
Abstract
Introduction
Chondrosarcomas (CSs) are the third most prevalent primary bone neoplasm after myeloma and osteosarcoma. Unlike chondroblastic osteosarcoma, these tumors are characterized by the absence of osteoid matrix production. They are predominantly found in the pelvis, extremities, and ribs. In the head and neck region, they constitute 1% to 12% of cases, with a higher incidence among women and individuals under 50 years of age. 1 CS in the head and neck region are commonly found in the mandible, paranasal sinuses, maxilla, and occasionally nasal septum. Diagnosis typically involves imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI), complemented by biopsies to confirm the malignant nature of the tumor. 2
The aim of this study was to describe the clinical findings, management, and outcome of sinonasal tract CS.
Case Report
A 43-year-old woman presented with a history of chronic left lacrimation lasting for 4 months. The condition was painless, and there was no history of blurred vision, prolonged fever, neck mass, or any associated symptoms of the ear or throat. The ophthalmological examination revealed a nonreducible axial left exophthalmos that was nonpainful, with impermeability of the nasolacrimal duct, without diplopia or decreased visual acuity. Nasal endoscopy revealed a tumor in the left nostril that originated from the middle left meatus. The tumor had a nonbleeding pinkish white appearance, destroyed the nasal septum, and extended to the right nostril. It appeared to have a smooth surface with prominent vessels. No palpable lymph nodes were found during neck examination. Neurological examination, the cranial nerves, was normal.
An orbital MRI was performed and revealed the presence of a heterogeneous expansive process (68 mm × 61 mm × 57 mm) with irregular contours. The process included the ethmoidal cells and the left maxillary sinus, prolapsed into the nasolabial and oropharyngeal lumen by filling the choanae and the ipsilateral nasal fossa. It exhibited heterogeneous hyposignal T1 and hypersignal T2 (Figure 1), with weak signal areas in all sequences. After the injection of gadolinium, it was heterogeneously enhanced. The MRI revealed a significant locoregional extension invading the left infratemporal fossa and parapharyngeal space. It made contact with the floor of the sphenoid sinus with contrast enhancement. It destroyed the posterior part nasal septum, the sieve blade, and the posterior part of the hard palate, and infiltrated the soft palate. The left papyraceous lamina was lysed and the inferior and medial walls of the left eye were destroyed, resulting in grade I exophthalmos caused by the left endorbital extension. The optic nerve was displaced laterally and the fatty safety line was lost. No signs of endocranial invasion were detected.

An orbital MRI in sagittal (a) and axial (b, c) section: showing a heterogeneous expansive process with irregular contours. The process invaded the ethmoidal cells, the left maxillary sinus, infratemporal fossa, and parapharyngeal space (), prolapsed into the nasolabial and oropharyngeal lumen. It exhibited heterogeneous hyposignal T1 (c), hypersignal T2 (a, b). The MRI showed invasion of the It destroyed the nasal septum in its posterior part, the sieve blade, the posterior part of the hard palate ( ) and left endorbital extension (
) and left endorbital extension ( ). MRI, magnetic resonance imaging.
). MRI, magnetic resonance imaging.
A biopsy was performed under local anesthesia, and histological and histochemical studies concluded that it was a well-differentiated CS (grade 1). The malignant chondrocytes showed small, round hyperchromatic nuclei and occasional binucleated cells, but mitoses were absent (Figure 2).
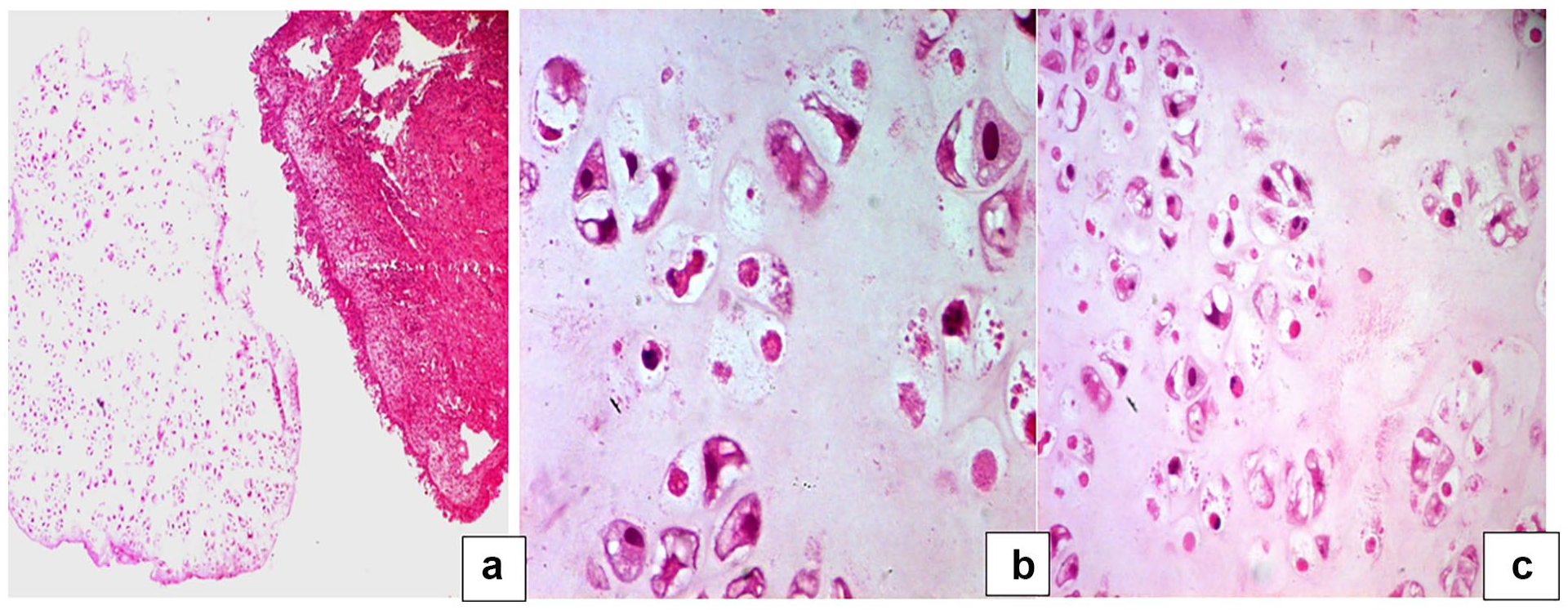
(a) One fragment involved a malignant tumor of cartilaginous differentiation with lobulated growth and slightly increased cellularity, and the second fragment involved a nasal mucosa with acute inflammatory remnants (HE ×50). (b) Malignant chondrocytes show small, round hyperchromatic nuclei and occasional binucleated cells (*), mitoses are absent (HE ×200). (c) Malignant chondrocytes show small, round hyperchromatic nuclei and rare mito-necrosis (*) (HE ×400). HE, hematoxylin eosin.
