
Abstract
The occurrence of parathyroid carcinoma (PC) is rare, which can lead to difficulties in diagnosis and complicate treatment. However, synchronous PC and breast carcinoma (BC) are rarer, which makes diagnosis and development of a treatment plan more difficult and requires the assistance of clinical evidence, imaging data, and histological examination results. This case report presents a patient with a final diagnosis of synchronous PC and BC.
Introduction
Parathyroid carcinoma (PC) is a rare malignant tumor, and approximately 90% of parathyroid cancers have hormone secretion functions, which can lead to the secretion of parathyroid hormone (PTH). PC accounts for approximately 1% of patients with primary hyperparathyroidism. 1 Therefore, most patients visit the hospital only after presenting obvious symptoms related to hypercalcemia or metabolic bone disease. PC is challenging because of its hidden onset, relatively-difficult diagnosis and treatment, and high postoperative recurrence rate. Breast carcinoma (BC) is one of the most common malignant tumors in women, and the overall prognosis of patients with BC can be improved through comprehensive treatment, such as surgery, chemotherapy, radiotherapy, and targeted therapy. 2 However, when BC co-occurs with other diseases, especially other malignant tumors, its treatment strategy and sequence become the focus and difficulty of treatment. PC has no specific tumor markers, and it is difficult to diagnose via preoperative imaging or even cytological examination. In addition, it is difficult to distinguish the specific properties of PC via preoperative examination in clinical practice. 1 The present case report describes a patient with PC with co-occurring BC to improve awareness and diagnosis of this type of disease.
Case Presentation
Written informed consent was obtained from the patient to publish this case report. The ethics committee waived informed consent for the study.
A 47-year-old female patient was admitted to the hospital after a mass in her left breast was discovered 1 month earlier. A relevant auxiliary examination was completed after admission. Thyroid ultrasonography revealed a low echo of approximately 13.0 mm × 16.8 mm × 9.1 mm in the right lobe of the thyroid gland, and the TI-RADS classification was 4a (Figure 1). Neck computed tomography (CT) revealed a low-density nodule in the right inferior lobe of the thyroid, with an unclear relationship to the thyroid (Figure 2). The patient underwent a coarse needle biopsy of the left breast mass and a fine needle biopsy of the hypoechoic nodule of the right lobe of the thyroid. Clinicopathological analysis confirmed that the left breast mass biopsy tissue infiltrated the ductal carcinoma, and the immunohistochemical labeling results revealed the following: ER (−), PR (−), AR (−), HER2 (−), and Ki67 (+60%). The puncture histological results of the hypoechoic tubercle of the right lobe of the thyroid indicated that there was no definite papillary carcinoma and that BC metastasis could not be ruled out. Other examinations of the patient were needed to exclude distant metastasis. Single-photon emission computed tomography-computed tomography (SPECT-CT) multiprobe whole-body bone imaging + organ tomography imaging suggested that whole-body bone symmetry and diffuse imaging agent uptake increased. The whole-body bone imaging was consistent with metabolic bone disease. The bone mineral density examination suggested decreased bone mass (T = −1.3). The serum calcium level was 2.91 mmol/L (normal reference range: 2.11-2.52 mmol/L), and the serum alkaline phosphatase (ALP) level was 106 U/L (normal reference range: 35-100 U/L). Other auxiliary results did not indicate obvious exceptions. In conjunction with the relevant auxiliary examination, the possibility of left breast malignancy with thyroid and bone metastases could not be ruled out. Given that no evidence of metastasis was found in the remaining important organs of the patient’s body and that the overall survival time was expected to be longer, after communication with the patient, total left breast resection and sentinel lymph node biopsy was performed under general anesthesia on October 10, 2022. Rapid intraoperative biopsy revealed no cancer metastasis in the sentinel lymph nodes. Postoperative pathological results revealed invasive ductal carcinoma of the left breast (WHO grade III) with high-grade intraductal carcinoma and lobular carcinoma (Figure 2). The patient was eventually diagnosed with triple-negative left breast nonspecific invasive ductal carcinoma, pT1cN0Mx, stage Ia. After surgery, a doxorubicin hydrochloride liposome injection (35 mg/m2) + cyclophosphamide (600 mg/m2) followed by an albumin-paclitaxel (260 mg/m2) chemotherapy regimen was administered every 21 days, with 8 cycles of chemotherapy. The patient tolerated the chemotherapy process well, and the serum calcium level was monitored at admission to the hospital during each cycle of chemotherapy. There were no significant changes in the right lobe of the thyroid space observed at admission during each cycle. After the end of the 8th chemotherapy regimen, the serum calcium level of the patients was measured again at 2.85 mmol/L, and the serum ALP level was 130 U/L.
