
Abstract
Primary nasopharyngeal tuberculosis, defined as an isolated tuberculosis infection of the nasopharynx without systemic or pulmonary disease, is rare, even in areas endemic for tuberculosis. It is challenging for ENT specialists to diagnose primary nasopharyngeal tuberculosis at an early stage. In this report, we describe a new case of primary nasopharyngeal tuberculosis, focusing on its nasopharyngoscopic features and radiological findings that can help the understanding and aid in accurate diagnosis of this unusual disease entity. Our experience suggests that although primary nasopharyngeal tuberculosis is a relatively rare disease, it must be included in the differential diagnosis of various nasopharyngeal lesions, particularly in patients with unusual nasopharyngoscopic and computed tomography findings.
Introduction
Extrapulmonary tuberculosis can be associated with any part of the body and accounts for 15% of newly diagnosed tuberculosis cases worldwide, of which 10% to 35% cases manifest in the head and neck region. 1 Head and neck tuberculosis can arise from most organs in the head and neck region, such as the lymph nodes, larynx, middle ear, oral cavity, and pharynx, in order of frequency.1,2 However, primary nasopharyngeal tuberculosis, defined as an isolated tuberculosis infection of the nasopharynx without systemic or pulmonary disease, is rare, even in areas endemic for tuberculosis.3,4 Previously reported cases of primary nasopharyngeal tuberculosis involved mostly healthy people who had never been exposed to tuberculosis and was slightly more common among young women.5-7 As a broad spectrum of pathologic conditions can occur in the nasopharynx, such as nasopharyngeal cancer and other types of granulomatous disease, careful attention should be paid to make an accurate differential diagnosis based on nasopharyngeal examination findings alone. In general, it is usually necessary to perform biopsies in order to confirm the diagnosis of primary nasopharyngeal tuberculosis. 4
Here, we report a new case of primary nasopharyngeal tuberculosis and a comprehensive review of previously published literature, focusing on its nasopharyngoscopic features and radiological findings that can help the understanding and aid in accurate diagnosis of this unusual lesion.
Case Report
A healthy, 54-year-old Asian woman presented with aural fullness in the right ear for 2 months. She reported no other aural or nasal symptoms and had no relevant medical history. On physical examination, otoscopy of the right ear showed no abnormalities, such as middle ear effusion, but nasopharyngoscopy of the right side using a 0° rigid endoscope revealed that the roof and posterior wall of the nasopharynx and the fossa of Rosenmüller were covered with a thick yellowish discharge that could not be easily removed by suction (Figure 1A). No other abnormalities, such as cervical lymphadenopathy, were observed in other head and neck areas. Routine laboratory tests, including complete blood counts, and chest radiography were unremarkable. Computed tomography (CT; Figure 2) revealed a diffuse enhancing mucosal irregularity with some nonenhancing low-density portions (necrotic portion) in the lateral and posterosuperior walls of the right nasopharynx. This lesion obliterated the right fossa of Rosenmüller and crossed the midline. There was no evidence of bony destruction or intracranial extension. Under local anesthesia, we performed a deep tissue biopsy with the endoscopic transnasal approach. During the biopsy, there was little pain or bleeding. In addition, we found that the thick yellowish, patch-like discharge was necrotic material rather than mucopurulent discharge, which was not easily detached from the lesion (Figure 1B). Histopathological examination showed central caseous necrosis surrounded by granulomatous inflammation and multinucleated giant cells in the granuloma (Figure 3A and B), but acid-fast bacilli stain was negative. However, polymerase chain reaction (PCR) for Mycobacterium tuberculosis (M tuberculosis) was positive. The final diagnosis was primary nasopharyngeal tuberculosis. After the patient was treated using antituberculosis medication with a combination of isoniazid (H), 300 mg, ethambutol (E), 25 mg/kg, rifampicin (R), 10 mg/kg body weight, and pyrazinamide (Z), 2 g (HERZ for 2 months plus HER for 4 months), a nasopharyngoscopy showed no significant abnormalities (Figure 1C).
