
Abstract
Tuberculosis (TB), an infectious disease caused by Mycobacterium tuberculosis (MTB), can affect the lungs (pulmonary TB) as well as other sites (extrapulmonary TB). Nasopharyngeal tuberculosis (NPTB) is a rare type of extrapulmonary TB. Since NPTB has nonspecific clinical presentation with low index of suspicion, it is difficult for clinicians to make an early diagnosis and proper treatment. We recently encountered a 42-year-old woman with NPTB concomitant with middle ear TB, which strongly mimicked nasopharyngeal carcinoma. Since the diagnosis of NPTB was difficult to confirm based on endoscopic findings and imaging studies, this patient underwent nasopharyngeal biopsy, and finally, polymerase chain reaction (PCR) confirmed NPTB. This report describes our NPTB case as well as summarizes all cases of NPTB reported in South Korea. We highlight that active tissue biopsy with antibacterial smear and additional PCR or specific TB blood test should be considered for cases with high suspicion of NPTB.
Introduction
Nasopharyngeal tuberculosis (NPTB) is a rare type of extrapulmonary tuberculosis (TB). Systemic symptoms of NPTB include cervical lymph node enlargement and nasopharyngeal symptoms such as ear fullness, otorrhea, rhinorrhea, and nasal obstruction. 1 Endoscopic examination for NPTB showed various findings such as irregular, ulcerative, or bulging mucosa, mass-like lesion, a whitish patch, and even normal appearance in some cases.2,3 Since clinical symptoms and objective findings of patients with NPTB are similar to those of other diseases including necrotizing granulomatous disease and nasopharyngeal cancer, the precise diagnosis of NPTB is often delayed.1,4,5 Further, in practical settings, NPTB requires early diagnosis and proper treatment because it is an airborne infection and easily transmissible through droplets. 4 We recently encountered a 42-year-old woman who presented with ear fullness in the left ear with ipsilateral otorrhea that had developed over 2 months prior to hospital visit. Initial endoscopic findings showed a diffuse bulging lesion on the posterior wall of the nasopharynx and a white patchy mucosa covering the left nasopharynx. The pathologic lesion showed no improvement even after a few weeks of antibiotic treatment; therefore, endoscopic biopsy was performed. The lesion was finally diagnosed as NPTB based on pathologic confirmation using the polymerase chain reaction (PCR) test. The patient was referred to the infectious department, and NPTB was successfully controlled by treatment with anti-TB drugs. This case highlights the importance of bacterial culture with PCR analysis in patients with highly suspicious of NPTB. Further, a summary of all reported NPTB cases in South Korea has been presented herein.
Case Presentation
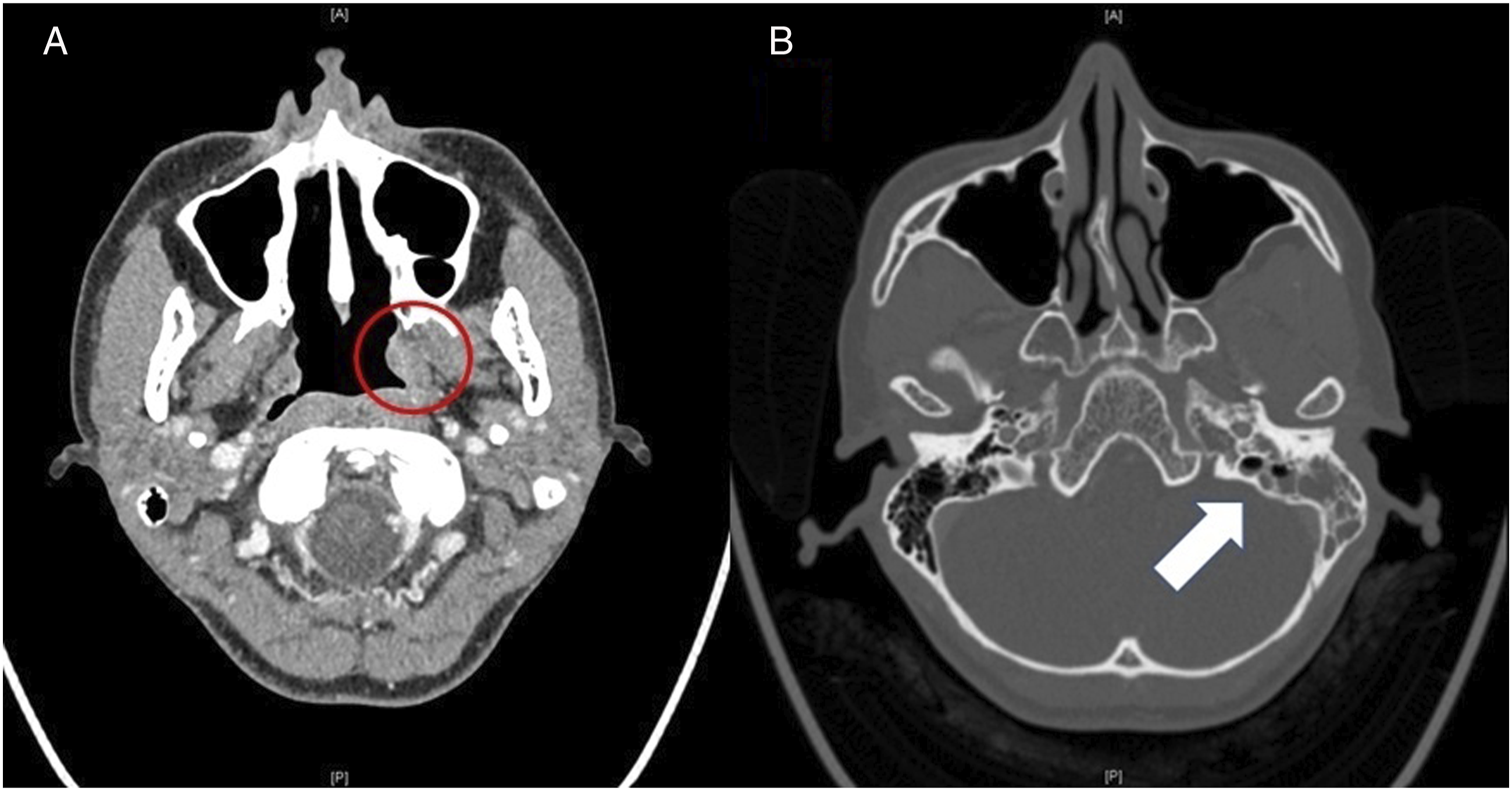
