
Abstract
Ameloblastomas are slow-growing, aggressive odontogenic epithelial tumors that originate from the jawbone. One of the most easily relapsing maxillofacial tumors, ameloblastomas mainly occur in the mandibular molar area and ascending branch, although they can occasionally occur in the nasal cavity and paranasal sinuses. A 14-year-old child with autism spectrum disorder underwent sinus computed tomography (CT) under anesthesia. A swollen tumor had grown in the left maxillary sinus, and the bone of the maxillary sinus was damaged. Nine months after the first operation, recurrence was observed in the left maxillary sinus. The pathological diagnosis was ameloblastoma. Due to the child’s inability to communicate and cooperate with the treatment normally, he underwent endoscopic surgery again combined with low-temperature plasma treatment. No tumor recurrence was found on reexamination 6 months after surgery.
Introduction
Ameloblastomas, one of the most recurrent maxillofacial tumors,1,2 show continuous growth with invasiveness and infiltrate the surrounding tissues. Approximately 50% of ameloblastomas occur in the second decade of life, 3 and these tumors occasionally appear in the nasal cavity and paranasal sinuses. 4 Autism spectrum disorder (ASD) is a neurodevelopmental disorder clinically characterized by impaired social interactions, language disorders, and abnormal interests and behaviors. This paper reports a case of recurrent ameloblastoma of the maxillary sinus in a 14-year-old child with autism.
Case Report
The patient, a 14-year-old boy, was reported by family members to have a cold and was slapping his own forehead at the beginning of his illness. One month later, his left cheek had become swollen. Three months later, the patient developed mouth closure and masticatory and swallowing dysfunction. The child had been diagnosed with ASD at the age of 3 years and was unable to communicate with people normally. After anesthesia and CT, a low-density round mass with expansive destruction of the maxillary sinus bone was found in the maxillary sinus (Figures 1A and B). The preliminary potential diagnoses were as follows: (1) ameloblastoma, (2) maxillary sinus cyst, (3) nasal septum deviation, and (4) ASD. Preoperative