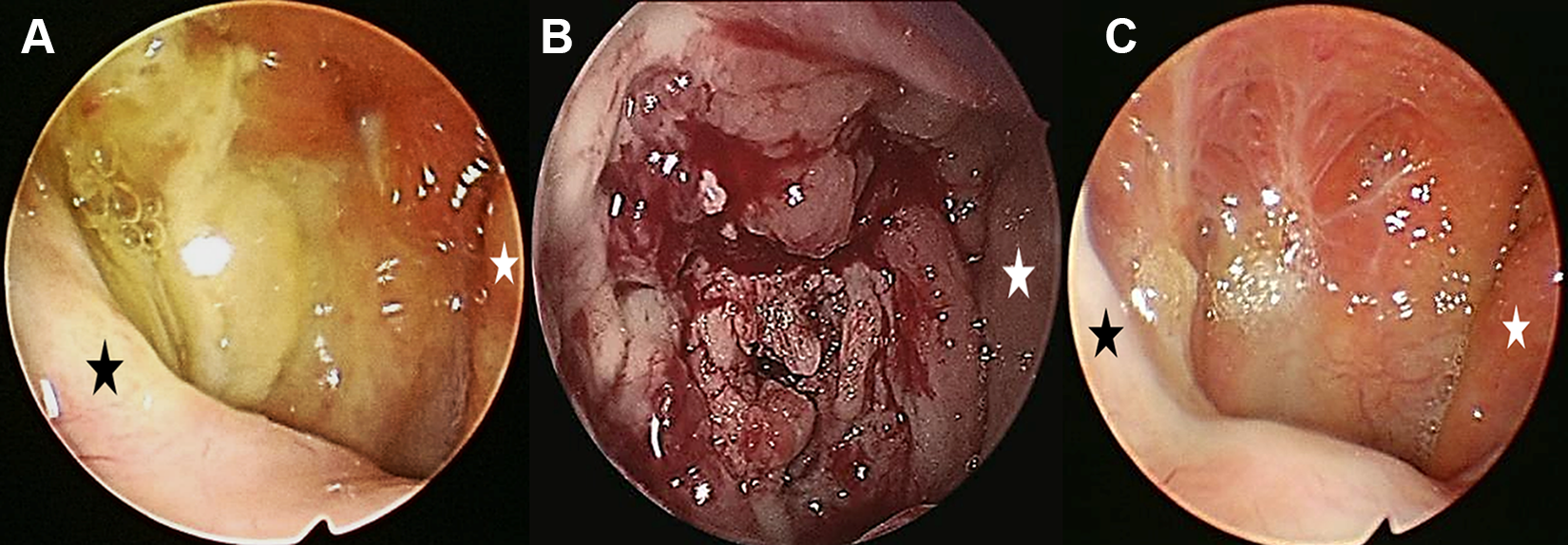
(A and B) The right nasopharyngoscopic view reveals that the fossa of Rosenmüller and the roof and posterior walls of the nasopharynx are covered with a thick yellowish discharge that cannot be easily removed with suction. (C) The nasopharyngoscopic view is nearly normal 6 months after treatment (black asterisk, right salpingopharyngeal fold; white asterisk, left salpingopharyngeal fold; A, initial visit; B, before deep biopsy).