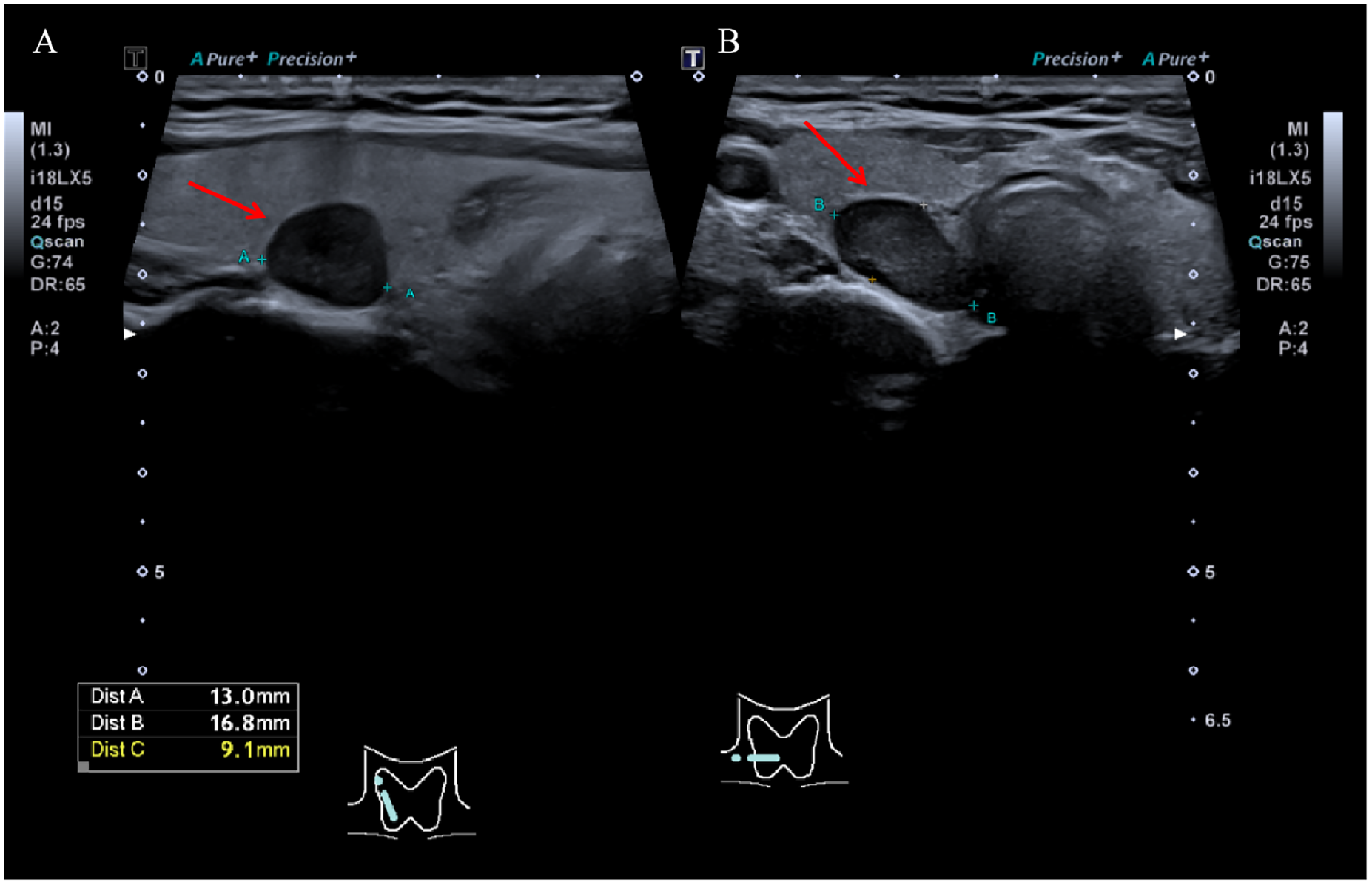
(A) The thyroid ultrasound showed the longitudinal section of the hypoechoic tubercle in the middle lobe of the right thyroid gland. (B) Thyroid ultrasound showed the transverse section of the hypoechoic tubercle in the middle lobe of the right thyroid. The red arrow indicates a suspected abnormal parathyroid area.
