
Abstract
The occurrence of ectopic intrathyroidal parathyroid adenoma (EPTA) is very rare, which causes some difficulties in diagnosis and complicates treatment. In addition, the occurrence of EPTA with nodular goiter (NG) is rare, which makes diagnosis difficult and requires the assistance of clinical evidence, imaging data, and cytological examination results. Therefore, we present a patient with a final diagnosis of ETPA with NG.
Keywords
Introduction
Primary hyperparathyroidism (PHPT) is an endocrine disease mainly caused by parathyroid adenoma (PA), hyperplasia, or adenocarcinoma. However, PA is the main cause of primary hyperparathyroidism and mostly occurs in isolation. Its main clinical symptoms include hypercalcemia, and the parathyroid hormone (PTH) level is elevated or abnormal. PA originates from clonal expansion of tumor cells, which may be located in the posterior lobe or ectopic site of the thyroid gland. In clinical practice, ectopic intrathyroidal parathyroid adenoma (ETPA) with nodular goiter (NG) is rarely seen. For this rare case, surgical resection is the only effective method. When ultrasound, 99mTc-MIBI SPECT/CT and fine needle aspiration biopsy (FNAB) cannot be used to distinguish the nature of this type of thyroid lesion, and 18F-fluorocholine (18F-FCH) PET/CT may be helpful in diagnosis, achieving the best therapeutic effect, providing the best patient care, and avoiding misdiagnosis and reoperation.
Case Presentation
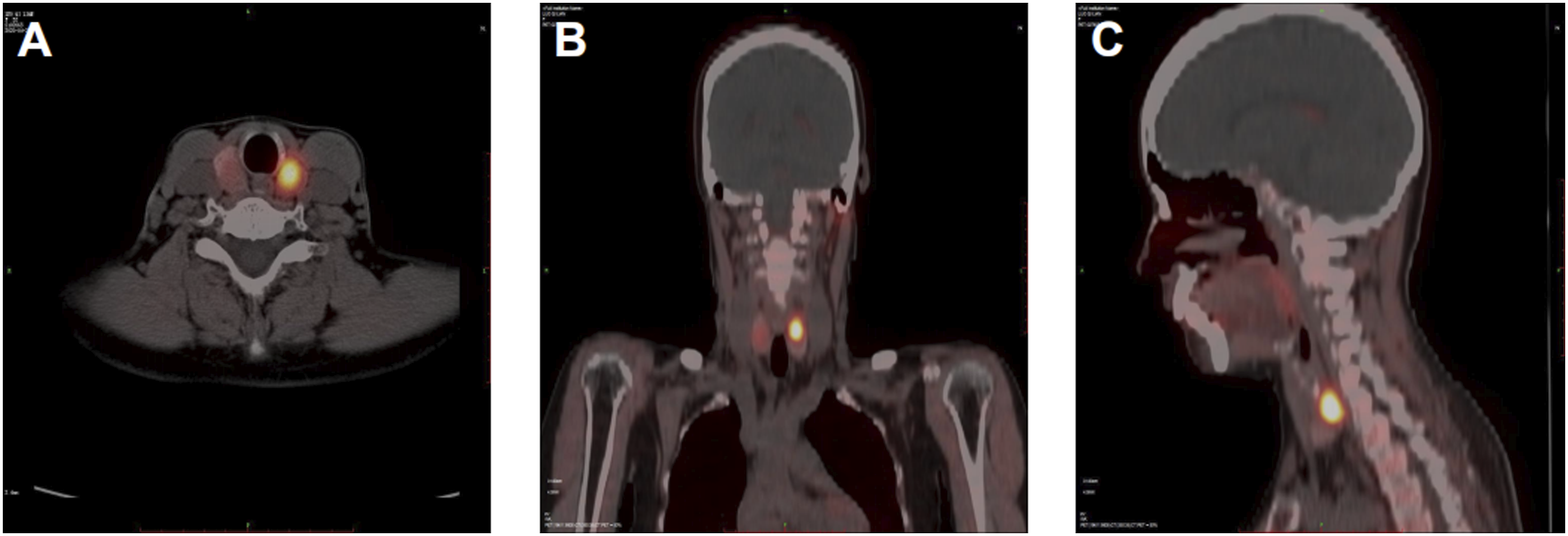
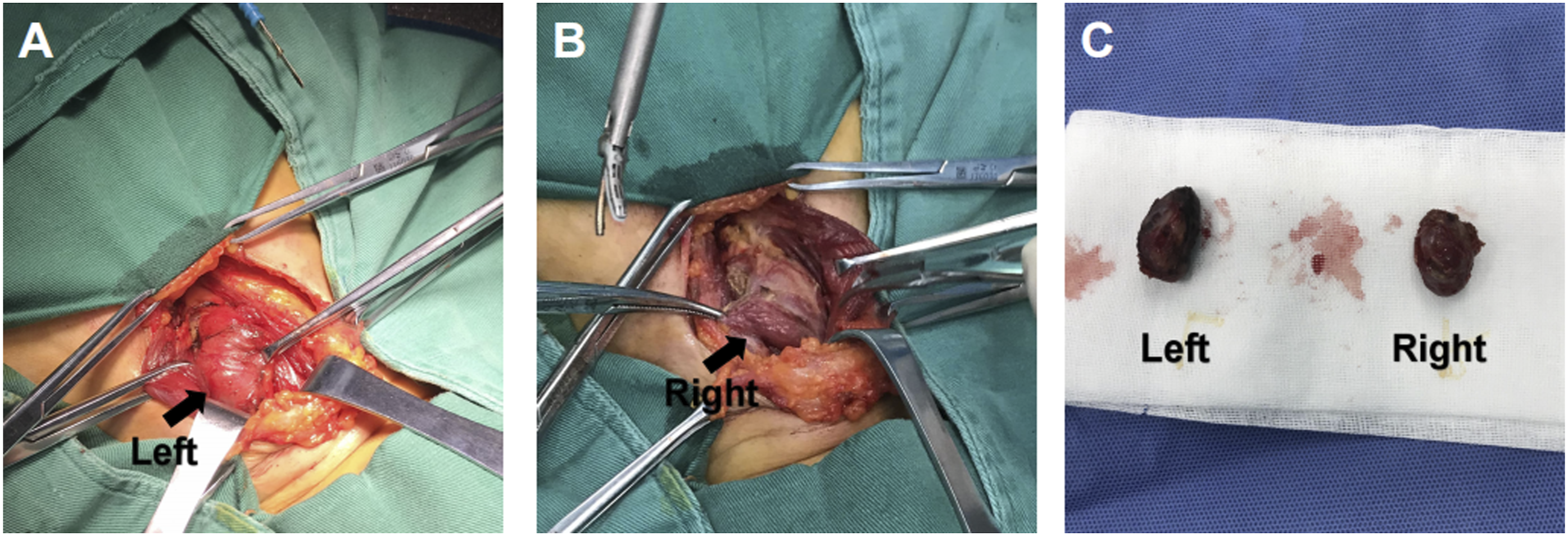
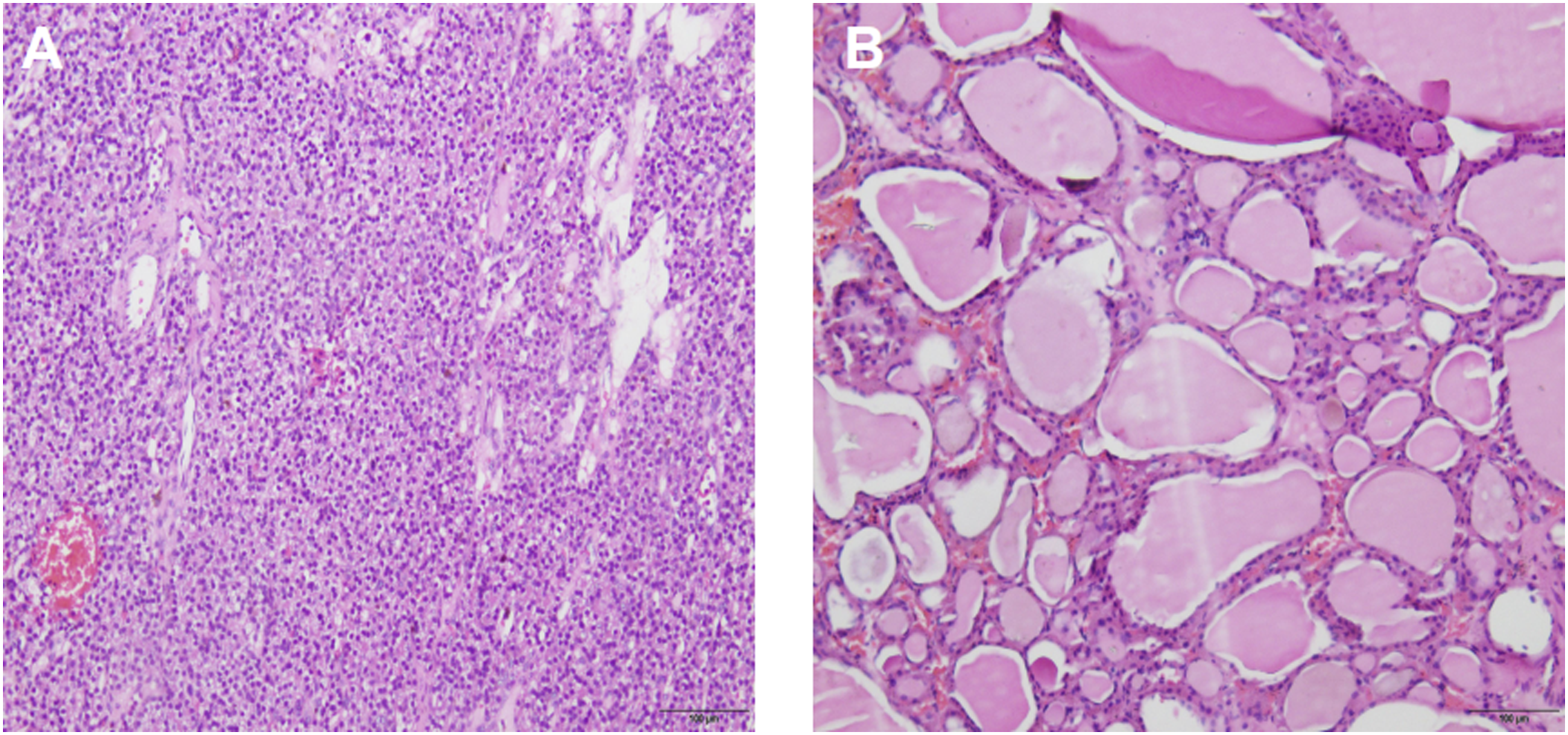
A 52-year-old woman was admitted to the thyroid surgery department of the Affiliated Hospital of Southwest Medical University for 9 days of thyroid occupation. She had a history of bone pain and underwent a right hip replacement for right femoral head avascular necrosis 15 days prior. Her serum free calcium level was 3.38 (normal range: 2.11–2.52 mmol/L), her parathyroid hormone (PTH) level was 734.89 pg/ml (normal range: 8.7–79.6 Pg/ml), and the thyroid function was normal. Ultrasonography showed that the left lobe of the thyroid gland had a weak echo of approximately 2.8 × 1.2 × 1.1 cm in size, regular shape and clear boundary, and the right lobe of the thyroid gland had echo clusters of approximately 2.24 × 1.64 × 1.17 cm in size, regular shape, and clear boundary. 