
Abstract
Keywords
Introduction
Hypopharyngeal cancer (HPC) is rare 1 and often asymptomatic in early stages. 2 Primary HPC is associated with a high rate of regional nodal metastasis, irrespective of T stage. Therefore, patients are often diagnosed at an advanced stage. 3 Patients with HPC have poor prognosis: the rate of 5-year overall survival (OS) is approximately 35%. 4
Nowadays, the primary treatment of HPC worldwide was predominantly non-surgical treatment.5-8 However, the combined use of chemotherapy and radiotherapy (RT) increases toxicity and sometimes leads to chronic injury and fibrosis of the pharyngeal mucosa, worsening swallowing function. 9 During follow-up, the disease re-presents as persistence/recurrence with poor survival and morbidity outcome, although salvage surgery was done. 10 Therefore, the preferred treatment for HPC in China is surgery, including total laryngectomy (TL) or larynx preservation surgery (LPS) depending on the involvement of larynx, followed by RT or alternating chemoradiotherapy (CRT).11-13 The LPS may be most effective when the primary tumor is located in the lateral wall of the pyriform sinus (LWPS) or in the posterior hypopharyngeal wall (PHPW), and less effective when it is located in the medial wall of the pyriform sinus (MWPS). LPS may not be appropriate when the tumor lies in the post-cricoid region. There are also patients that are not eligible for LPS because of advanced HPC. Yet sometimes, after induction chemotherapy or induction CRT, the primary HPC reduced in size, and LPS became possible. 14
This retrospective study investigated oncologic control, functional outcomes (swallowing, breath, and voice), and quality of life (QoL) in HPC patients treated with LPS and multimodal adjuvant therapy.
Methods
Patients
This retrospective study examined a consecutive cohort of patients with pathology-proven primary HPC who underwent LPS and multimodal adjuvant therapy at Chinese PLA General Hospital between November 2005 and August 2012, or at Capital Medical University Beijing Friendship Hospital between May 2014 and November 2019. HPC was classified according to the TNM system and the American Joint Committee on Cancer (AJCC) criteria (8th edition).
The protocol for the research project has been approved by Bioethics Committee of Beijing Friendship Hospital, Capital Medical University, and that it conforms to the provisions of the Declaration of Helsinki. Written consent was obtained from every patient included in this study.
Larynx preservation surgery
The senior author performed LPS on all patients. Partial pharyngectomy (PP) was performed via lateral pharyngotomy for lesions in the LWPS as described 15 or for lesions in the PHPW as described. 9 In patients with lesions involving the MWPS who were unlikely to require total laryngectomy and in whom tumor-free surgical margins were achieved (confirmed by intra-operational frozen section examination), partial laryngopharyngectomy (PLP) was performed via vertical hemipharyngo-laryngectomy, 16 supracricoid hemilaryngopharyngectomy, 17 or extended supraglottic laryngopharyngectomy. 18 Both PP and PLP can be considered as LPS.
During LPS, the thyroid cartilage sub-crura above the cricothyroid joint was spared in order to protect the recurrent laryngeal nerve (RLN), and care was taken to preserve the superior laryngeal nerve (SLN) and hypoglossal nerve. The primary tumor was resected with curative intent, with a circumferential margin of ≥5 mm. Another 2–3 mm of circumferential residual mucosa were resected (divided into 5–6 pieces according to anatomic locations) for frozen section histopathology to ensure a negative margin. If a certain margin was positive by intra-operational frozen section examination, then corresponding mucosal area was further excised until the margin was confirmed to be tumor-free.
For tumors in the pyriform sinus, the ipsilateral thyroid lobe was routinely resected, and ipsilateral neck dissection at levels II–VI was routinely performed. Decision of contralateral neck dissection was dependent on the findings of preoperative imaging (especially ultrasonography) and intraoperative exploration. For tumors of PHPW primary, the thyroid lobe ipsilateral to the side with greater tumor burden was routinely resected; and bilateral neck dissection at levels II–VI, or radical neck dissection of levels II–VI on the side of severe metastasis (especially extra-nodal extension) and selective neck dissection on the other side, would be performed.