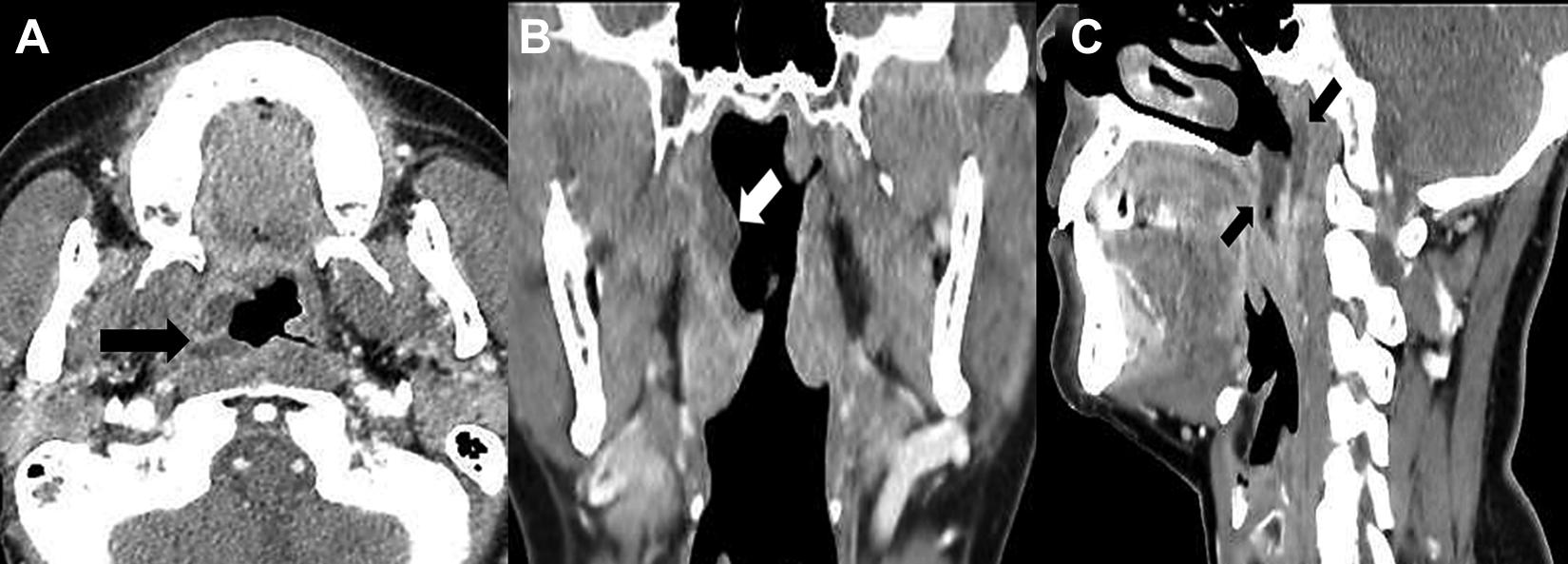
The paranasal sinus computed tomography scan reveals a diffuse enhancing mucosal irregularity with some nonenhancing low-density portions (necrotic portion, black and white arrows) in the lateral and posterosuperior walls of the right nasopharynx (A, axial view; B, coronal view; C, sagittal view).
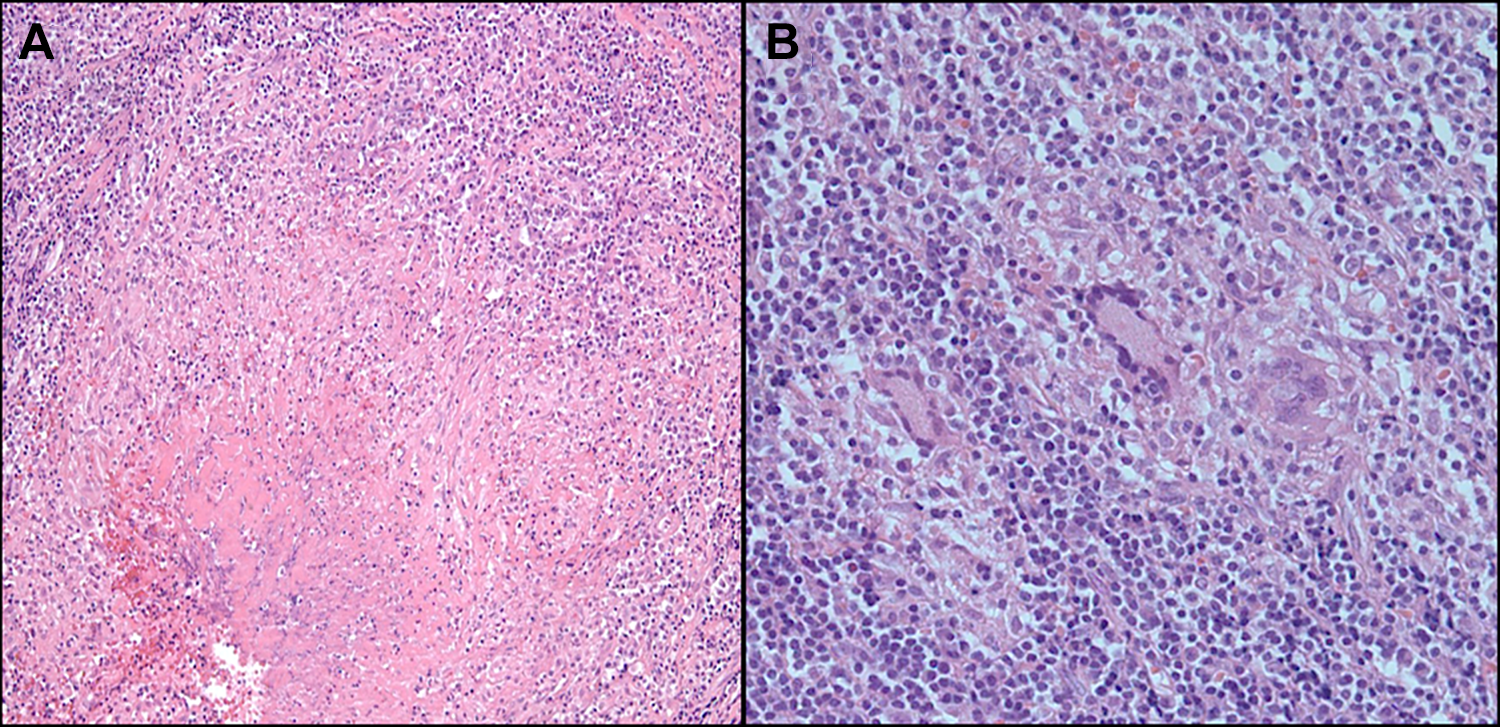
(A and B) Histopathologic images show central caseous necrosis surrounded by granulomatous inflammation and multinucleated giant cells in the granuloma (A, original magnification, ×100; B, original magnification, ×400).
Discussion
It is challenging for ENT specialists to diagnose primary nasopharyngeal tuberculosis at an early stage, as it has varying nonspecific clinical presentations.6,8 The common symptoms of primary nasopharyngeal tuberculosis are cervical lymphadenopathy, otologic discomforts (ear fullness, hearing impairment, and otitis media), and nasal symptoms (nasal obstruction, epistaxis, and postnasal drip).4,8,9
The nasopharynx may be infected with M tuberculosis via 2 routes. 4 In primary nasopharyngeal tuberculosis, the infection occurs directly through nasal ventilation. As a secondary route, nasopharyngeal tuberculosis can occur as an adjacent infection from another primary site, most often pulmonary tuberculosis through the airways, blood vessels, or lymphatic networks. 4
The possible nasopharyngoscopic findings include (1) normal appearance; (2) irregular mucosa or ulcerative lesions; (3) a mass, bulging, or swelling; and (4) white patches covering the nasopharyngeal area. Among these nasopharyngoscopic findings, the nasopharyngeal mass seen in the proliferative phase may cause bulging of the wall, while the mucosal irregularity or thickening with ulceration observed in the exfoliative phase may make differentiating primary nasopharyngeal tuberculosis from nasopharyngeal cancer difficult.6,10
In the present case, nasopharyngoscopic findings from the deep tissue biopsy were unusual, as the nasopharynx was covered with a yellowish, thick patch-like discharge, which was actually necrotic tissue that could not be easily removed with suction. This nasopharyngoscopic finding might be considered as the middle phase between the mass-like lesion and the ulcerative lesion. In addition, the necrotic tissue may be caseous necrosis, a unique form of cell death in which the tissue maintains a cheese-like appearance.
