongly suspicious for malignancy in the nasal cavity. An intranasal endoscopic biopsy was performed three times, but only revealed evidence of a benign mesenchymal tumor and there was insufficient evidence of malignancy. Therefore, we decided to remove the mass using the lateral rhinotomy approach for the purpose of confirming or ruling out malignancy. Examination of the frozen section strongly suggested that the mass was malignant. The tumor was removed completely from the patient with ethmoidectomy using an extended lateral rhinotomy approach. Postoperative pathologic findings showed cell changes that were suggestive of malignancy. This lesion exhibited moderate hypercellularity, severe atypia, and mitosis (6/10HPF) but no necrosis. (Figure 2(A) and (B)). Immunohistochemical studies of paraffin-embedded tissue sections of the excised tumor showed staining of the tumor cells for CD34, b-catenin, BCL-2, and SMA (Figure 2(C) and (D)), but no staining for the S-100 protein. A diffuse weak positive staining was observed for P53 and Ki67(5%). The patient had radiation therapy, 60 cGy, postoperatively. Radiological images after surgery and radiation therapy showed no definitive evidence of a recurrence of the mass. However, mild enhancement of the right periorbital soft tissue layer was observed, probably due to post radiation changes. Following surgery, the patient did well, and three years later, there are no signs of disease. CT scan at the level of the orbit and ethmoid sinus (A, B) and MR images, T1-weighted (C) and T2-weighted (D). The nasal mass filled the right anterior ethmoid sinus and extended to the right medial orbital wall and orbit with bony destruction. The right medial rectus muscle was found to be invaded and the right cribriform plate showed a bony erosion, but not invaded intracranially. Non infiltrative border, but increased cellularity on low power field, X100 HE (A), increased mitosis and atypia on high power field, X400 HE (B), immunostaining for Bcl-2 showing strong positivity in spindle cells. X400 Bcl-2 (C), immunostaining for CD34 showing strong positivity in spindle cells, X400 CD34 (D).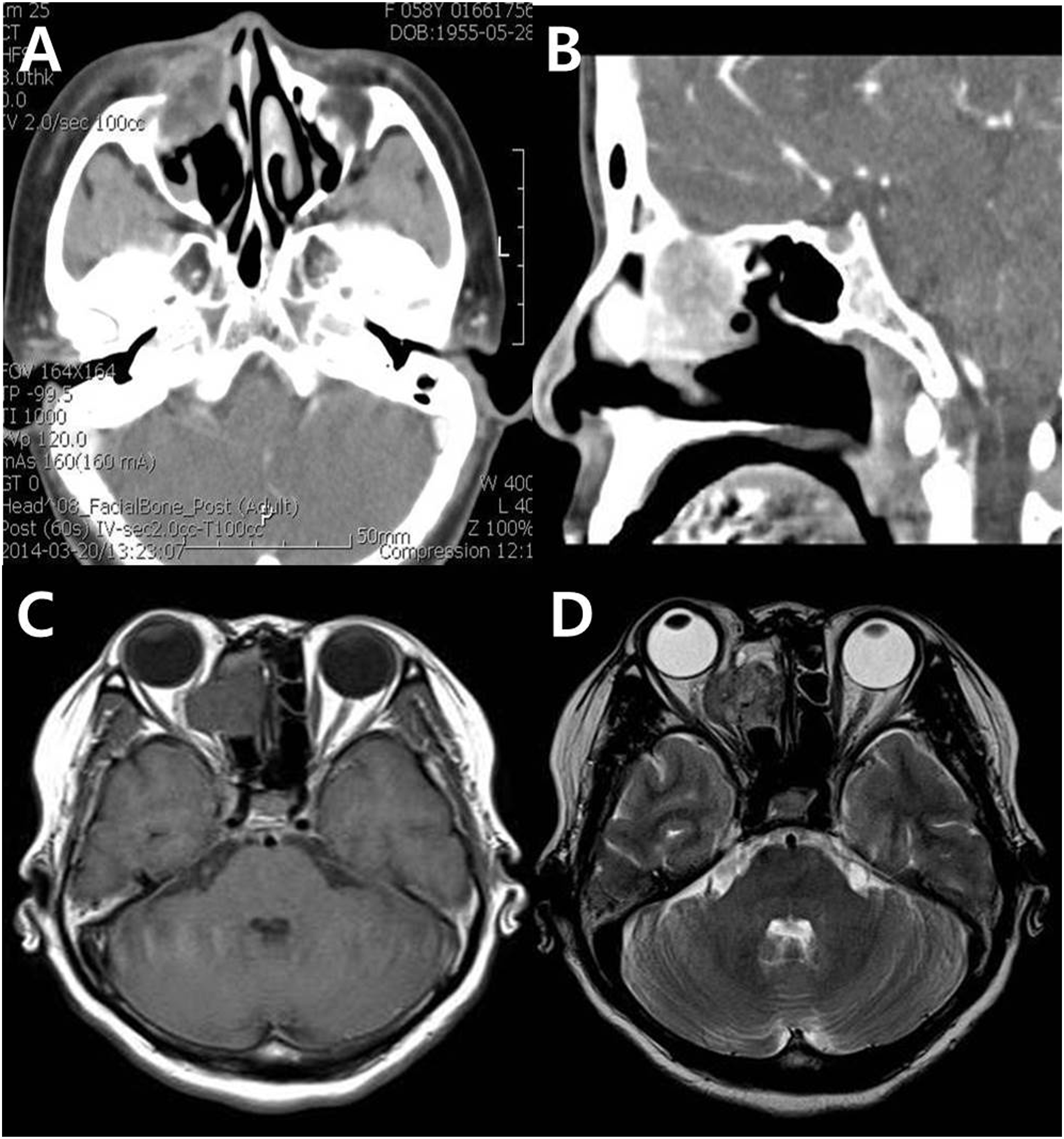
Discussion
Solitary fibrous tumors (SFT) are well-recognized in the pleura, however, occurrence in the nasal cavity is uncommon. Most SFTs in the head and neck region occur in the orbit and upper respiratory tract and tend to behave in a nonaggressive fashion. 2 Microscopically, SFTs are composed of plump spindle cells situated in a collagenous background and have a characteristic “patternless” arrangement. They possess both hypercellular and hypocellular areas, and a portion of the tumor frequently exhibits a hemangiopericytoma-like appearance with strong branching vessels. Histologically, the lesion could be confused with hemangiopericytoma, schwannoma, fibrous histiocytoma, fibrosarcoma, or nasopharyngeal angiofibroma. In addition, it is very difficult to distinguish between the malignant and benign SFTs as most of the malignant SFTs have zones that are morphologically identical to a benign SFT.3,5