Multimodal adjuvant therapy
Patients in this study received various kind of adjuvant therapies, including chemotherapy, RT, and/or targeted therapy. It was intended that intensity-modulated RT began within 6 weeks after surgery, and it was administered 5 days a week at 2 Gy per day during a 7-week period, reaching a total dose of 70 Gy. Patients may also receive adjuvant chemotherapy (cisplatin, 75 mg/m2, d1; 5-fluorouracil, 750 mg/m2, d1–d5; docetaxel, 75 mg/m2) and/or targeted therapy (cetuximab, 400 mg/m2), according to the recommendations of a multidisciplinary team.
From 2011 onward, enrolled patients who had advanced HPC that were not eligible for LPS, would receive two cycles of induction chemotherapy (cisplatin, 75 mg/m2, d1; 5-fluorouracil, 750 mg/m2) before surgery, in order to reduce tumor size and improve larynx preservation. Then the patients were re-evaluated in order to guide decisions about further treatments, such as surgery or RT.
Outcome assessment and follow-up
The primary endpoint in this study was OS, while secondary endpoints were airway status, function of the voice and swallowing, and QoL.
Following completion of planned treatment, all patients were followed up via routine outpatient visits at 1 and 3 months, and every 3 months thereafter. At each follow-up visit, contrast imaging of swallowing was performed, except in patients with obvious aspiration, who were instead evaluated using a fiberoptic laryngoscope.
Starting at 6 months after the end of treatment, patients were assessed for airway, swallowing, voice and QoL. Airway function was graded as grade 0, normal breath; grade 1, moderate breathing difficulty on exertion (decannulated); grade 2, partial dependence on tracheostomy with intermittent tube occlusion; or grade 3, total dependence on tracheostomy (This grading system was based on the principle investigator’s personal experience).
Swallowing function was evaluated using the Functional Outcome Swallowing Scale (FOSS), 19 which ranges from stage 0 (normal function and asymptomatic) to stage V (non-oral feeding for all nutrition). 20 Swallowing function of stage 0–III was considered satisfactory.
Voice function was evaluated on the Voice Handicap Index (VHI)-10, 21 a self-assessment tool of 10 items, for which each item is scored 0–4. Lower scores represent better voice function.
QoL was assessed using the Functional Assessment of Cancer Therapy-General Questionnaire (FACT-G), 22 which has 27 items and can yield total scores of 0–108. Higher scores represent better QoL.
Overall survival (OS) was calculated from the day of surgery until all-cause death or last follow-up.
Statistical analysis
All statistical analyses were performed using SPSS 26.0 (IBM, Armonk, NY, USA), and P < .05 was considered to indicate statistical significance. Descriptive statistics were used to summarize demographics and baseline characteristics of patients. Continuous data were expressed as mean and standard deviation (SD) or as median and range, and differences were assessed for significance using Student’s t test. Categorical data were expressed as n (%), and differences were assessed using the chi-squared or Fisher’s exact test.
OS was determined using Kaplan–Meier analysis. Univariate analysis was carried out to identify variables associated with swallowing, voice, and QoL. Variables for which the univariate P < .05 were entered into multivariate analysis based on logistic regression or linear regression.
Results
Patient demographics and baseline characteristics
Demographic and baseline characteristics of patients.