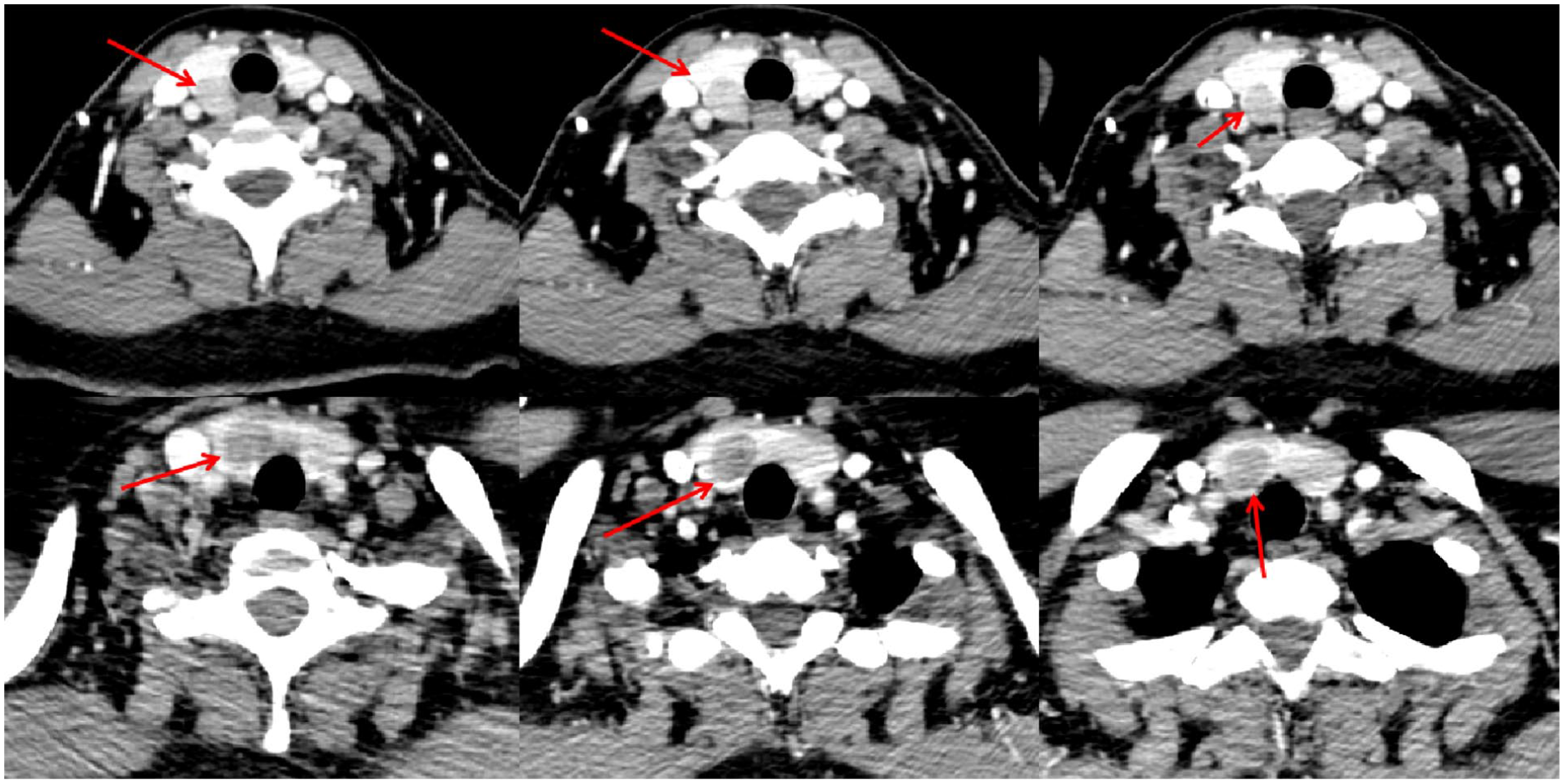
CT images of the neck after 20 minutes injection of iodohexol. Red arrows indicate suspected abnormal parathyroid glands. CT, computed tomography.