The patient underwent surgery via a para-lateral-nasal approach, with incomplete resection due to endo-orbital extension. Weber Ferguson incision was performed. The tumor filled both nasal cavities with involvement of the left maxillary sinus and left ethmoid cells. The tumor caused lysis of the left lamina papyracea and extended into the left orbit without invading the orbital adnexa. In addition, the tumor infiltrated the hard palate on the left side and extended to the nasal septum. A bilateral medial maxillectomy was performed, and there was no defect in the hard palate after the excision of the lesion.
The excised specimen was sent to the pathologist who confirmed the diagnosis of CS. The patient’s postoperative recovery was uneventful, and he received adjuvant radiotherapy. However, the patient was then lost to follow-up.
Discussion
CS is a malignant tumor that produces cartilage matrix and accounts for 20% to 27% of all primary bone sarcomas at various anatomical locations. 2 While it is typically found in long bones and pelvic bones, CS can occur in the head and neck region in 5% to 10% of cases. 3 This slow-growing tumor shows a preference for males, with the highest frequency occurring between the ages of 40 and 60. 4 Our patient was a 43-year-old woman.
The occurrence of CS in the paranasal sinus system is exceptionally rare. Notably, the series by Knott, 5 spanning 25 years, describes 13 cases at this location. Other studies, such as Touati et al (2 cases), 4 Krömer et al, 3 and Rowley et al 6 (1 case), also report limited instances. The clinical presentations of CS depend on the extent of the tumor. In the sinonasal region, nasal obstruction is the predominant symptom, accompanied by headaches, epistaxis, anosmia, facial pain, signs of cranial nerve involvement, or visual disturbances, 7 as was the case with our patient who was presented with chronic left lacrimation and nonreducible axial left exophthalmos.
Imaging techniques, such as CT and MRI, play a crucial role in providing detailed information on bone destruction. This includes structures such as the ethmoid blade, orbit walls, and the bony palate. Sinonasal CSs tend to reshape the sinonasal cavity, with the degree of bone erosion correlating with tumor grade. Punctate cartilaginous calcifications are exhibited in well-differentiated tumors.
On MRI, the cartilaginous matrix of CSs exhibits very low signal intensities on T1- and T2-weighted images, with homogeneous or heterogeneous enhancement post-contrast injection. Calcified and ossified regions show very weak signals across all sequences.8,9 MRI aids in detailing the extension into surrounding soft tissues and distinguishing between granulomatous tissue and recurrences during postoperative monitoring of CS.
The histological diagnosis of CS is essential. The most prevalent form is conventional CS, which can be categorized into 4° of malignancy based on cell abundance, nuclear polymorphism, and mitotic rate. Other forms include clear cell CS, mesenchymal CS, and undifferentiated CS. 3 In this case, the CS was categorized as grade 1. When considering the differential diagnosis of sinonasal CS, it is important to also consider conditions such as chondroma, chordoma, and chondromyxoid fibroma.
Surgical excision via bloc resection is the primary treatment approach due to its relative radioresistance. 10 The surgical approach is dependent on the location, extension, and histological grade of the tumor. Obtaining soft surgical margins is crucial for local control. 9
Adjuvant treatment typically involves radiation which is rarely used in isolation. The recommended dose for radiation therapy is 6000 to 7000 Cgy, administered in 30 to 35 fractions. Chemotherapy is specifically reserved for high-grade cases. 11 In this case, the patient received surgical excision as the primary treatment followed by adjuvant radiotherapy. Postoperative radiation therapy is indicated for cases of large tumors, involvement of the skull base or vital neurovascular structures, and subtotal resection, as was the case with our patient. CS survival rates range from 44% to 87%, with resectability being a crucial prognostic factor, as most deaths are due to locally invasive disease. 1 According to a systematic review, patients who undergo radiation therapy have a lower incidence of local recurrence and distant metastases compared to those who receive surgery alone (29.4% vs 32.8%). 12 However, due to the rarity of the lesion and the absence of standardized patient data, drawing definitive conclusions is challenging. 10
Conclusions
CSs in the sinonasal tract are rare. Patients with early diagnosis and appropriate surgical intervention tend to have a better prognosis. The main cause of mortality is unmanageable local disease, which compresses neighboring vital structures.
Footnotes
Acknowledgements
We would like to thank Editage for English language editing.
Author Contributions
EL Omri Malika and Marwa Ben Njima drafted the manuscript. All authors read and approved the final version of the manuscript.
Data Availability
The data used to support the findings of this study are included within the article. Additional data are available on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series since we anonymously reported clinical and imaging information concerning our patient’s case.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.