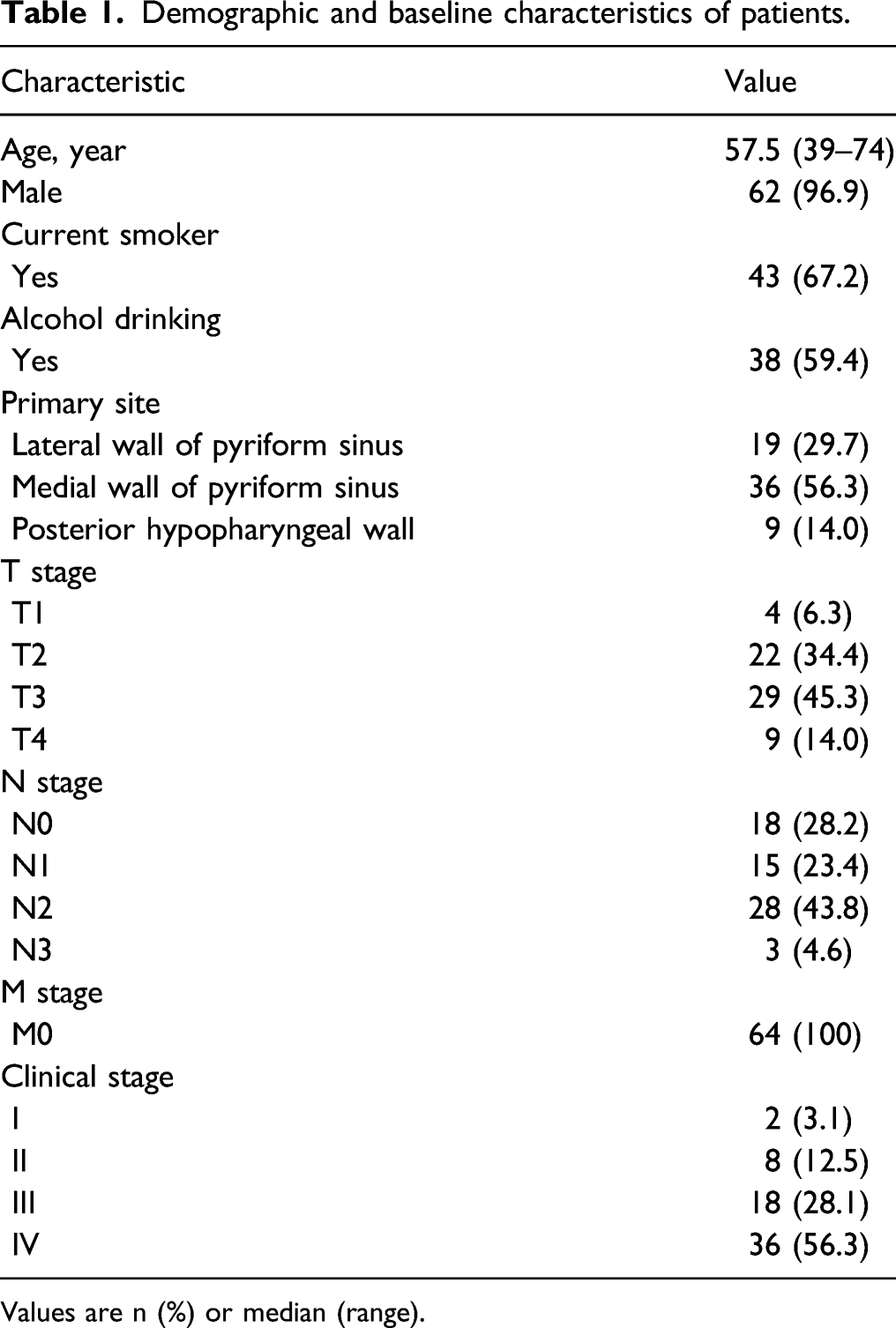
Values are n (%) or median (range).
