
Abstract
Objective
Under current standards of treating highly aggressive hypopharyngeal cancer (HPC), oncological control and functional outcome are still unsatisfactory worldwide. This study explored the surgery-oriented comprehensive treatment approach based on 15 years of practice.
Methods
A retrospective cohort of HPC patients treated by the senior author at Chinese PLA General Hospital between Nov 2005 and Aug 2012 and Capital Medical University Beijing Friendship Hospital between May 2014 and Nov 2019 was studied. Oncological control, swallowing function, and quality of life (QoL) were assessed.
Results
In total, 122 patients were included in this study, with 11 (9.0%) cases in the early stage and 111 (91.0%) cases in the advanced stage. Five-year overall survival (OS) and disease-free survival (DFS) were 40.0% and 36.1%, respectively. The swallowing outcome was satisfactory in 90 (73.8%) patients. Tracheostomy-free survival was achieved in 55 (45.1%) patients. Multivariate cox regression analysis showed that the size of the surgical defect, local-regional recurrence, and distant metastasis were independent impact factors for OS and DFS (P < .05). Multivariate analysis showed that the logistic regression coefficients (standard error) of pharyngo-cutaneous fistula and local-regional recurrence on swallowing function were 1.274 (.532) and 1.283 (.496), respectively (P < .05). In addition, the logistic regression coefficients (standard error) of the clinical stage, local-regional recurrence, decannulation, and feeding tube on QoL were −7.803 (3.593), −7.699 (3.151), 13.853 (3.494), and −20.243 (3.696), respectively (P < .05).
Conclusions
Surgery-oriented comprehensive treatment can give rise to good swallowing function without jeopardizing oncological control. The size of the surgical defect, local-regional recurrence, and distant metastasis were independent factors impacting OS and DFS. Pharyngo-cutaneous fistula and local-regional recurrence were independent factors impacting swallowing function. Clinical stage, local-regional recurrence, decannulation, and feeding tube were independent factors impacting QoL.
Keywords
Introduction
Hypopharyngeal cancer (HPC) is reported as one of the most aggressive cancers of the head and neck region.1–4 The primary tumor commonly causes intra-luminal obstruction of the upper aerodigestive tract, leading to progressive swallowing problems (dysphagia), hoarseness of voice (dysphonia), and airway compromise (dyspnea). 5 Most patients present with advanced-stage disease at the initial diagnosis. Early-stage HPC tumors are small in size and volume and manifest nonspecific symptoms, making early diagnosis difficult if not impossible without specialist examination. 6 The prognosis of HPC is poor, with a 5 year overall survival (OS) rate of around 40%.2,4,7
The treatment goals are to achieve local-regional tumor control with preservation of laryngopharyngeal functions: tracheostomy-free breathing, ability to maintain body mass (weight) by a daily oral diet, and ability to vocalize. 4 Transoral surgery, including transoral laser microsurgery (TLM) and transoral robotic surgery (TORS), has enabled oncologic surgeons to remove tumors without the need of breaching the neck skin. This treatment modality avoids many of the complications of conventional open neck surgery (scar formation, pharyngo-cutaneous fistula, infection, and hemorrhage), allowing rapid functional recovery, particularly swallowing. 8 This surgical technique is recommended for selected cases.
Although it was reported that the temporal sequence of surgery and radiotherapy (RT) did not affect prognosis, 9 a recent study concluded that patients receiving postoperative radiation alone had superior swallowing outcomes and equivalent speech outcomes relative to the preoperative radiation group. 10 Moreover, some authors advocate that primary total laryngo-pharyngectomy remains the “gold standard” treatment for T4 HPC (with extra-laryngeal extension) because it gives rise to satisfactory oncologic and functional outcomes. 11 Furthermore, it was reported that patients with advanced-stage HPC treated surgically with adjuvant RT or chemoradiotherapy (CRT) showed a trend toward clinically improved OS compared with patients treated with definitive CRT; however, the difference was not statistically significant. 12
In China, surgery followed by RT is the mainstream treatment, and the maximal restoration of pharyngo-esophageal continuity and function improves survival in patients whose tumors are excised completely. 8 This report reviews the clinical data from a cohort of 122 HPC patients undergoing surgery-oriented comprehensive treatment, including preoperative induction chemotherapy, postoperative intensity-modulated RT (IMRT), chemotherapy, or targeted therapy, focusing on their oncologic control and functional outcome, especially swallowing function outcome.