A 42-year-old woman presented with ear fullness and otorrhea, which had lasted for 2 months prior to the hospital visit. She had no medical history of hypertension, diabetes mellitus, or asthma. Nasal endoscopic examination performed at the first visit revealed that both nasal cavities were clear. However, a diffuse bulging lesion on the posterior wall of the nasopharynx and white patchy mucosa of the left nasopharynx were observed (Figure 1A). A tympanoscopic examination revealed a left tympanic membrane perforation with wet discharge (Figure 1B). Paranasal sinus computed tomography (CT) revealed a poorly enhanced bulging lesion in the left nasopharynx with concomitant left otomastoiditis (Figure 2). Initial laboratory examination revealed normal white blood cell (6230/mm3), neutrophil (70.0%), and lymphocyte (23.5%) counts, as well as normal levels of systemic inflammatory markers including erythematous sedimentation rate and C-reactive protein. Chest radiography revealed no signs of pulmonary TB. Endoscopic examination: (A) Nasal endoscopic examination shows mucopurulent discharge from the left nasopharynx and diffuse bulging lesion on the posterolateral wall of the nasopharynx. (B) Tympanoscopic examination shows a left tympanic membrane perforation with mucopurulent discharge. Computed tomography of the paranasal sinuses: (A) No clearly identified mass-like lesion in the posterior nasopharynx and poorly enhanced bulging lesion on the lateral wall of the left nasopharynx (red circle). (B) Concomitant left otomastoiditis (white arrow).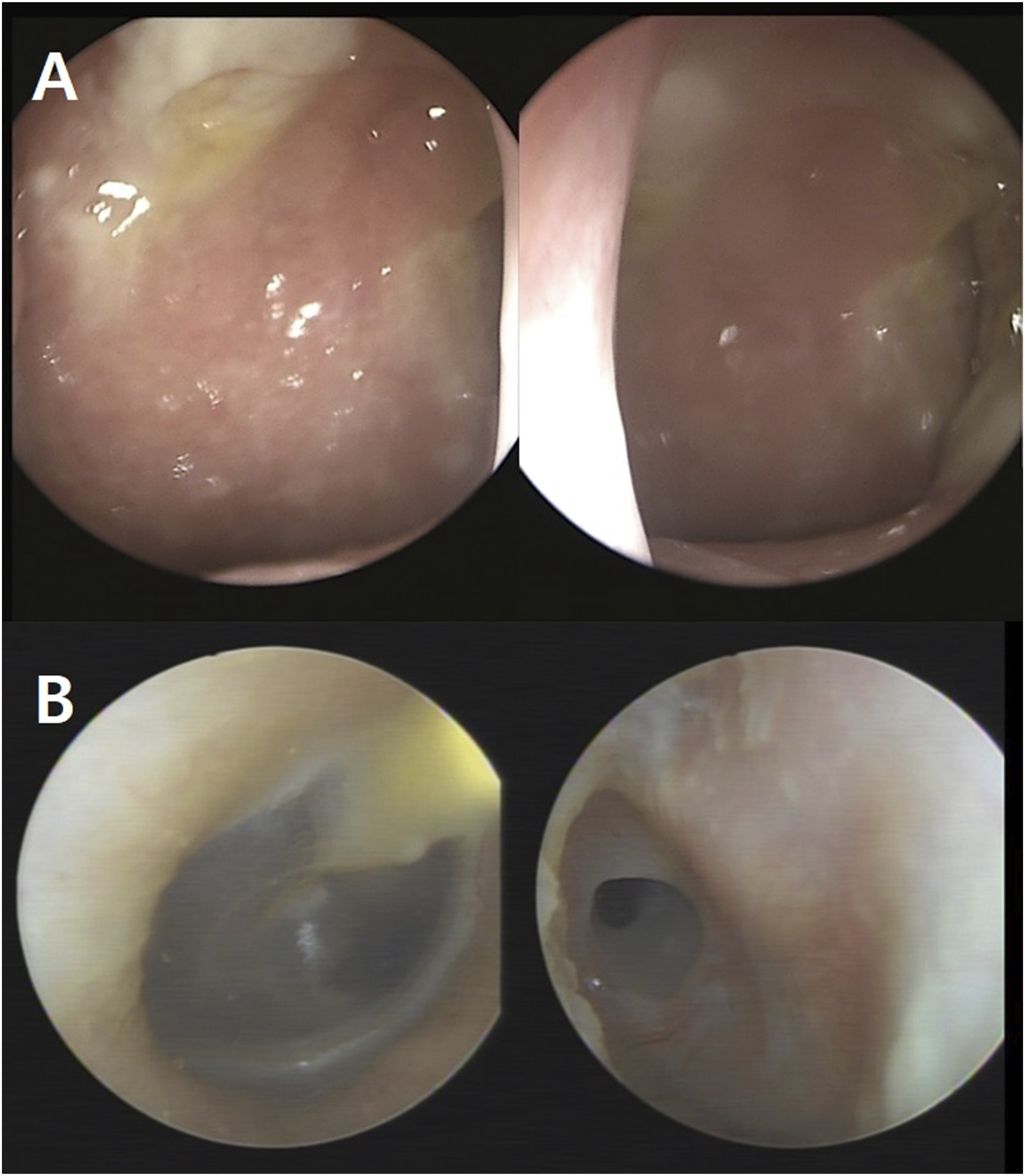