Treatments
Eight patients received induction chemotherapy, which led to partial tumor shrinkage. All those patients provided informed consent to undergo surgery. Across all patients, median operative time was 180 min (range 120–720 min). Median size of the final hypopharyngeal surgical defect was 12 cm2 (range 5–110). Thirty-eight (59.4%) patients achieved primary closure, and 26 (40.6%) underwent reconstruction. Postoperative pharyngo-cutaneous fistula (PCF) occurred in 8 (12.5%) patients, all of which healed without surgical intervention. No other complications were observed, such as hematoma or pneumonia. Postoperative pathology confirmed squamous cell cancer in all patients and showed tumor differentiation to be low to moderate in 41 (74.1%). 13 patients had postoperative positive surgical margins or lymphatic/vascular invasion.
Thirteen patients received adjuvant chemotherapy (cisplatin, 75 mg/m2, d1; 5-fluorouracil, 750 mg/m2, d1–d5; docetaxel, 75 mg/m2), three of whom received additional targeted therapy (cetuximab, 400 mg/m2). Fifty-four patients underwent intensity-modulated RT, which occurred within 6 weeks after surgery, except for 8 patients who developed PCF, and RT began after their PCF had healed. Two patients (3.1%) declined any form of adjuvant therapy.
Overall Survival
Follow-up lasted a median of 35 months (range 9–136), during which 12 patients (18.8%) experienced locoregional recurrence and 12 (18.8%) experienced distant metastasis without evidence of locoregional recurrence. Most of these patients received palliative therapy rather than salvage treatment after tumor recurrence, while two of them received salvage surgery of total laryngopharyngectomy reconstructed with pectoralis major myocutaneous flap. Unfortunately, the two of them had locoregional recurrence after 6 and 11 months of disease-free survival respectively and died afterward. Among the 12 patients experiencing locoregional recurrence during follow-up, 7 of them had adverse features on pathology. Among the 52 patients without locoregional recurrence, 6 of them had adverse features on pathology. Thus, adverse features were associated with lower locoregional control rates significantly (P < .05).