99mTc-MIBI SPECT/CT showed that there was a slightly low-density tissue nodule shadow of approximately 2 cm on both sides of the thyroid gland, with a clear boundary. Tumor lesions were possibly present on both sides of the nodule, and no abnormal soft tissue density shadows or imaging agent concentration shadows were found in the rest of the neck (Figure 1). Fine needle aspiration biopsy (FNAB) showed that adenomatous changes were possible in bilateral intrathyroid nodules. To further clarify the diagnosis, we used 18F-fluorocholine (18F-FCH) PET/CT imaging. The results showed that the level of imaging agent uptake in the bilateral thyroid nodules increased, and the level of imaging agent uptake of left lobe nodules was more significant than that of lateral thyroid nodules. Parathyroid tissue was assessed in the left thyroid (Figure 2). After the operation, dark red nodules with a size of approximately 2 × 1 × 1 cm could be seen on both sides of the thyroid, which were relatively soft and clearly demarcated from the surrounding tissues (Figure 3). The intraoperative frozen examination showed that benign lesions were possible in the right intralobular nodule of the thyroid gland, and parathyroid adenoma was possibly present in the left intralobular nodule of the thyroid gland. Therefore, we performed left parathyroid adenoma resection, right partial thyroidectomy, bilateral recurrent laryngeal nerve, and parathyroid exploration. PTH levels were detected during the operation. The PTH level decreased to 158.02 pg/ml (normal range: 8.7–79.6 pg/ml) in 15 minutes and decreased to 100.26 pg/ml (normal range: 8.7–79.6 pg/ml) in 30 minutes after parathyroidectomy. The PTH level returned to normal on the 7th day after the operation, and the patient developed transient perioral dermatitis, limb numbness, and other symptoms after the operation. After being treated with calcium supplements (oral calcitriol and calcium carbonate), the symptoms were relieved rapidly, and the serum free calcium level recovered to 2.29 mmol/L (normal range: 2.11–2.52 mmol/L) on the third day after the operation. The postoperative pathological report showed that the left intralobular nodule of the thyroid was considered parathyroid tissue with adenomatous hyperplasia, and the right intralobular nodule of the thyroid was considered NG (Figure 4). (a) The nodular concentration of 99mTc-MIBI imaging agent can be seen in bilateral thyroid lobes in 15 minutes. (b) The nodular concentration of 99mTc-MIBI imaging agent appearance of bilateral thyroid lobes disappeared in 120 