
Abstract
Mantle cell lymphoma (MCL) is a subtype of B-cell lymphoma derived from CD5-positive antigen-naïve pre-germinal center B-cells within the mantle zone that surrounds normal germinal center follicles. MCL comprises approximately 5 to 10% of all lymphomas. Tonsil is the most common location of MCL in the head and neck region, followed by the nasopharynx. Primary MCL involving the nasopharynx is extremely rare. Its clinical course is very aggressive with frequent relapses after conventional chemotherapy. It always presents as a protruding mass on the mucosal lining of the pharyngeal cavity. Here, we report a new nodular type of MCL in the nasopharynx. Endoscopically, this case showed multiple nodular lesions of primary MCL on the nasopharyngeal mucosa. This unique finding has not been reported yet in the English literature. These lesions should be differentiated from simple pharyngeal infections or benign lymphoid hyperplasia in the nasopharynx.
Introduction
Nasopharyngeal masses are difficult to diagnose because of their location and silent growth. Generally, non-Hodgkin lymphoma of the nasopharynx shows a homogeneous tumor that tends to diffusely involve all walls of the nasopharynx and spreads in an exophytic fashion to fill the airway.1,2 These tumors can cause chronic rhinorrhea, recurrent epistaxis, and nasal obstruction. 5 In contrast, nasopharyngeal carcinoma has a propensity to invade deeply and spread superiorly into the skull base. 3 Mantle cell lymphoma (MCL) is diagnosed by examining the affected tissue obtained from a lymph node biopsy, tissue, bone marrow, or blood sample to observe its typical morphology of monomorphic small- to medium-sized lymphoid cells with irregular nuclear contours.4-6 MCL can develop on the mucosa of all parts of the body, including the pharynx and gastrointestinal (GI) tract. MCL lesions in each part of the GI (esophagus, stomach, and intestines) vary in appearance. 7 They are classified into several subtypes according to the gross findings. However, when MCL occurs on the mucosa of the pharynx, including the tonsil and nasopharynx, it is mostly characterized as a protruding mass in the pharyngeal cavity, which results in a foreign body sensation or respiratory problems. Unfortunately, the subtypes of pharyngeal MCL have