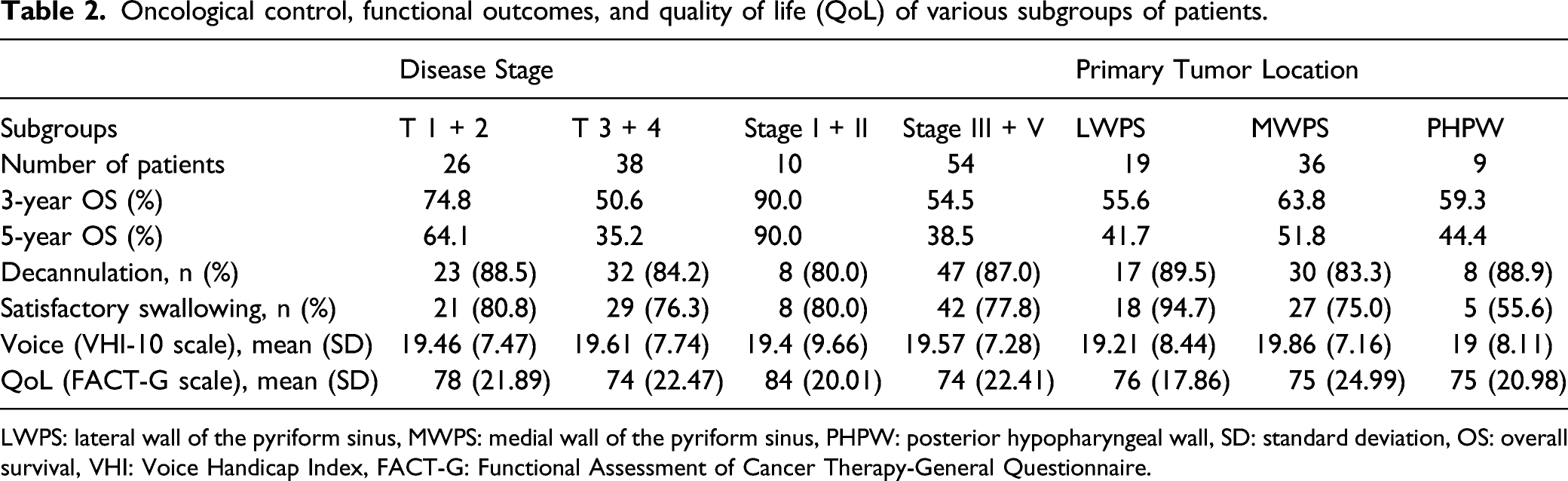
Three patients died of a second primary cancer, and eight died of other causes. OS rates were 60.7% at 3 years and 47.3% at 5 years (Figure 1A). OS rate was significantly higher for patients with T1 or T2 HPC than for patients with T3 or T4 disease (HR 2.27, 95% CI 1.11–4.64, log-rank P = .034; Table 2 and Figure 1B), and higher for patients with stage I or II disease than for those in stage III or IV (HR 8.64, 95% CI 3.69–20.2, log-rank P = .010; Table 2 and Figure 1C). Kaplan–Meier survival curves for overall survival among all patients (A) without stratification, or stratified by (B) T stage or (C) clinical stage. Shown are hazard ratios (HR), 95% confidence intervals (CIs), and log-rank P values. Oncological control, functional outcomes, and quality of life (QoL) of various subgroups of patients. LWPS: lateral wall of the pyriform sinus, MWPS: medial wall of the pyriform sinus, PHPW: posterior hypopharyngeal wall, SD: standard deviation, OS: overall survival, VHI: Voice Handicap Index, FACT-G: Functional Assessment of Cancer Therapy-General Questionnaire.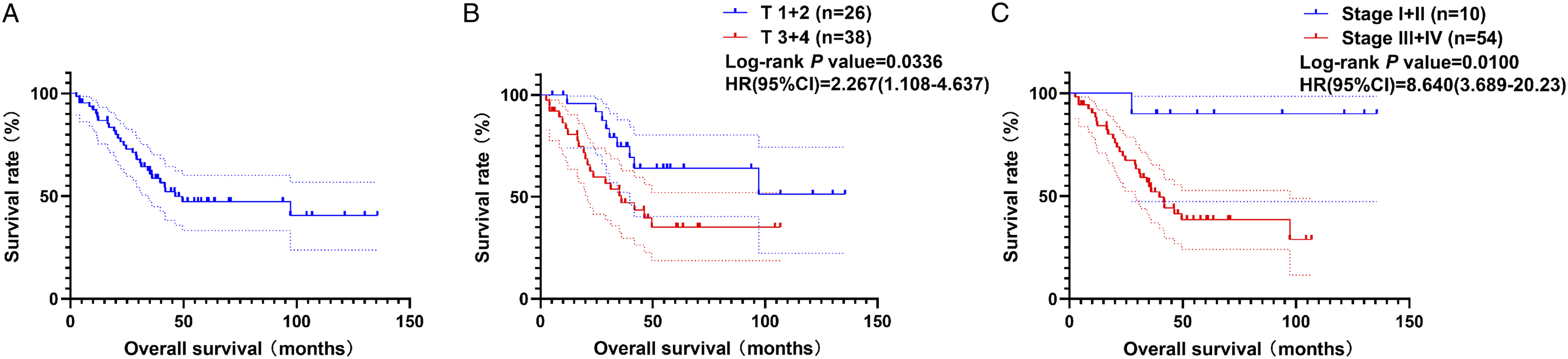
Airway status and breathing ability
Decannulation (grade 0/1) was successful in 55 patients (85.9%). The airway was maintained open by tracheostomy in 9 patients (14.1%), of whom 7 were in grade 2 and 2 were in grade 3. Decannulation grade did not differ significantly among patients with HPC in different locations or with HPC in different stages (Table 2).
Swallowing
Fifty patients (78.1%) showed satisfactory swallowing function (grade 0–III) based on FOSS criteria (see Table 2). Univariate analysis identified history of alcohol drinking, size of surgical defect and local recurrence as significantly associated with swallowing function. (Data not shown) Multivariate analysis further identified local recurrence as an independent predictor of swallowing function (HR 11.395, 95% CI 2.334–55.617, P = .003). Esophageal dilatation was performed in four patients, who experienced temporary relief.