minutes. (a-c) In transverse, coronal, and sagittal 18F-FCH PET/CT imaging, low-density soft tissue nodular shadow in bilateral thyroid lobes can be seen, and the uptake of left nodular imaging agent is more significant than that in the opposite. (a-c) The dark red nodules were found in the bilateral lobes of the thyroid gland during the operation (black arrow), which were soft and about 2 × 1 × 1 cm in size. (a) The pathological specimen confirms that parathyroid adenoma was found in the left lobe of thyroid gland. (b) The pathological specimen confirms that NG in the right lobe of thyroid.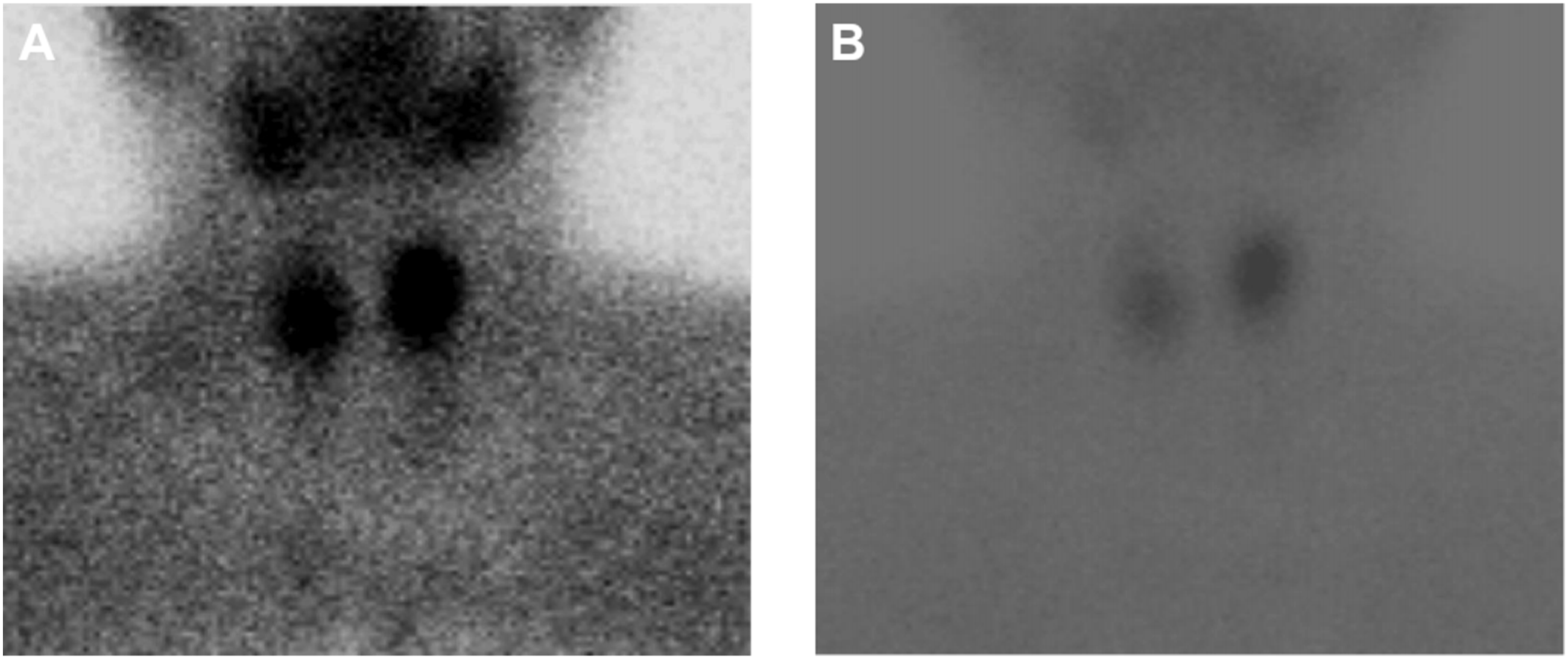
Discussion
In embryology and anatomy, the parathyroid gland originates from the endoderm of the pharyngeal sac in all vertebrate animals. 1 Parathyroid glands are generally divided into two pairs with four in total, attached to the middle or lower part of the back of the left and right lobes of the thyroid gland, which are oval and flat and red, brown, or light yellow. The position of the upper parathyroid glands is relatively constant, usually located in the middle of the posterior margin of the thyroid gland (where the superior thyroid artery enters the gland or intersects with the recurrent laryngeal nerve). In a few cases, the parathyroid gland can move backward and laterally and can be located in the posterior pharyngeal or esophageal space. 2 The lower parathyroid glands originate from the third parotid sac complex and are accompanied by the thymus. As the tail of the complex descends, it is separated from the thymus. Their positions are not constant; most of them are located in the front or rear of the inferior pole of the thyroid, some of them are kept in the thymus at the entrance of the thorax, and a few of them enter the mediastinum with a decrease in the thymus gland or their early development is blocked. Therefore, the parathyroid gland can be found anywhere from the mandibular angle to the pericardium.3,4 In the early stage of thyroid development, parathyroid glands can also descend to the thyroid gland lobe and become a part of the thyroid gland lobe. Lappas D et al. found 3796 parathyroids in 942 autopsies; 8.5% of them had heterotopia, and 0.2% of them were located in the thyroid gland, indicating the rare degree of EPTA. 5 Moreover, NG is a diffuse or nodular enlargement of the thyroid associated with normal thyroid function, which does not result in a neoplastic or inflammatory process. Goiters may occur endemically, mainly due to iodine deficiency, or they can occur sporadically. 6 There is no genetic relationship between PA and NG. The coexistence of PA and NG is rare, and experience in clinical diagnosis and treatment of this condition is relatively scarce.