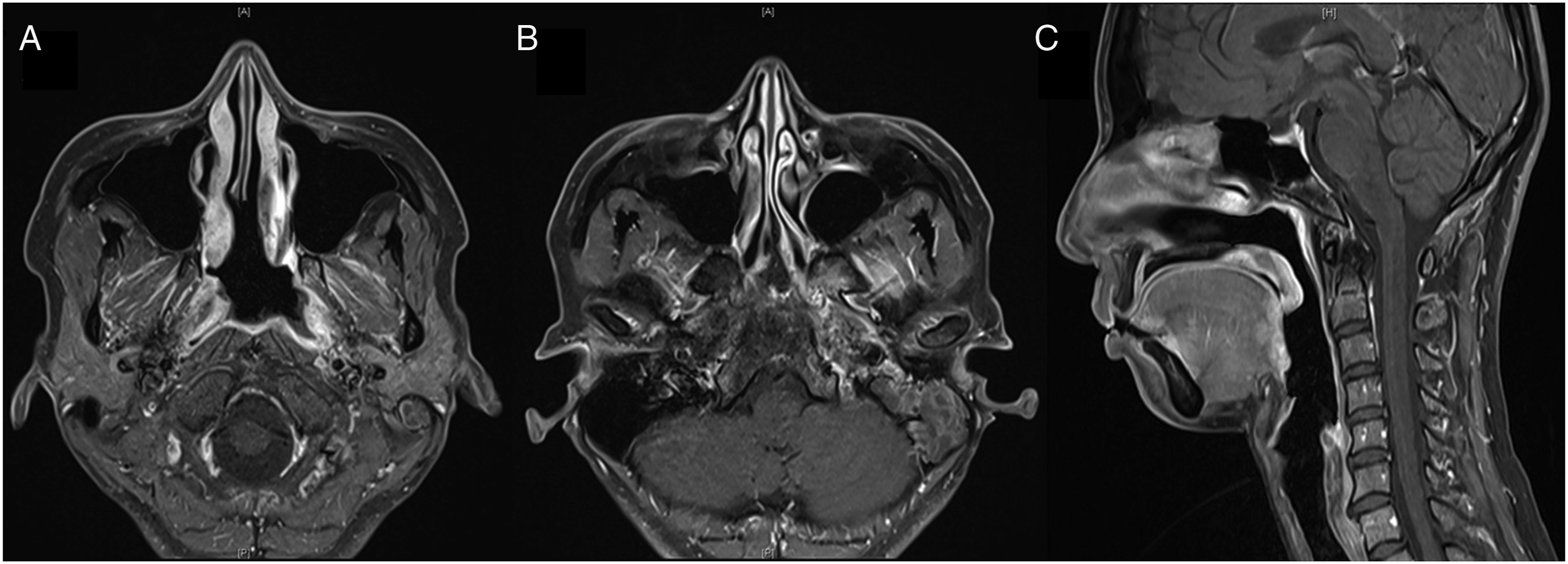
The patient did not complain of any nasal symptoms such as nasal pain or postnasal drip, but otologic symptoms such as otorrhea and otalgia. Since otorrhea and nasopharyngeal discharge with otalgia were not controlled by antibiotics, endoscopic biopsy was performed under general anesthesia at 2 weeks after the first visit. During the operation, diffuse bulging lesions were noted on the posterior wall of the nasopharynx (Figure 3A). Frozen biopsies were examined twice, and both showed chronic granulomatous inflammation. The permanent pathology revealed the chronic granulomatous inflammation (Figures 3B and 3C). The Ziehl–Neelsen stain for acid-fast bacilli was performed to rule out the possibility of localized TB, and the result was negative, but caseous necrosis was noted (Figure 3D). The mucopurulent discharge from the nasopharynx around the Eustachian tube (ET) with active otorrhea did not improve with intravenous antibiotics. Therefore, we evaluated the paranasal sinuses using magnetic resonance imaging (MRI), which showed regional mild mucosal thickening with high signal density confined to the lateral nasopharynx with otomastoiditis (Figure 4). There was no significant pathologic lymph node enlargement or extension of the disease into the skull base. Gross and pathologic finding: (A) Diffuse bulging lesion can be noted on the posterior wall of the nasopharynx and