The rate of patients achieving satisfactory swallowing was significantly higher among those whose lesion was in the LWPS than in those whose lesion was in the PHPW (94.7% vs. 55.6%, P = .026, Table 2). Neither the difference between LWPS and MWPS, nor that between MWPS and PHPW, were statistically significant. The rate did not differ significantly across disease stages.
Voice
Median VHI-10 score was 19 (range 4–40), and it did not differ significantly across disease stages, or among primary sites (Table 2). Univariate analysis identified history of smoking or alcohol drinking, N stage, and decannulation as significantly associated with voice function. Multivariate analysis identified decannulation as an independent predictor of voice function (Data not shown).
Quality of life
Median FACT-G score was 75 (range 16–105), which did not differ significantly across disease stages, or among primary sites (Table 2). Univariate analysis identified history of smoking or alcohol drinking, N stage, local recurrence, decannulation and need for a feeding tube as significantly associated with QoL. Multivariate analysis further identified the need for a feeding tube as an independent predictor of QoL. (Data not shown)
Discussion
Preserving laryngeal function is generally defined as preserving glottal phonation without a prothesis, the ability to swallow food without aspiration or a feeding tube, and the ability to breathe without a permanent tracheostomy.2,17 Preserving laryngeal function, in our experience, requires retaining as much as of the larynx as possible, as well as protecting the contralateral or even ipsilateral superior laryngeal nerve, especially their internal branches innervating the supra-glottis and glottis. The goal is to retain fine tactile sensation in the residual larynx and thereby avoid aspiration. The superior laryngeal vascular pedicles should be ligated with great care.
Our results suggest that surgery is effective at treating primary HPC in the PHPW, which is supported by literature. 23 Such tumors lie relatively far from the larynx and seldom involve it, even in advanced disease. In addition, HPC in the PHPW frequently resists RT, 24 and it necessitates a wider, circumferential mucosal radiation field in contrast to the unilateral field applied when the tumor lies in the pyriform sinus. The wider radiation field may increase risk of dysphagia and stricture formation, prolonging dependence on a feeding tube. 25 We suggest that surgery may be the optimal treatment for primary HPC of the PHPW. In contrast, we advise against LPS for patients with tumors in or involving the post-cricoid region, bilateral crico-arytenoid unit, cricoid cartilage, cricopharyngeal muscle, cervical esophagus, tongue base, or oropharyngeal and prevertebral muscles.
For patients with HPC in selected locations, our results and previous studies 26 suggest that LPS followed by full-dose RT is likely to be effective. Full-dose RT was preferred than the lower standard doses because of the following reasons. Radiotherapy doses <60 Gy was associated with lower locoregional control rates. 27 Doses over 60 Gy after partial laryngectomy showed little evidence of additional toxicity. 28 This regimen can lead to good OS and functional outcomes in most patients with early-stage HPC, but it should be carefully applied to selected patients with advanced disease. A precondition for LPS is a functioning contralateral “crico-arytenoid unit,” whereas N status does not seem to matter.26,29 We further suggest that patients selected for surgery should have good pulmonary functional reserves, motivation, and access to psychological support to ensure that they can cope with prolonged swallowing rehabilitation. 3
The patient’s systemic condition is another factor to consider when deciding for or against LPS. Poor systemic condition, such as poor cardiopulmonary function or severe diabetes mellitus, may be a contraindication because of significantly higher risk of postoperative complications. Another contraindication may be a cervical metastatic lesion whose resection is judged to be impossible, such as lesions encasing common/internal carotid artery or involving bilateral internal jugular veins.
Oncologic control and functional outcome of LPS-treated HPC patients.