After the end of chemotherapy, the above indices did not improve. Measurement of the serum PTH level of the patient indicated a level of 68.3 pmol/L (normal reference range: 1.27-9.33 pmol/L). Continued parathyroid ultrasonography revealed a low echo of 15.1 × 13.8 × 11.0 mm in the dorsal part of the right lobe of the thyroid gland, which was closely related to the thyroid tissue, and this low echo nodule was considered a parathyroid adenoma. Neck-enhanced CT revealed a reduction in nodular density in the right lobe of the thyroid, with a maximum diameter of approximately 1.5 cm. An elliptical enhanced shadow was observed behind the right lobe, and the boundary with the right lobe was not clear, with a maximum diameter of approximately 1.6 cm. Multiprobe SPECT-CT parathyroid dual-phase imaging plus organ tomography revealed that in the initial phase, the 2 lobes of the thyroid clearly developed, the position and shape were normal, and the radioactivity distribution was uneven. The upper part of the right lobe of the thyroid was observed with a speckled developer shadow, and the radioactivity level was similar to that of the myocardial image (Figure 3A). In the delayed phase, the degree of radioactive activity was lower than that of the myocardial shadow, and the speckled developer concentration shadow was observed in the upper part of the right lobe of the thyroid (Figure 3B). In summary, considering the concentrated shadow of speckled radioactivity in the upper part of the right lobe of the thyroid, the possibility of hyperparathyroidism was considered high, and resection of the right superior parathyroid gland plus rapid intraoperative pathological biopsy was performed on March 1, 2023. During the operation, the right superior parathyroid gland clearly invaded the right lobe of the thyroid gland, which was difficult to separate (Figure 4). Therefore, the increased surgical scope involved excision of the right lobe and isthmus of the thyroid plus excision of the right upper parathyroid. Intraoperative frozen biopsy revealed a nodular goiter in the right lobe and isthmus of the thyroid. Another parathyroid tumor (6 cm × 1.5 cm × 1.2 cm in size) was found in the sent tissue. The envelope of the parathyroid tumor was suspected to be invaded, and extensive paraffin section observation was necessary to determine whether it was parathyroid cancer. PTH detection 15 minutes after the lesion left the body revealed that the PTH level was 4.21 pmol/L. Considering that parathyroid malignancy may be large, combined with intraoperative conditions and rapid intraoperative pathological biopsy results, the operation was concluded after the dissection of the right neck VI lymph node. The postoperative pathologic findings confirmed that the nodule was a PC (Figure 5A). After surgery, the main diagnoses were as follows: (1) triple-negative left nonspecific invasive BC, pT1cN0M0, stage Ia; (2) right upper PC; and (3) primary hyperparathyroidism. Capecitabine 650 mg/m2 bid po was continued for 1 year after surgery to treat the BC. At the 17th month after the parathyroid surgery, there was no evidence of recurrence or metastasis in the whole-body, and the serum PTH, calcium ion, and ferritin levels were within the normal range.