The diagnosis of primary nasopharyngeal tuberculosis is made by histopathologic and microbiologic findings from a biopsy sample. 10 Although the common CT and magnetic resonance imaging (MRI) finding in primary nasopharyngeal tuberculosis is a polypoid mass, followed by diffuse mucosal thickening, 6 CT or MRI is not sufficient for the diagnosis of primary nasopharyngeal tuberculosis. 11 However, a small nasopharyngeal lesion with necrosis on imaging studies might be a valuable clue to the diagnosis of nasopharyngeal tuberculosis, as this small necrosis in the nasopharynx may be caseous necrosis on pathological study. 6 Even in the present case, CT revealed a diffuse enhancing mucosal irregularity with some nonenhancing low-density portions (necrotic portion) in the lateral and posterosuperior walls of the right nasopharynx, suggesting tuberculosis.
Pathologic examination revealed granulomatous inflammation with epithelioid giant cells and caseous necrosis. Acid-fast bacilli could be found and the culture isolates of M tuberculosis. 10 Although a granulomatous reaction is frequently observed, the isolation of acid-fast bacilli and a culture of M tuberculosis can be extremely difficult. 10 However, PCR amplification with tissue specimens is useful for detecting M tuberculosis DNA and can be used to increase the diagnostic accuracy in patients who have perplexing diagnostic difficulties associated with a granulomatous tissue response. 12
Recently, tuberculosis has become a global public health crisis due to an increasing number of drug-resistant cases. Therefore, early effective treatment is important to prevent the emergence of drug-resistant strains. This requires a fast and reliable diagnostic method for effective case management. 13 The methods commonly used to screen and diagnose tuberculosis are clinical, immunological (interferon γ release assay), microscopy, radiography, and bacterial culture. 13 In addition, molecular diagnostic methods to diagnose and characterize tuberculosis, including MTBDRplus (M tuberculosis and drug resistance), loop-mediated isothermal amplification, line-probe assay, GeneXpert, and whole-genome sequencing have recently been developed and are now available for the simultaneous identification of M tuberculosis and mutation(s) associated with routinely used antituberculosis drugs. 13
Although nasopharyngeal cancer is the most important differential diagnosis owing to its similar clinical presentations, primary nasopharyngeal tuberculosis requires differentiation from various diseases, including fungal infection (aspergillosis, mucormycosis), granulomatous inflammation (sarcoidosis, leprosy, syphilis, midline lethal granuloma), and autoimmune disease (polyarteritis nodosa, Churg-Strauss syndrome, and Wegener granulomatosis). 7
The treatment for extrapulmonary tuberculosis, including primary nasopharyngeal tuberculosis, is the same as that for pulmonary tuberculosis. Primary nasopharyngeal tuberculosis has good prognosis after a well-performed antituberculosis treatment for a sufficient period. 4 In South Korea, the minimal duration of antituberculosis treatment for nasopharyngeal tuberculosis is 6 months (HERZ for 2 months plus HER for 4 months). 8
Conclusion
It is challenging for ENT specialists to diagnose primary nasopharyngeal tuberculosis at an early stage. Here, we report an additional, new case of primary nasopharyngeal tuberculosis, focusing on its nasopharyngoscopic features and radiological findings that can help the understanding and aid in accurate diagnosis of this unusual disease entity. Our experience suggests that although primary nasopharyngeal tuberculosis is relatively rare, it must be included in the differential diagnosis of various nasopharyngeal lesions, particularly in patients with unusual nasopharyngoscopic and CT findings.
Footnotes
Authors’ Note
The patient’s permission was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.