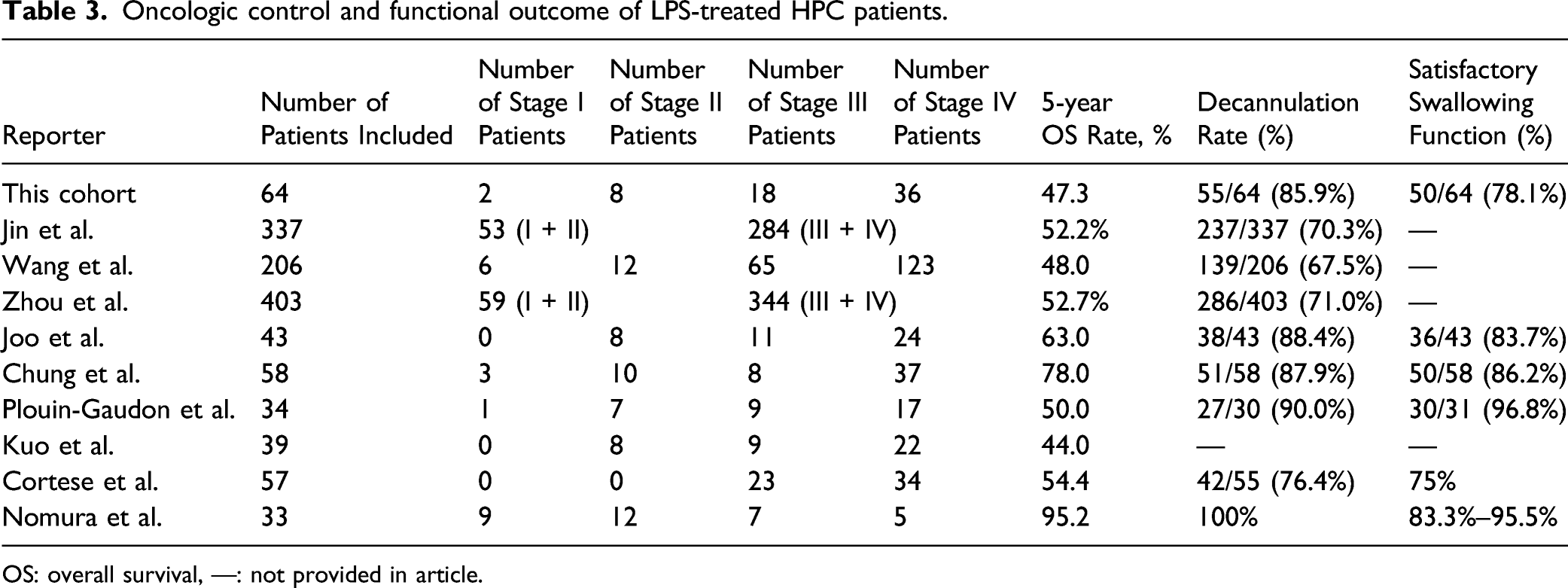
OS: overall survival, —: not provided in article.
Comparison of outcomes between the present cohort and previously reported patients treated non-surgically.