sinus CT. Coronal (A) and axial (B) views showing expansive bone destruction of the maxillary sinus and around a low-density mass with greatest dimensions of nearly 6.4 cm × 5.0 cm in the left maxillary sinus. Multiple fine septa and high-density nodules can be seen, the left ethmoid sinus mucosa is thickened, and the nasal septum is bent to the right under pressure. In the CT scans of the sinus before the second operation, the axial view (C and D) shows that the left maxillary sinus was swollen, with a low-density mass showing maximum dimensions of nearly 3.8 cm × 3.5 cm × 5.0 cm. Patchy high density was seen in the lesion, and part of the maxillary sinus wall was eroded. In the CT scan of the sinus obtained 6 months after the second operation, the enhanced CT axial view (E and F) showed no recurrence of the tumor in the left maxillary sinus.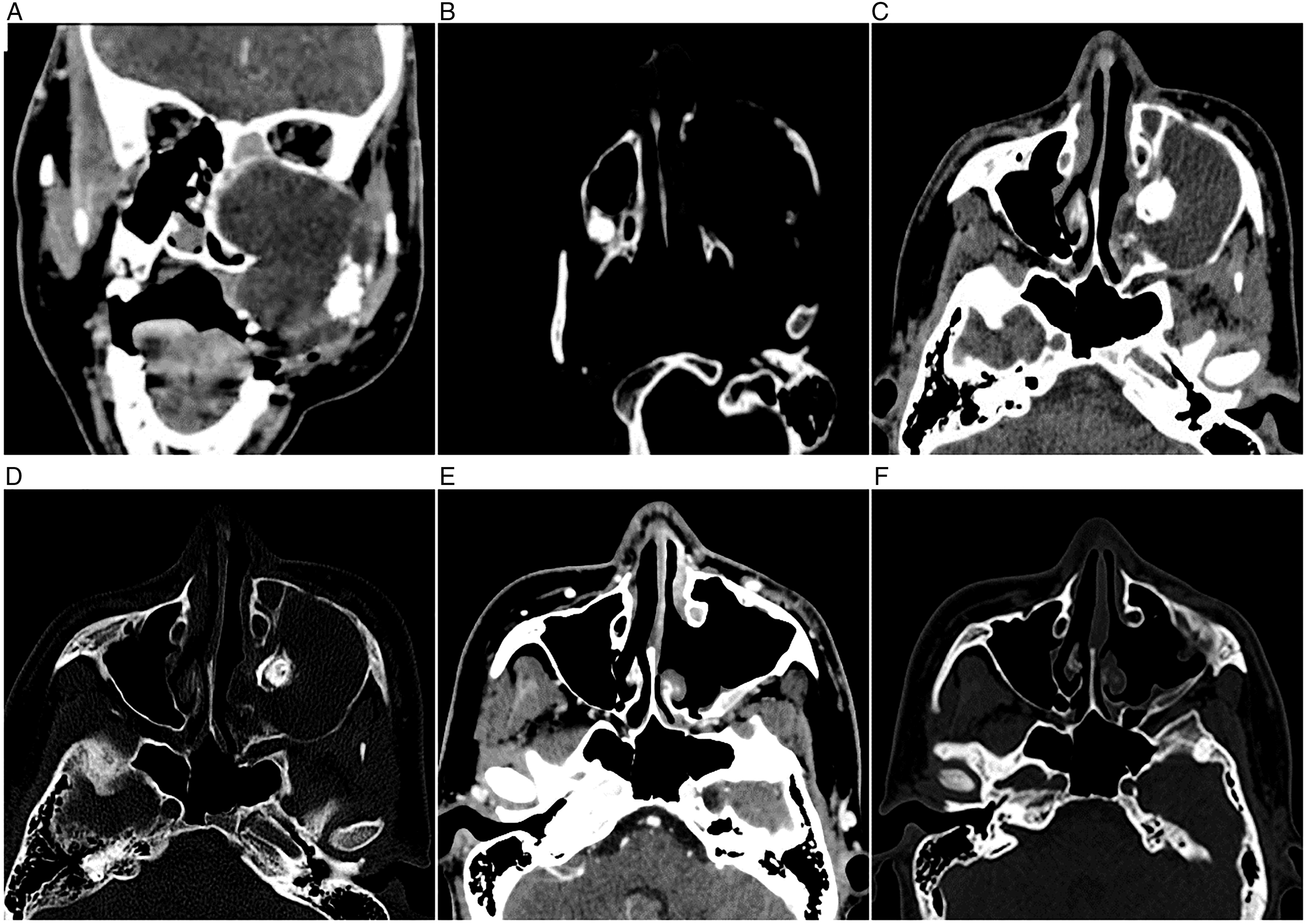
In the first operation, the left uncinate process was resected under 30° nasal endoscopy, and the maxillary sinus was opened. After endoscopic removal of the tumor, the bone of the sinus wall was found to be partially damaged. Postoperative pathological examination revealed an ameloblastoma (Figure 2C). The diseased tissue in the maxillary sinus was peeled off during the operation, and paving stone-like changes were observed on the surface (A). Pathological tissue in the maxillary sinus under nasal endoscopy (B). Pathological results: The (maxillary sinus) capsule wall-like substance is composed of fibrous tissue, which is lined with enamel epithelium and partially lined with squamous epithelium. The enamel epithelium shows many shadow cell nests and calcium salt deposits, and ameloblastoma was considered (C).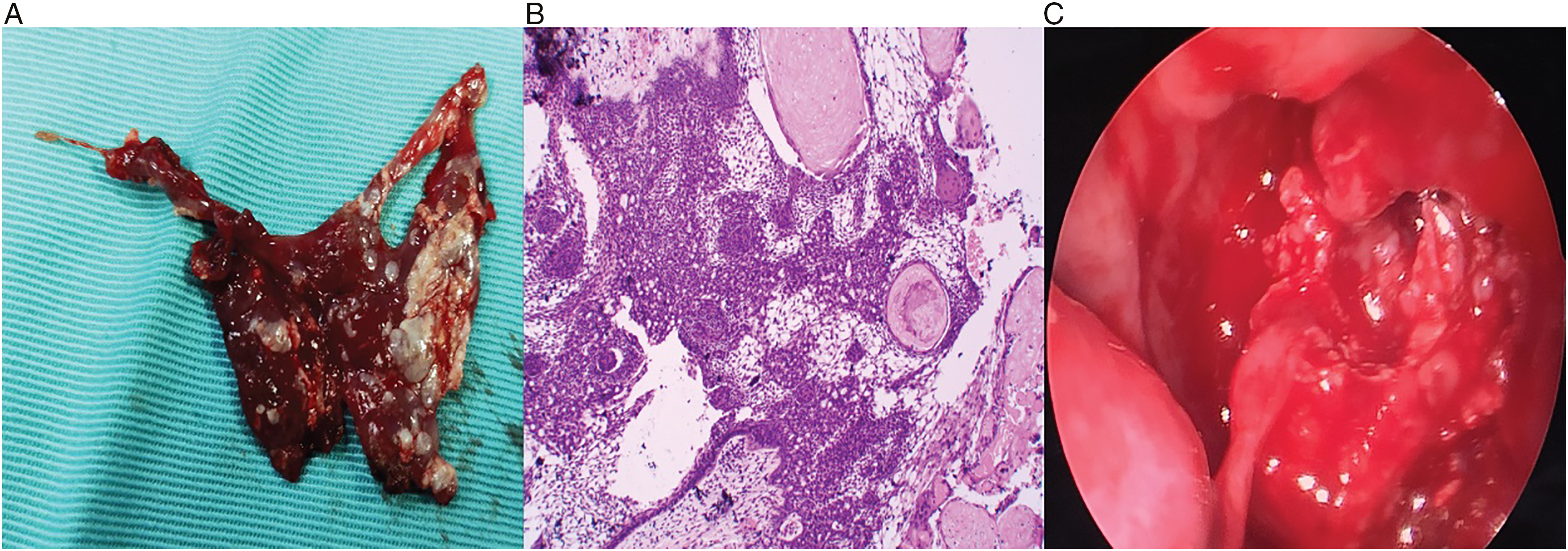
Due to the COVID-19 epidemic, the child could only be re-examined 10 months after surgery. CT examination of the sinus showed a low-density mass in the left maxillary sinus, and tumor recurrence was suspected (Figures 1C and D). In the second endoscopic sinus surgery, the left maxillary sinus was opened using the anterior lacrimal recess approach. After removing the rough-paving stone-like tumors on the capsule wall, the local suspicious tumor tissue at the root of the third upper left molar was burned with a low-temperature plasma knife. Pathological examination revealed an ameloblastoma. A CT scan of the sinus obtained after 6 months showed no tumor recurrence (Figures 1E and F).