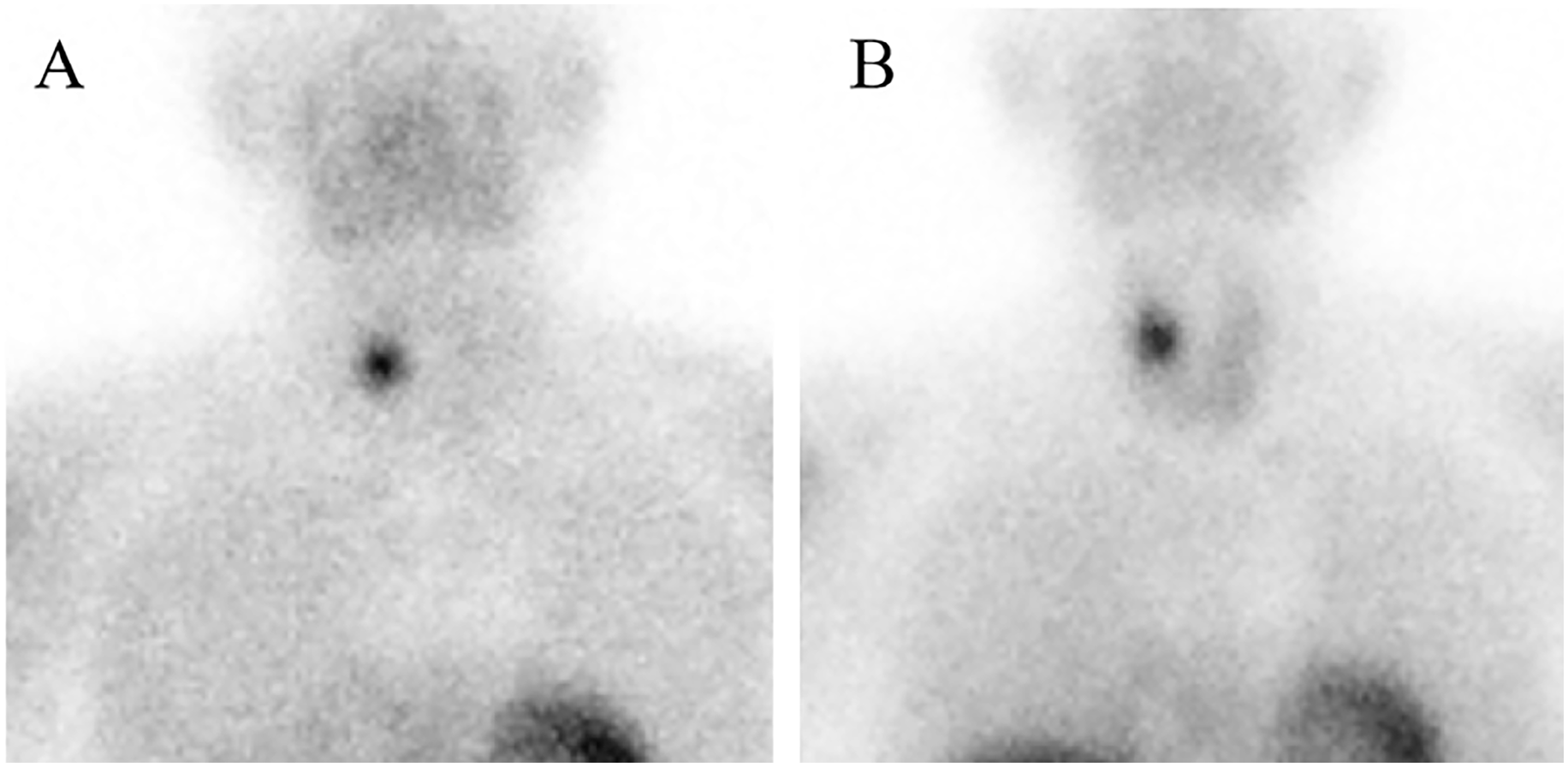
(A) Parathyroid imaging and organ tomography were performed 15 minutes after intravenous injection of Tc-99m-MIBI 10 mCi. (B) Parathyroid imaging and organ tomography were performed 2 hours after intravenous injection of Tc-99m-MIBI 10 mCi.