not been classified or reported yet in the English literature. MCL is easily diagnosed by a simple biopsy from the pharyngeal mass in the involved space. However, when the pharyngeal mucosa shows hyperemic injection or nodular hyperplasia, this lesion is frequently diagnosed as simple lymphoid hyperplasia or lymphadenitis. Moreover, when MCL in the pharyngeal cavity shows a nodular scattered lesion, a diagnosis of MCL of the nasopharynx is difficult. Here, we report a rare case of nodular-type nasopharyngeal MCL.
Patient
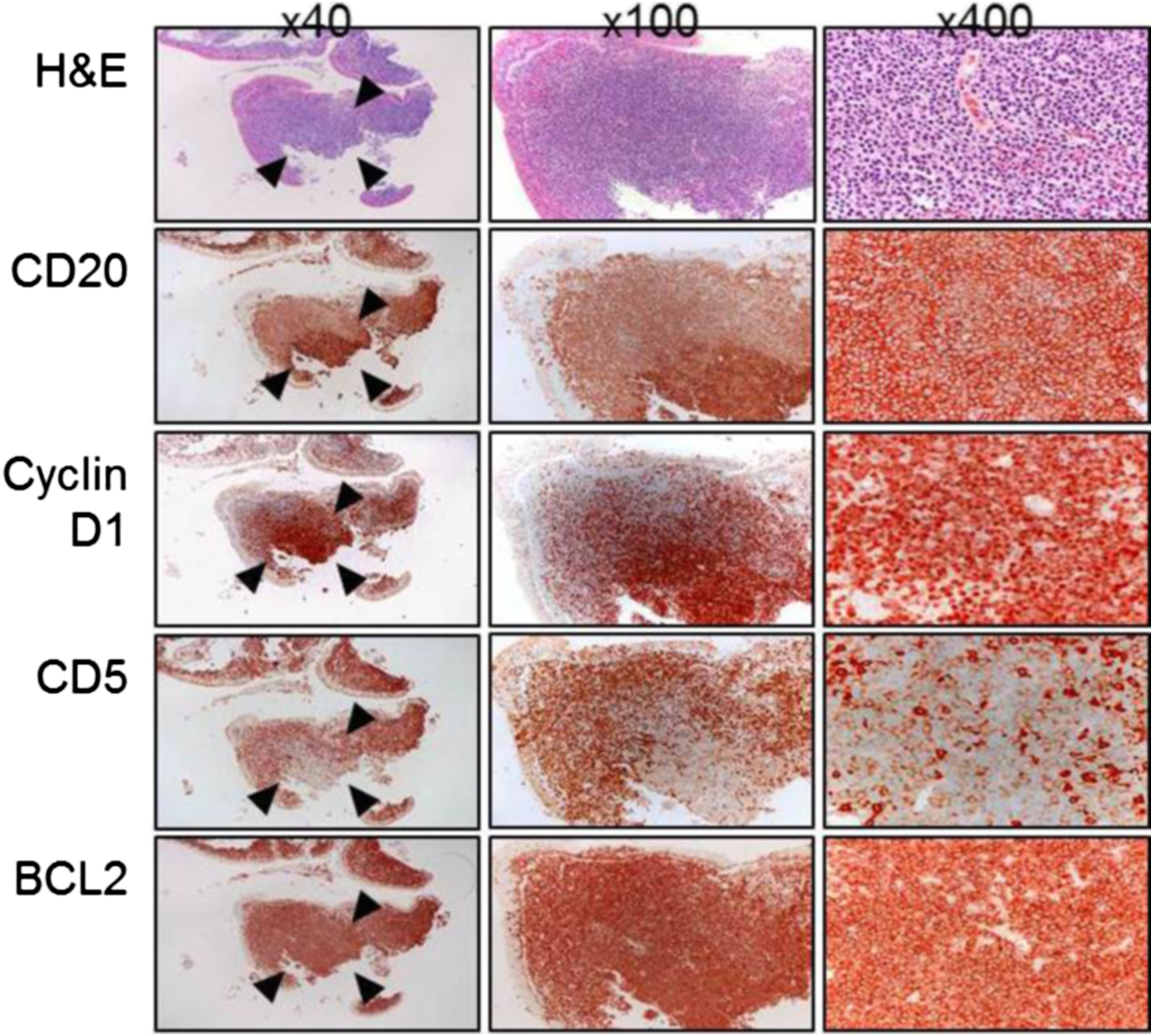
A 68-year-old male visited the authors’ clinic with throat dryness and foreign body sensation in the neck. He had a 4-month history of throat discomfort without any other symptoms such as a neck mass, voice change, dysphagia, or weight loss. He presented with nonspecific symptoms commonly encountered in daily practice that mimicked those of an upper respiratory infection. The patient was a heavy alcohol drinker and smoker (40 pack-years). We initially performed fiberoptic nasopharyngoscopy and neck palpation for head and neck evaluation. On fiberoptic examination, multi-nodular scattered lesions with a hyperemic injection of mucosa were noted on the whole surface of both nasopharynxes without the involvement of the lateral part of both torus tubarius (Figure 1). These lesions extended along both lateral walls of the nasopharynx. We obtained a pathologic specimen via fiberoptic biopsy. The histologic findings revealed mantle cell lymphoma of the nasopharynx. Tumor cells aggregated in the submucosa and formed vague nodular aggregations. These tumor cells were small with inconspicuous nuclei. Immunohistochemically, the tumor cells were positive for CD20, cyclin D1, BCL2, and weakly positive for CD5, but negative for CD3 (Figure 2). The findings were consistent with MCL. The patient underwent positron emission tomography/computed tomography (PET-CT) for whole-body evaluation. Both nasopharynxes showed mild fluorodeoxyglucose (FDG) uptake. However, the cervical lymph nodes did not show FDG uptake. Small lymph nodes with mild FDG uptake were noted in the periportal, left paraaortic, and pericaval areas. The patient was transferred to the department of hemato-oncology for whole-body evaluation and treatment. Typical