Methods
Patients
The eligible HPC patients were collected based on inclusion and exclusion criteria.
This retrospective study investigated a consecutive series of HPC patients surgically treated by the senior author at Chinese PLA General Hospital from Nov 2005 to Aug 2012 and at Capital Medical University Beijing Friendship Hospital from May 2014 to Nov 2019. All the surgical procedures were performed by a single surgeon to eliminate the surgeon’s bias. The following aspects were analyzed and summarized: patient demographics, presenting symptoms, medical history, treatment, complications, survival, swallowing function outcome, and QoL.
The study protocol was approved by the authors’ institutions, and the requirement for patient consent was waived because of the retrospective nature of the study and anonymized analyses. All the patients or their legal surrogates provided written informed consent to undergo surgery.
Every HPC patient was subjected to a multidisciplinary team (MDT) session to determine the most suitable and individualized course of treatment.
Preoperative therapies
Since 2011, for patients whose lesion was too advanced to preserve the larynx, two sessions of induction chemotherapy (cisplatin, 75 mg/m2, d1; 5-fluorouracil, 750 mg/m2), or induction CRT chemotherapy and preoperative radiotherapy (additional RT dose of 40–50 Gy) were administered. Then the patients were re-evaluated to determine further course of treatment: RT for complete remission, RT or surgery for partial remission, and surgery for no response or disease progression.
Patients diagnosed with a synchronous second primary esophageal carcinoma underwent treatment by endoscopic submucosal dissection, RT, CRT, or open surgery, based on the depth of tumor infiltration, distance from HPC, and their general condition, before treatment of the hypopharyngeal lesion.
Surgical procedures
Based on preoperative examination results, the location and size of the primary tumor could be accurately estimated. A variety of surgical procedures have been described in the literature to achieve complete tumor removal. Procedures of larynx preservation surgery (LPS) consisted of partial pharyngectomy 13 and partial laryngo-pharyngectomy, 14 including extended supra-glottic laryngo-pharyngectomy, 15 supra-cricoid hemi-laryngo-pharyngectomy, 16 and vertical hemi-pharyngo-laryngectomy. 17 When the larynx could not be preserved, the following procedures were performed: total laryngectomy (TL) with partial pharyngectomy, total laryngo-pharyngectomy (TLP), TLP with cervical esophagectomy, and total laryngo-hypopharyngeo-esophagectomy.
A functioning contra-lateral “crico-arytenoid unit” was paramount when considering LPS,1,18 while the N status of the patients’ disease generally did not influence the type of LPS surgery undertaken. Furthermore, it was paramount for LPS candidates to have a good pulmonary functional reserve, motivation, and psychological support to ensure that they could cope with the potentially prolonged period possibly required for swallowing rehabilitation. 19
We would advise against laryngeal preservation if any of the following anatomical locations were involved or the situation was confirmed: postcricoid region, impaired bilateral crico-arytenoid units, extensive involvement of the cricoid cartilage, cricopharyngeal muscle, extensive involvement of cervical esophagus, tongue base, and oropharyngeal or prevertebral muscles. Besides, if the patient’s systemic condition was worrying, especially in the case of adverse cardiopulmonary function or severe diabetes mellitus, we would also advise against LPS to minimize postoperative complications. These can also be considered as an indication for TL.