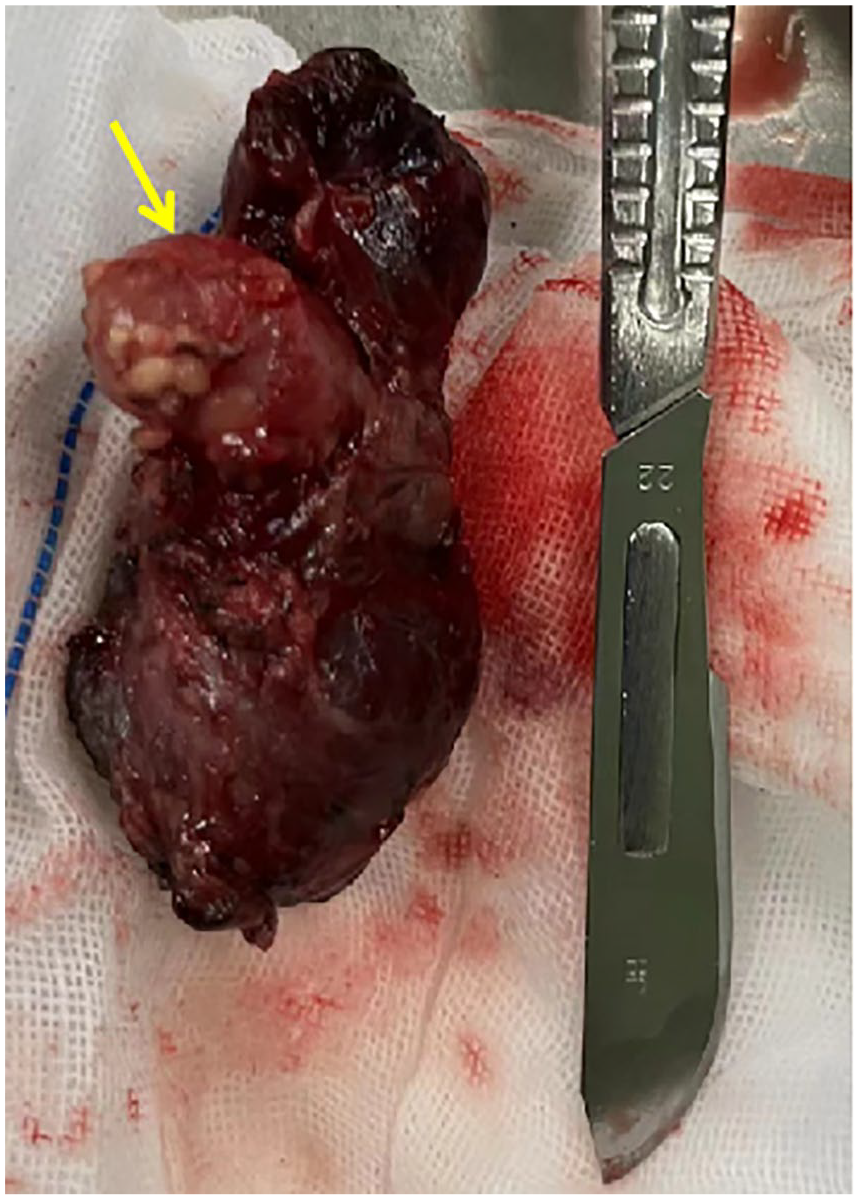
Surgeon completely removed the right lobe and isthmus of the thyroid gland and the abnormal parathyroid gland located in its middle and back.