mucopurulent discharge on the left Eustachian tube opening (white arrow). (B) Hematoxylin and eosin (H&E) stain, ×100; permanent section of frozen tissue showing chronic granulomatous inflammation. (C) H&E stain, ×200; permanent section of frozen tissue showing chronic granulomatous inflammation. (D) Ziehl–Neelsen stain; caseous necrosis on the left lower end but negative for acid-fast bacilli (black arrow). Magnetic resonance imaging (MRI) of the paranasal sinuses: (A) MRI T1 gadolinium enhancement axial view, regional mild mucosal thickening, confined to the left lateral nasopharynx (white arrow). (B) MRI T1 gadolinium enhancement axial view, otomastoiditis, left. (C) MRI T1 gadolinium enhancement sagittal view, no extension into the parapharyngeal, retropharyngeal space, or central skull base.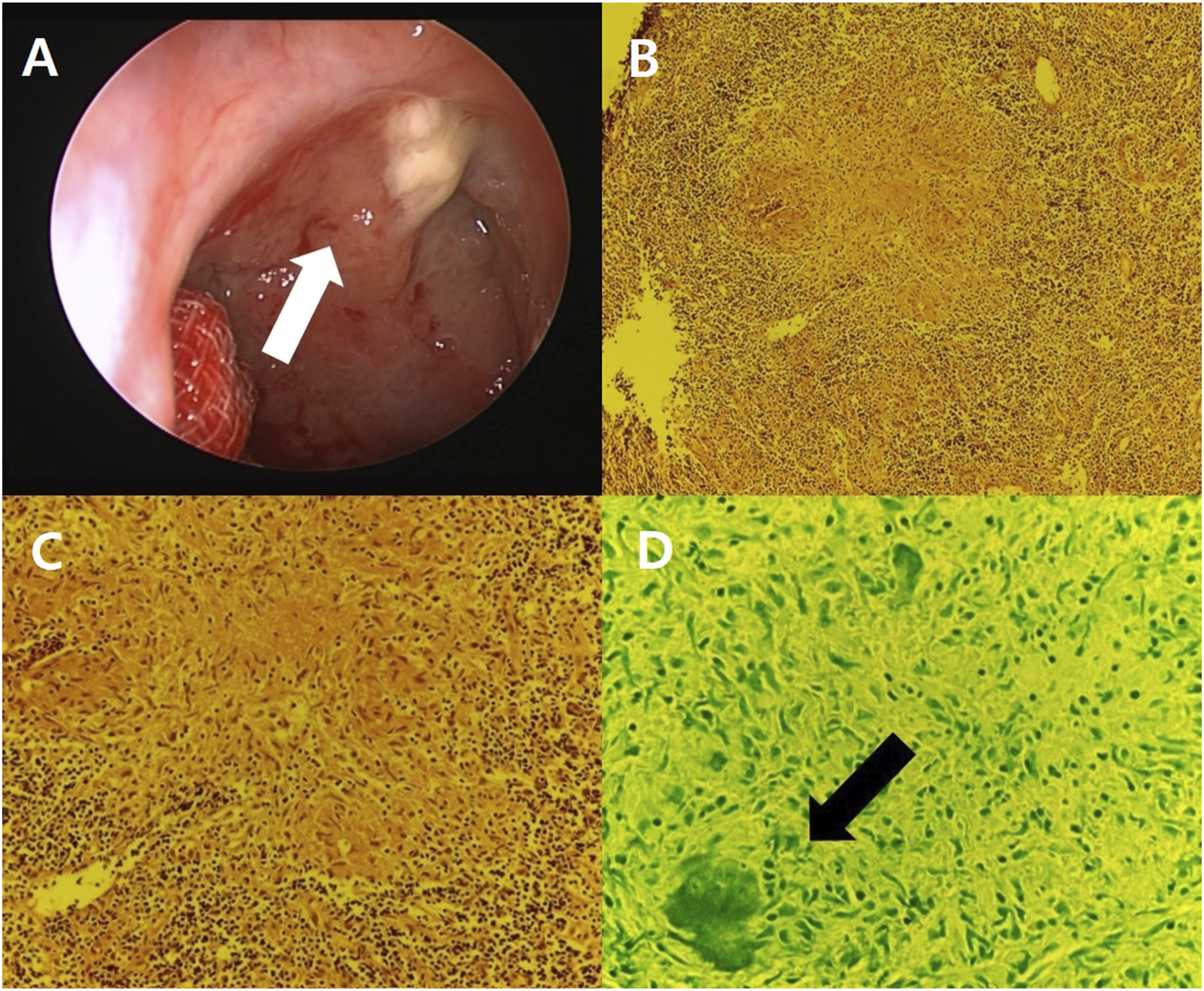
Finally, we decided to perform real-time PCR for mycobacterium tuberculosis (MTB)/non-tuberculosis mycobacterium (NTM) on the biopsy specimen. The result was positive for MTB and negative for NTM in spite of no evidence of pulmonary TB on chest radiography. Additionally, the culture from the left otorrhea was examined, and the real-time PCR result was the same as that from the nasopharynx. After diagnosis of primary NPTB concurrent with middle ear TB, the patient was referred to the department of infectious disease and started anti-TB drugs (HERZ). After taking anti-TB drugs, the nasopharyngeal lesion gradually improved.