The qualitative diagnosis of primary hyperparathyroidism (PHPT) mainly depends on the clinical manifestations and the determination of blood calcium, phosphorus, and PTH concentrations; the diagnosis of its location mainly depends on imaging examinations, such as ultrasound, 99mTc-MIBI SPECT/CT, and 18F-FCH PET/CT. However, identifying the accurate location is the key to the success of the operation. When PA and NG exist together, it is difficult to distinguish them morphologically, and the rates of misdiagnosis and missed diagnosis are especially high. For the diagnosis of thyroid nodules, ultrasound is the preferred method for identifying anatomical location. The ultrasound manifestations of NG are usually oval low echo, clear boundary, lack of halo, and calcification, and cystic change can be seen inside, while the ultrasound manifestations of PA are usually oval or oval low echo, clear boundary, regular edge, bleeding, and necrosis cystic change. 7 In this case, the ultrasound phenotype of bilateral intrathyroid nodules was similar, and the nature of the nodules could not be distinguished. Therefore, ultrasound has certain defects in this kind of patient. However, there are also studies on EPTA ultrasound images, and the results show that there is a hyperechoic line on the ventral surface of the parathyroid gland, which is the most distinctive feature of this kind of hyperechoic line that can still be found in PA with small volume and no obvious blood flow signal, 7 which may be helpful for the diagnosis of EPTA. 99mTc-MIBI SPECT/CT may have more advantages in the evaluation of PA than those that ultrasound can provide. It can be used to estimate the function of the parathyroid gland and the extent of its hyperplasia. It is the simplest and most widely used noninvasive method for preoperative determination of the localization and diagnosis of PHPT lesions. 