Discussion
Ameloblastomas mainly occur in the mandible, although a few occur in the maxilla. 5 Ameloblastomas originating in the nasal cavity and paranasal sinuses, including the nasal cavity, 6 maxillary sinus, 7 and ethmoid sinus, 8 are rare. The histological features of ameloblastomas vary, and these lesions are currently categorized into 5 histological types: follicular, plexiform, acanthoma, basal cell, and granular cell types. The tumors are usually gray–white or pink, have a smooth surface and a tough texture, and easily bleed when touched. Some studies suggest that the age of people with ameloblastomas in the nasal cavity and paranasal sinuses is usually 60-80 years, with an average age of 59.7 years. These tumors often occur in men and mainly present with nasal congestion, epistaxis, and sensory abnormalities. Additionally, some patients may report facial tenderness.9-11 The diagnosis of ameloblastoma currently depends on clinical symptoms and imaging and histopathological findings. The ameloblastoma in the child in this report originated from the maxillary sinus, which is a relatively rare presentation in clinical practice. The age of onset was only 14 years, which is lower than the average age. The child showed no typical symptoms such as epistaxis during the early stages. Due to his ASD, he was unable to convey whether he had any symptoms such as abnormal sensation and nasal congestion. Before they noticed the swelling of the left cheek, his family members only noted that the child had a “cold” and then slapped his forehead. Because the child was not sufficiently cooperative to undergo CT scans and nasal endoscopy when awake, he was diagnosed with “chronic sinusitis” many times in the early stage, until his cheek swelled and affected his swallowing ability. CT examination of the paranasal sinuses under general anesthesia was subsequently performed. Due to the child’s inability to accurately describe his medical history and cooperate in the examination, differential diagnosis of the disease became increasingly difficult.