Malignant SFTs are extremely rare and it can be difficult to distinguish between benign and malignant SFTs. Generally, the malignant SFTs are larger than the benign SFTs and common gross features are hemorrhage and/or necrosis in the malignant neoplasm. The differential diagnoses from malignant SFT are numerous and include a variety of cell lineages. When including site-specific tumors, it is more difficult to distinguish between mesothelioma or sarcomatoid carcinoma in pleural tumors and “true” hemangiopericytomas of the sinonasal tract.7,8 In particular, and vis-à-vis fine needle aspiration cytology, it is more difficult to make an informed and accurate diagnosis if the high-grade areas are not sampled. So, a larger tumor sample favors malignancy before surgery. Due to the fact that malignant SFTs have a lot in common with other neoplasms, they have a general immunohistochemistry profile and can occur at almost any place. Immunohistochemically, malignant SFT showed a significant positivity for CD34 and bcl-2, but CD34 expression can at times be lost in malignant SFT (Figure 2). Although malignant SFTs have frequently been described as lacking CD34 expression, bcl-2 has been reported to be more consistently positive than CD34 in malignant SFT. The difficulty is multiplied when considering that CD34 expression, a feature that is often relied upon to make a diagnosis of a benign SFT, is often lost in malignant SFT. 9 The treatment of choice for malignant SFTs, from any origin or at any location, is surgical resection. Radiation therapy is of some benefit when clinically appropriate and used in conjunction with chemotherapy.10,11 However, there are still no codified or standardized chemotherapeutic treatments or regimens. A careful follow-up is necessary and would engender the yearly assessment of local recurrence by diagnostic imaging in order to discern or exclude the presence of metastatic disease.
In conclusion, malignant SFTs are difficult to accurately diagnose because the attributes of the malignant lesion can substantially overlap the attributes of the benign SFT. Pathologically, this tumor showed a proliferation of spindle cells with a fascicular pattern interspersed with increased cellularity, cellular pleomorphism, hemorrhage, necrosis, and a high mitotic activity. Immunohistochemical staining revealed diffuse positivity for CD34, CD99, Ki67, and p53.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.