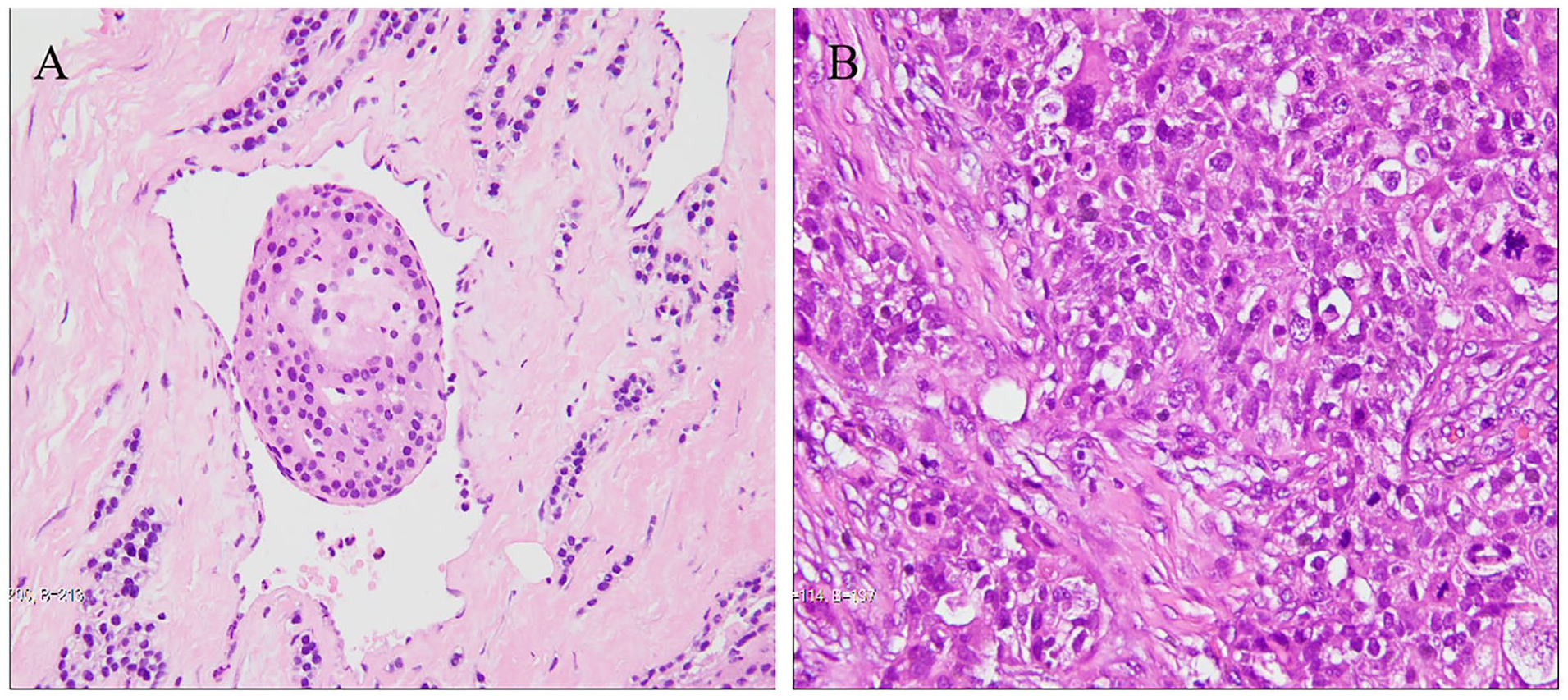
(A) H&E staining of abnormal right upper parathyroid tissue revealed parathyroid carcinoma, tumor cells infiltrate the surrounding soft tissue, arranged in sheet and beam shape, with light staining and uniform nuclei. (B) H&E staining of the left breast mass showed nonspecific invasive breast cancer in the left breast, tumor cells infiltrate the surrounding soft tissue, nuclear atypia, and pleomorphism with scattered mitotic figures.