Preoperative imaging can show the size and scope of the tumor and provide the basis for choosing the appropriate operation time and method. CT showed a low- or mixed-density cystic area, which was multilocular, honeycomb-like, or unicameral. Bone resorption or destruction may occur because of tumor enlargement. In this case, a CT scan revealed a circular low-density mass in the left maxillary sinus and a high-density nodule, resulting in expansive destruction of the maxillary sinus bone. The disease was differentiated from nasal polyps, inverted papilloma, and chondroma.
Ameloblastomas do not respond to radiotherapy and chemotherapy, and surgical resection is the primary treatment for these tumors, which are characterized by infiltrative growth and easy relapse after curettage. 12 The initial treatment has a major influence on the postoperative recurrence of ameloblastoma. Improper surgical treatment destroys the integrity of primary ameloblastomas, which can easily cause residual tumors and implantation followed by repeated episodes of relapse. 13 The surgical methods and scope of treatment vary among patients and can be divided into conservative surgery (simple tumor resection) and radical surgery (Kelu approach, nasal incision, and partial or total maxillary resection). Due to their concerns about the child’s inability to take care of himself after partial maxillary resection, his family members refused the procedure and opted for endoscopic resection of the maxillary sinus tumors.
The recurrence rate varies with the treatment. The prognosis of radical surgery is better and its recurrence rate is lower. Cryotherapy after curettage can effectively reduce the recurrence rate of ameloblastoma. 14 Although the recurrence rate shows no significant correlation with sex and age, it has been shown to be related to disease duration as well as the location and type of the tumor. Ameloblastomas with long-duration lesions and roots in the maxilla have a higher recurrence rate and poorer prognosis than those in the mandible. The cure rate of follicular-type lesions is low, and they relapse easily, whereas the postoperative recurrence rate of the plexiform-type lesions is lower, and their prognosis is better. 15 Ameloblastomas can destroy the surrounding adjacent bone, leading to bone resorption because of the secretion of receptor activator of nuclear factor kappa-Β ligand (RANKL) and tumor necrosis factor (TNF)-Q. 16 The patient in this case showed recurrent ameloblastoma 9 months after the first operation, which was related to the first conservative operation. The initial treatment only involved scraping along the surface of the tumor, and the bone tissue in contact with the tumor surface was not removed. Although this treatment causes less damage to the facial shape and oral function of patients, the retained bone tissue may have residual lesions and lead to recurrence. Before the second operation, the treatment team suggested radical surgery, but the family members refused because of the difficulty of postoperative maxillary reconstruction, the child’s inability to cooperate independently after the operation, and concerns about serious complications. After discussion, the patients’ family agreed to endoscopic surgery. The tumor was completely removed using a nasal endoscope and local ablation of the tumor root pedicle around the left upper third molar was performed using low-temperature plasma. Six months after the surgery, the treatment effect was good, and no tumor recurrence was found on a CT scan of the paranasal sinuses. Follow-up assessments of the patient are ongoing.
Conclusions
Patients with autism have low verbal and nonverbal comprehension, which increases the difficulty of diagnosis, treatment, and postoperative reexamination of ameloblastoma of the maxillary sinus. The findings of this case also highlight the need to be alert to the possibility of tumor lesions of the maxillary sinus in patients with ASD and other conditions that involve a lack of autonomous behavioral ability. CT examination of the sinus is helpful for early detection and diagnosis of the disease. Early detection and definitive diagnosis are key to antitumor efforts. For patients with autism, anesthesia can facilitate imaging examinations. In comparison with traditional partial maxillectomy, nasal endoscopic surgery combined with low-temperature plasma ablation can significantly improve the quality of life of children and reduce the incidence of postoperative complications, which is worthy of further exploration and observation.
Footnotes
Acknowledgements
We thanks SAGE for the proper English language, grammar, punctuation, spelling, and overall style service.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Fund of
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.