8 However, 99mTc-MIBI SPECT/CT also has some defects, for example, when parathyroid hyperplasia is not obvious, the focus is too small to be covered by thyroid tissue, or in this case, to identify NG and ETPA, and false negative results may appear. In this case, 99mTc-MIBI SPECT/CT identified a slightly low-density tissue nodular shadow on both sides of the thyroid gland, suggesting tumor lesions, but its nature could not be determined. FNAB has been widely used in the differential diagnosis of benign and malignant thyroid nodules to determine whether surgery is needed. At the same time, it can also be used in the differential diagnosis of benign thyroid diseases. 9 Next, we performed FNAB on the patient to further clarify the nature of the bilateral intrathyroid nodules. FNAB results showed that bilateral intrathyroid nodules were adenomatous changes, but their specific nature was still unclear. Some studies have shown that 18F-FCH PET/CT is more sensitive and accurate than ultrasound, 99mTc-MIBI SPECT/CT and FNAB in the diagnosis of PA, and its use in preoperative diagnosis is better. 10 It is a PET tracer that can be used to evaluate the turnover of the cell membrane. It is generally used in the imaging examination of prostate cancer and determination of the localization of hyperparathyroidism. 11 Therefore, when ultrasound, 99mTc-MIBI SPECT/CT and FNAB cannot determine the nature of intrathyroid nodules; 18F-FCH PET/CT may be a better choice. The 18F-FCH PET/CT method showed that the level of imaging agent uptake in the bilateral thyroid nodules increased, and the level of imaging agent uptake in the left lobe nodules was more significant than that of lateral thyroid nodules. The left intrathyroid nodules were considered parathyroid tissue, and the right intrathyroid nodules were considered NG. According to the literature, there is no research on 18f-FCH PET/CT recognition of NG and ETPA. It is speculated that 18F-FCH PET/CT may be a potential method to identify NG and ETPA.
At present, PHPT is still mainly treated by surgery. Generally, the lower neck collar is selected as the site of surgical incision, which is mainly convenient to explore the superior and inferior thyroid glands or ectopic tumors, cancer, etc. The scope of resection is as follows: parathyroid adenoma should be excised only, 3 or 3½ glands should be excised for hyperparathyroidism, and if parathyroid carcinoma is present, the surrounding tissue should be excised as a whole. At present, the treatment of nodular goiter is also mainly based on surgery, including NG resection, subtotal thyroidectomy, partial thyroidectomy, and total thyroidectomy, which is mainly based on the number of NG, severity, location, and patient age to implement the individualized treatment