Discussion
According to the World Health Organization 2020 Global TB Report, extrapulmonary TB accounted for 16% of the 7.1 million incident TB cases that were reported in 2019. 6 Nasopharyngeal tuberculosis, which was first reported in 1761 by Giovanni Morgagni, 7 can be identified in less than 1% of head and neck TB cases. 8 Although NPTB is uncommon in previous literature, improvement of diagnostic techniques and increased awareness of the disease has led to a recent increase in reported cases. 9
Nasopharyngeal tuberculosis can be classified as either spontaneous nasal TB, which occurs secondary to pulmonary TB, or as primary nasal TB, which occurs without a prior pulmonary TB infection. 7 The route of infection can be the following: (1) through the ET from the sputum of pulmonary TB patients, (2) spread along the ET from a nasopharyngeal lesion, (3) or by hematogenous transmission. 10 Nasopharyngeal tuberculosis can also spread through the rich lymphatic network of Waldeyer’s ring.10,11 Primary nasopharyngeal infection can develop by inhalation of tubercle bacilli. Although normal respiratory mucous membranes are markedly resistant to invasion by the tubercle bacillus, local trauma such as atrophic rhinitis, poor dentition, and weakened host immune systems due to malnutrition or other reasons are predisposing factors to TB infection. 2 The reported cases in South Korea 9 female and 3 male NPTB patients have been reported so far, with most cases involving young individuals, and there were no immune deficiency patients. Our patient was also young immunocompetent female patient, so clinicians should be aware that even normal immune system can be susceptible to TB infection.
Nasopharyngeal tuberculosis is a rare clinical condition that is difficult to diagnose early and treat properly due to nonspecific symptoms and various endoscopic findings that mimic those of inflammation or cancerous lesions. 1 The most common symptoms of NPTB are cervical lymphadenopathy, weight loss, fever, epistaxis, nasal obstruction, hearing loss, otalgia, tinnitus, postnasal drip, and night sweats.1,2 Because endoscopic findings in nasopharyngeal cancer include necrotizing and granulomatous nasopharyngeal lesions that are also likely to be observed in NPTB, imaging studies such as CT or MRI are needed for differential diagnosis and evaluation of disease extent. 11 Unlike nasopharyngeal cancerous lesions, NPTB is usually confined to the nasopharyngeal area without invasion into the surrounding structures such as the skull base, prevertebral muscle, nasal cavity, and oropharyngeal area. Cervical lymphadenopathy can also be detected in both nasopharyngeal cancer and NPTB. 12 Due to limitations in differential diagnosis using clinical manifestations and imaging studies, pathologic confirmation is needed to diagnose NPTB in such cases.
In pathologic studies, gross findings of NPTB are also difficult to distinguish from those of other nasopharyngeal diseases such as nasopharyngeal cancer, lymphoma, Wegener’s granulomatosis, angiofibroma, fungal infection, and sarcoidosis. 4 Therefore, immunohistochemical staining can be a useful differential diagnostic method in such cases. Microscopic findings of NPTB show caseating granulomatous inflammation with multinucleated giant cells of the Langhans type and foreign body giant cells with or without necrosis. 4 Moreover, chronic granulomatous inflammation with positive Ziehl–Neelsen stain for acid-fast bacilli has also been reported.2,9 However, in the present case, biopsy confirmed chronic granulomatous inflammation with negative acid-fast bacilli stain, and the real-time PCR for MTB/NTM was positive for MTB. 4 Therefore, more sensitive TB-PCR test should be considered to confirm suspected NPTB patients to avoid misdiagnosis, facilitating early treatment.
Summary of Reported Cases of Nasopharyngeal Tuberculosis in South Korea.