Discussion
PC is a rare endocrine malignant tumor that accounts for less than 1% of all primary hyperparathyroidism cases, but the incidence of parathyroid cancer has increased in recent years, which may be due to the popularization of serum calcium level monitoring during physical examination, which has focused more attention on the status of the parathyroid glands. 3
The typical clinical symptoms of PC are not obvious in the early stages of PC disease, which sometimes manifests only as elevated serum calcium and PTH levels. Even when the serum calcium and PTH levels are found to be elevated, it is difficult to diagnose PC by imaging and needle biopsy because diagnosis relies mainly on postoperative pathology to confirm the invasion or distant metastasis of PC to surrounding tissue.4,5 In the present case, although the suspicious nodules in the right lobe of the thyroid were initially detected by thyroid ultrasound, their nature was still unclear after further needle biopsy, which may be due to 3 reasons. First, the right upper parathyroid gland invaded the right lobe of the thyroid gland, causing the nodule to appear to be growing from the inside of the thyroid gland on ultrasound images (Figure 1), which mistakenly led us to believe that the nodule was from the thyroid gland rather than the parathyroid gland. Second, further parathyroid-related tests were not conducted. No signs of typical thyroid malignancy were found in the subsequent preoperative CT images, 6 and a clear boundary between the PC tumor and the thyroid was clearly observed in the CT images, suggesting that when the level of PTH and serum calcium increased, ultrasound images revealed suspicious nodules inside of the thyroid (especially abnormal nodules beyond the dorsal membrane). If CT and thyroid imaging tests confirm the same location of the abnormal parathyroid gland, combined with suspicious puncture biopsy results, the possibility of PC should be reasonably suspected, and surgical intervention should be more actively selected. Finally, in this case, the possibility of PC was not initially considered. In addition to the incomplete accuracy of ultrasound imaging and pathological results, another reason that cannot be ignored is that bone metastasis of BC is also common because bone metabolic syndrome, hypercalcemia, and elevated ALP can also occur after bone metastasis. 7 Therefore, the initial diagnosis and treatment plan were that the patient may have BC thyroid metastasis and bone metastasis, inducing a series of related symptoms in the patient. After combining all the factors of the patient, radical mastectomy was selected first, followed by further therapeutic diagnosis through postoperative chemotherapy. Therefore, this case highlighted that the clinical symptoms of early PC are often not obvious and are sometimes only hypercalcemia abnormalities. In opportunistic patients, regardless of the primary disease, when accompanied by hypercalcemia, the existence of hyperparathyroidism should be considered to avoid missed diagnoses.
For the treatment of PC, the focus is to address hypercalcemia syndrome caused by functional PC. For both local lesions and metastatic lesions, the current mainstream view is to surgically remove the lesion as much as possible. 8 At present, no high-quality clinical studies have confirmed the therapeutic effects of chemotherapy and radiotherapy on PC. In the present case, the interval from the patient’s first visit to the radical operation for PC was 6 months, but the size of the parathyroid gland in the ultrasound image did not significantly change. Although various chemotherapy drugs were applied in the treatment process, their effects on PC may be negligible. According to previous reports, the biological characteristics of PC are slow. 9 This may suggest that when PC is accompanied by another rapidly-progressing disease, if the patient is generally not suitable for neck surgery, the priority treatment of the more life-threatening disease can be considered under the premise of effective control of blood calcium.
The patient’s serum calcium and PTH levels have been maintained at normal levels since follow-up. For patients with multiple primary cancers of this type, the follow-up needs of multiple cancers should receive attention at the same time during the follow-up. Importantly, when elevated blood calcium is detected at review, distinguishing between the recurrence of BC with bone metastasis and the recurrence of PC is necessary. To address the above problems, the PTH level can be detected, and if necessary, Tc-99m-MIBI 10 mCi scanning can be performed.
Conclusion
The diagnosis of PC is difficult and mainly depends on postoperative pathology. However, given the aggressive biological characteristics of PC, the results of imaging and other auxiliary examinations should be carefully analyzed to make appropriate choices for subsequent treatment. When PC and other malignant tumors occur at the same time, if it is not possible to perform or prioritize PC at the same time under the condition of effectively controlling the serum calcium level, other diseases can be treated first, and a deadline can be set for PC surgical treatment. However, this idea is not supported by high-quality research at present and needs to be explored further.
Footnotes
Acknowledgements
We thank Zigong First People’s Hospital for the approval of our study.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethics approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient to publish this case report.
Trial Registration Number
Individual cases or case series do not require trial registration number.
Grant Number
None.