plan. At present, subtotal thyroidectomy and total thyroidectomy are preferred. According to the patient’s intraoperative exploration and preoperative examination results, left parathyroid adenoma resection and right partial thyroidectomy were performed. It is still controversial whether parathyroid exploration should be carried out unilaterally or bilaterally after PA resection. Some studies have detected PTH levels in the blood of PHPT patients 15 and 30 minutes after PA resection and found that PTH levels can be reduced by more than 50% within 10 minutes after PA resection. The lowest level can be reached within 1–3 hours after operation, and the normal level can be recovered within 40 hours. The PTH level of the vast majority of patients decreased significantly 10 minutes after focal resection. If the exploratory operation continues and stimulates other parathyroid glands, the timing of the significant decrease in PTH level can be delayed to 20–30 minutes. If the PTH level decreases by more than 50% during the operation, only one-sided exploration can be performed. If there is no significant decrease or increase after the partial decrease, bilateral exploration can be performed.12,13 In this case, the PTH level decreased by 78.5% 15 minutes after the operation, so unilateral exploration of the parathyroid was considered. Hypocalcemia (perioral numbness and tetany) is a common complication of hyperparathyroidism. Because hypocalcemia after surgery for hyperparathyroidism is mostly temporary, it can be relieved by active calcium and VitD. If hypocalcemia cannot be recovered for a long time, this suggests that there may be permanent hypoparathyroidism, so parathyroid transplantation should be considered to correct hypocalcemia.
Conclusion
It is very rare that EPTA and NG occur at the same time. If symptoms of HPT, such as unexplained lumbago and leg pain, spontaneous fracture, urinary calculi, and peptic ulcer, are found, we should be alert to the presence of PA and carry out the detection of serum PTH, blood calcium, and blood phosphorus levels, as well as an imaging examination. When the nature of the thyroid intranodule cannot be determined by ultrasound, 99mTc-MIBI SPECT/CT and FNAB,18F-FCH PET/CT may be helpful for our diagnosis to prevent misdiagnosis and secondary operation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Scientific Research Fund of Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University (2021ZKQN116).