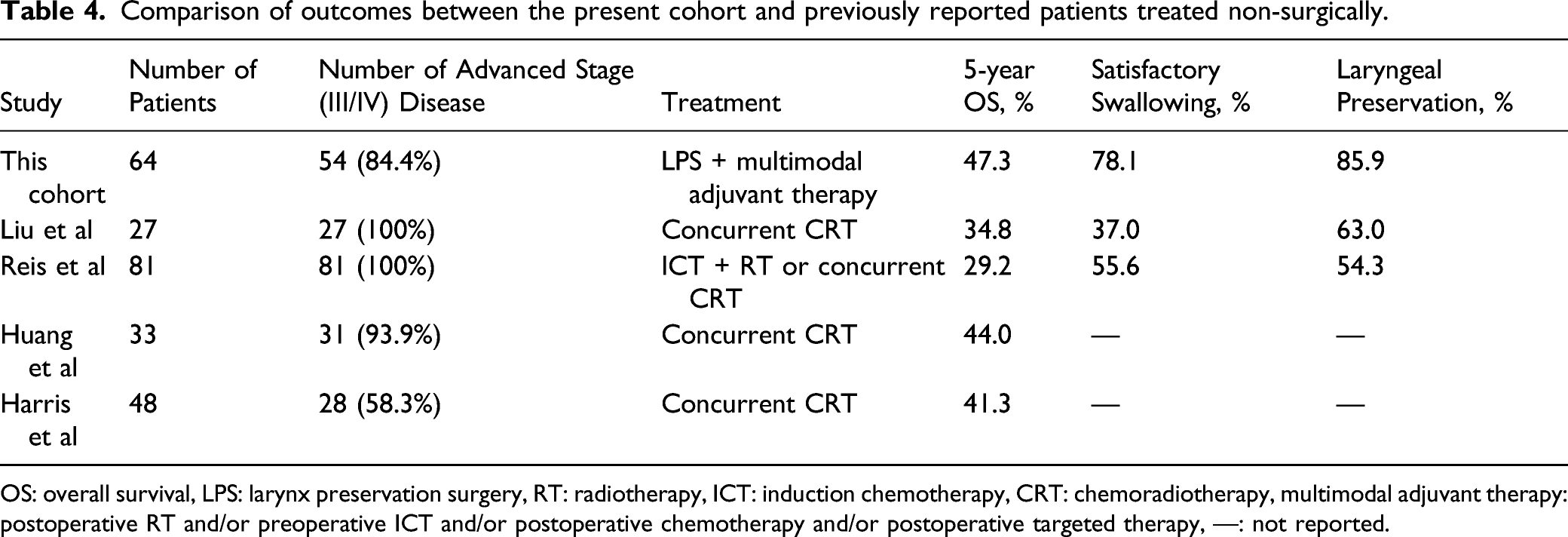
OS: overall survival, LPS: larynx preservation surgery, RT: radiotherapy, ICT: induction chemotherapy, CRT: chemoradiotherapy, multimodal adjuvant therapy: postoperative RT and/or preoperative ICT and/or postoperative chemotherapy and/or postoperative targeted therapy, —: not reported.
There were some advantages in this study. The surgery-oriented therapy was popular in China. We would like to add some evidence in the debate of “surgery vs non-surgery.” Furthermore, this study presented the data of oncologic control, functional outcomes (swallowing, breath, and voice), and quality of life (QoL) for 64 HPC patients treated with LPS. The number of cases was reasonable and the follow-up information was complete. Univariate and multivariate analysis were carried out to identify variables associated with these outcomes (data not shown because of limited number of tables).
There are several limitations of the study. As a retrospective review of case series, there is no control group to compare to. Selection bias is to be expected, as patients amenable for LPS may have better prognosis than non-surgical patients with the same clinical stage. And number of included patients was relatively small, compared with other rather large series. But there are some virtues of this report. All included patients were operated on by the same senior surgeon. There was detailed data on important aspects of functional outcomes, and in particular, subsites of disease origin were documented separately, which was not commonly performed and might add to literature.
Conclusion
For selected patients with primary HPC, especially stage I or II disease, LPS and multimodal adjuvant therapy can provide satisfactory oncologic control, OS, and functional outcome (successful decannulation and satisfactory swallowing).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Key Science and Technology Program of Beijing Municipal Commission of Education [grant number KZ202110025035], Seed Project of Beijing Friendship Hospital, Capital Medical University [grant number YYZZ202125], Research and Development Project of Scientific Research Instruments and Equipment of Chinese Academy of Sciences-major instruments project [grant number YJKYYQ20180039] and Digestive Medical Coordinated Development Center of Beijing Municipal Administration of Hospitals [grant number XXZ0604].