endoscopic findings of a nodular lesion of mantle cell lymphoma. Multiple nodular and scattered lesions on the posterosuperior wall of the right nasopharynx (A) and left nasopharynx (B), lateral wall of the right nasopharynx (C), and left nasopharynx (D). Histologic findings of mantle cell lymphoma in the pharynx. Tumor cells are aggregated in the submucosa and form vague nodular aggregations as indicated by the arrowheads. The tumor cells are small with inconspicuous nuclei. Immunohistochemically, the tumor cells were positive for CD20, cyclin D1, BCL2, and weakly positive for CD5, but negative for CD3.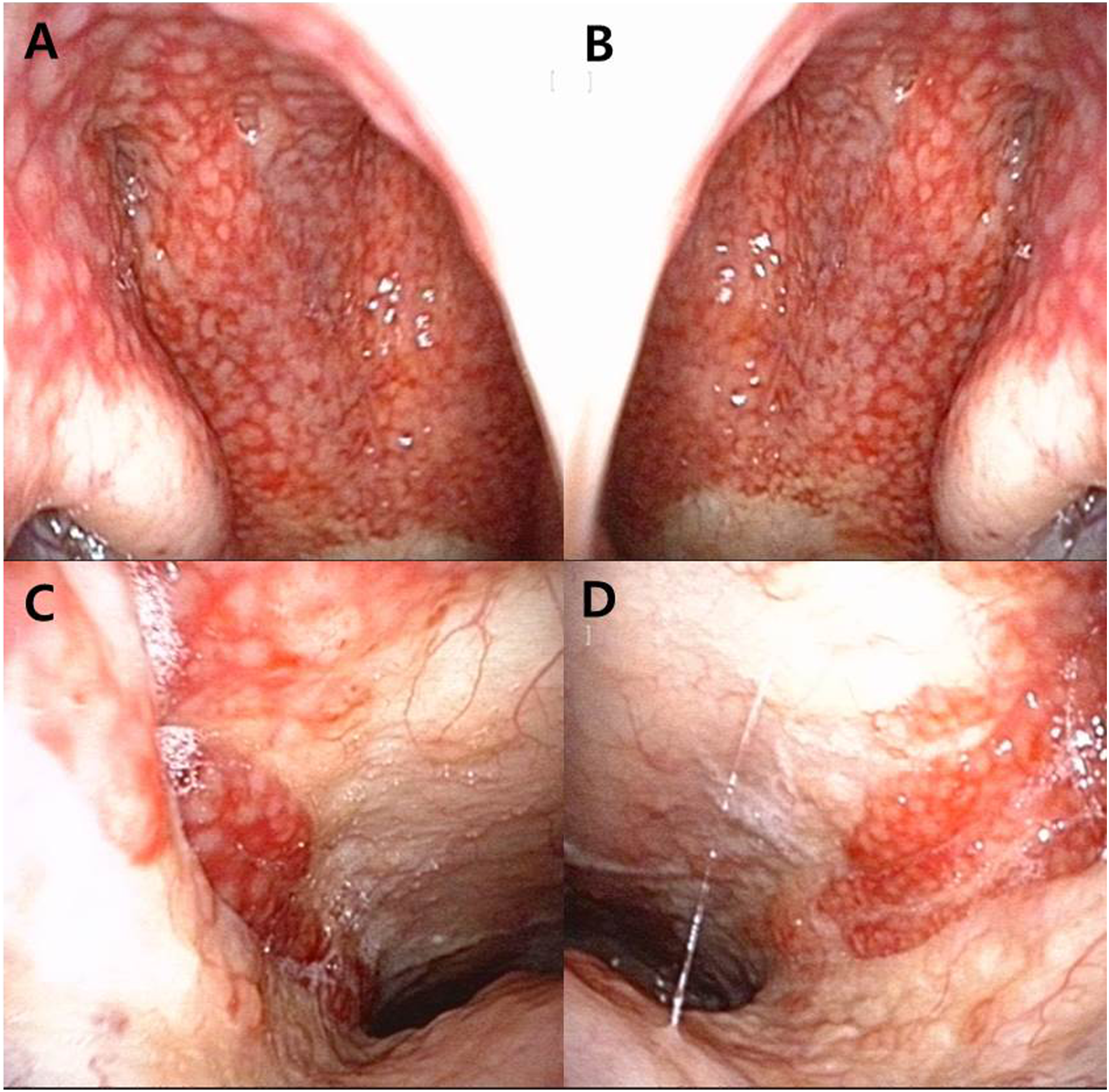
Discussion
Most lymphocytes are found in the lymphatic system, including the lymph nodes in all parts of the body. Transformed B lymphocytes can grow in an uncontrolled way, resulting in the accumulation of lymphoma cells that can cause enlargement of the lymph nodes. Mantle cell lymphoma (MCL) is caused by the malignant transformation of B lymphocytes in the outer edge of a lymph node follicle (the mantle zone). MCL cells can enter the lymphatic channels and blood and spread to other lymph nodes or tissues, such as the spleen, bone marrow, and lymph nodes in the throat (tonsils and adenoids), liver, and gastrointestinal tract. 5 MCL cells can also enter the brain, lungs, and spinal cord, although these are relatively rare. MCL can develop on the mucosa of all parts of the body, typically the pharyngeal Waldeyer’s ring and the GI tract. 5
The GI tract is subdivided into 3 parts, the esophagus, stomach, and intestines (including the duodenum, ileum, cecum, colon, and rectum). MCL lesions in each part of the GI tract can be classified into the following 6 subtypes by endoscopic gross findings 7 : (1) protruded type (solitary or fewer than 10 elevated lesions forming tumorous nodules. These lesions often resemble submucosal tumors and sometimes have accompanying ulcers on their top surfaces), (2) fold-thickening type (thickened mucosal folds like large cerebroid folds, typically seen only in the stomach), (3) multiple micropolyp type (multiple micropolyps with or without some large polyps. The number of polyps is 10 or more), (4) ulcerative type (solitary or multiple shorter lesions due to ulcers), (5) superficial type (changes in mucosal color and/or changes in mucosal morphology), and (6) mixed type (combinations of these 5 subtypes).