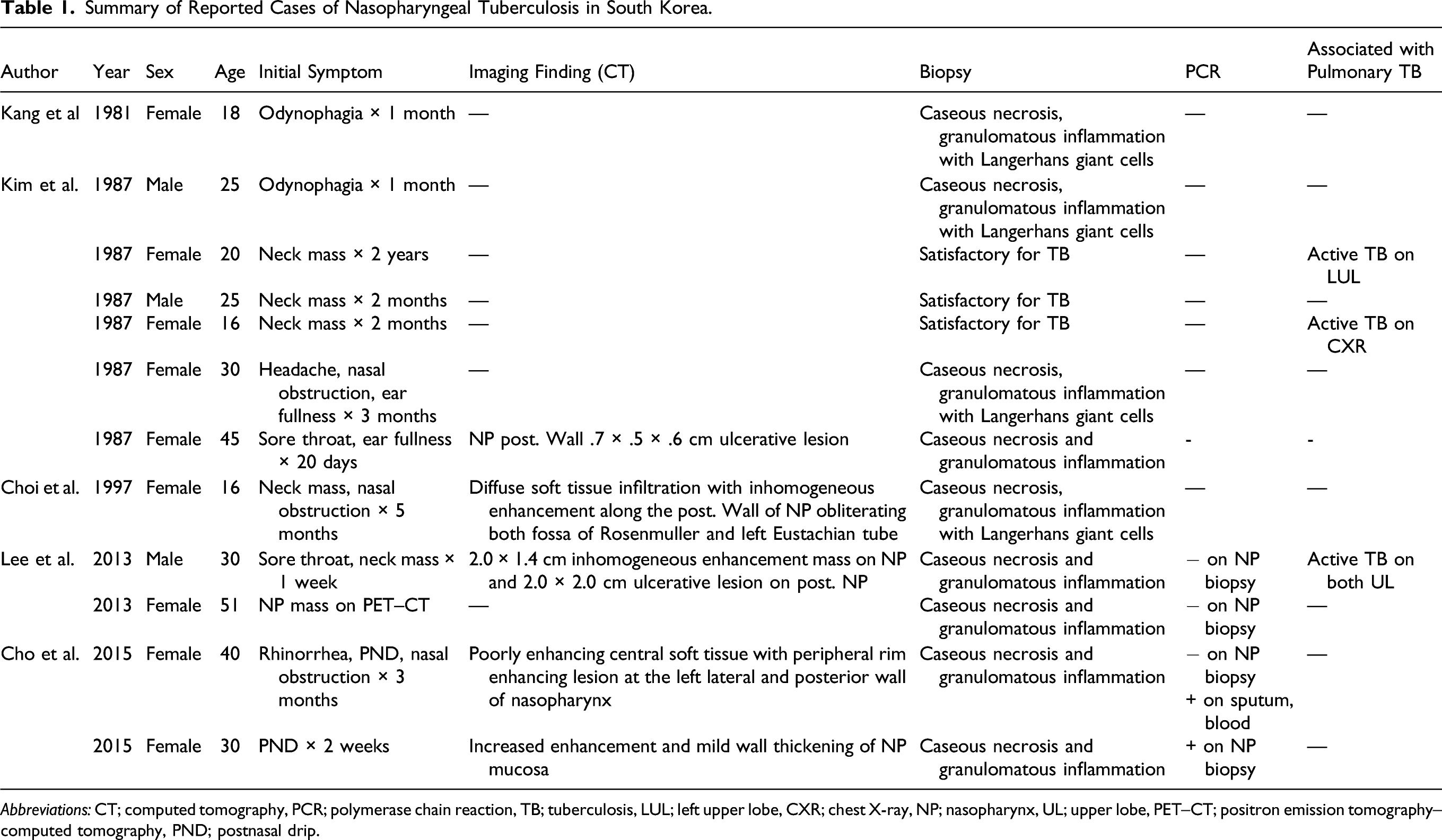
Abbreviations: CT; computed tomography, PCR; polymerase chain reaction, TB; tuberculosis, LUL; left upper lobe, CXR; chest X-ray, NP; nasopharynx, UL; upper lobe, PET–CT; positron emission tomography–computed tomography, PND; postnasal drip.
Conclusion
Early diagnosis and treatment of NPTB are vital for preventing further transmission. For nasopharyngeal lesions that do not respond to preliminary treatment, active tissue biopsy and antibacterial smear should be performed first. Additionally, TB-PCR, QuantiFERON TB blood test, or TB-specific interferon-gamma test should be considered in suspected NPTB patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a faculty research grant of Yonsei University Wonju College of Medicine for 2022-52-0054 (granted to E.J.L.) and the Basic Science Research Program through the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT) (NRF-2021R1A2C1010082, granted to E.J.L.).
Ethical Approval
Ethical approval to report this case was obtained from the Institutional Review Board (IRB) of the Yonsei University Wonju College of Medicine.
Statement of Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.