However, the subtypes of MCL in the head and neck region have not been classified or reported yet. Most MCLs of the head and neck region develop in the extranodal lymphatic system of Waldeyer’s ring. Within Waldeyer’s ring, the tonsil is the most common location of MCL, followed by the nasopharynx. MCL always presents as a protruding mass type. Because of protruding mass, MCL of Waldeyer’s ring can be easily diagnosed by examining the affected tissue obtained from a surgical biopsy. However, the number of cells obtained from a fine-needle aspiration (FNA) is not sufficient to establish a diagnosis. Sometimes, MCL of Waldeyer’s ring can be associated with necrosis due to angiocentric and polymorphous lymphoreticular infiltrates. These coagulopathies are thought to contribute to hemorrhagic necrosis within the tumor. 1 Different from tonsillar MCL, MCL of the nasopharynx causes diagnostic problems because of the variable features seen in endoscopic findings. When nasopharyngeal MCL is not the protruding type, endoscopic features can present as pseudoinflammatory manifestations, hyperemic injection, or nodular hyperplasia on the pharyngeal mucosa. Physicians can diagnose these lesions as pharyngitis, simple lymphoid hyperplasia, or lymphadenitis. The present case could help distinguish MCL from other nasopharyngeal lesions. In addition, special attention should be paid to evaluating other results of MCL of the nasopharynx, especially the radiologic images.
Conclusion
This was the first case report showing nodular patterns of MCL in the nasopharynx. MCL of the GI tract is classified into several subtypes according to the endoscopic characteristics. However, the subtypes of nasopharyngeal MCL have not yet been classified. Nasopharyngeal MCL should be classified into 2 subtypes, the protruding type and the nodular type. Nodular-type MCL should be recognized and adequately diagnosed because it may have a more aggressive clinical course. A detailed endoscopic evaluation with a thorough whole-body evaluation is essential for an accurate diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by Fund of Biomedical Research Institute of Jeonbuk National University Hospital