Multiple reconstruction choices could be utilized, and there was an order for our choice: as long as primary closure (without undue tension or laxity) could be achieved, we would not use any flap; as long as a regional pedicled flap could be used, we would not use free tissue flap, which would need time-consuming microscopic vessel anastomoses. The surgical defect was always closed with the most simple, convenient, and quick method. For circumferential hypopharyngeal defect, we preferred radial forearm free flap (RFFF), which was pliable and easy to manipulate. An anterolateral thigh (ALT) free flap could also be used if the patient was thin enough. If the esophagus was seriously involved and could not be completely removed through a cervical incision, then we would cooperate with thoracic surgeons to remove the entire esophagus and perform tubular gastric pull-up pharyngo-gastric anastomosis. Selective or modified radical or radical neck dissection would be performed when necessary.
NG-FT feeding would be initiated on the first postoperative day. Oral feeding, along with NG-FT feeding, would be tried on the 10th postoperative day for primary cases and on the 14th postoperative day for salvage cases. The patients were suggested to have a liquid diet at first and gradually change it to a soft diet. NG-FT would be removed once patients could take in sufficient food orally (usually the second day of oral feeding), without evidence of pharyngo-cutaneous fistula. After completion of RT, the decannulation of tracheotomy tubes should be planned in a graduated fashion for LPS recipients. Cuffed tracheotomy tubes would be changed to metal ones once patients could drink water without aspiration with the cuff deflated and could only be removed when they could be spigotted day and night for a month.
Postoperative adjuvant therapies
In the treatment planning, all the patients with advanced clinical stage disease would receive postoperative adjuvant RT, preferably commencing within 6 weeks, delivered by IMRT: 5 days a week, 2 Gy/day over 7 weeks, reaching a total dose of 60–70 Gy. Radical radiotherapy (i.e., 70 Gy) should be given in the presence of any postoperative adverse risk factors, such as positive resection margin and extracapsular nodal spread. Otherwise, a prophylactic postoperative radiotherapy dose (i.e., 60 Gy) was given. Patients developing pharyngo-cutaneous fistula (PCF) had delayed RT when the fistula had healed. Alternating or concurrent chemotherapy (cisplatin, 75 mg/m2, d1; 5-fluorouracil, 750 mg/m2, d1–d5; docetaxel, 75 mg/m2), and/or targeted therapy (cetuximab, 400 mg/m2) would also be administered, based on the presence of clinicopathological risk factors (N stage, extra-nodal extension, perineural and perivascular invasion, etc.).
Outcome assessment and follow-up
All the patients were followed up via routine outpatient appointments: one month, 3 months, and every 3 months after that. Barium swallow x-ray was routinely performed during every follow-up visit, except for patients with apparent aspiration, who would be evaluated with a fiberoptic laryngoscope. Swallowing function outcome and QoL were routinely evaluated commencing from 6 months. The scores of swallowing function outcome and QoL, used for further analyses, were from the individual’s latest evaluation.
The swallowing function was evaluated regarding a functional outcome swallowing scale (FOSS). 1 Symptom criteria ranged from stage 0 (normal function and asymptomatic) to stage V (nonoral feeding for all nutrition). Swallowing function at or above stage III was considered satisfactory because patients could swallow orally, and aspiration was avoided. The functional assessment of cancer therapy-general (FACT-G) questionnaire was used to evaluate patients’ general postoperative QoL. The FACT-G (version 4) consists of 27 items rated on a 0–4 Likert-type scale, divided into four subscales that assess physical well-being, social/family well-being, emotional well-being, and functional well-being. The total score range was 0–108, 20 with higher scores representing better QoL. The status of breath and voice was recorded for LPS recipients only. OS was calculated from the day of surgery until all-cause death or last follow-up.
Statistical analysis
OS and disease-free survival (DFS) were determined by Kaplan–Meier analysis. For postoperative course and functional results, the chi-squared test or Fisher’s exact test was used to compare differences between categorical variables, and the t-test was conducted to compare differences in continuous variables.
All the variables associated with P <.05 on univariate analysis were included in the logistic (qualitative variables) or linear (quantitative variables) regression models (enter) for multivariate analysis (conducted only when more than one factor was significant in univariate analyses). All the statistical analyses were performed by SPSS 26.0 (IBM Corp, Armonk, NY).
Results
Patient demographics and baseline characteristics
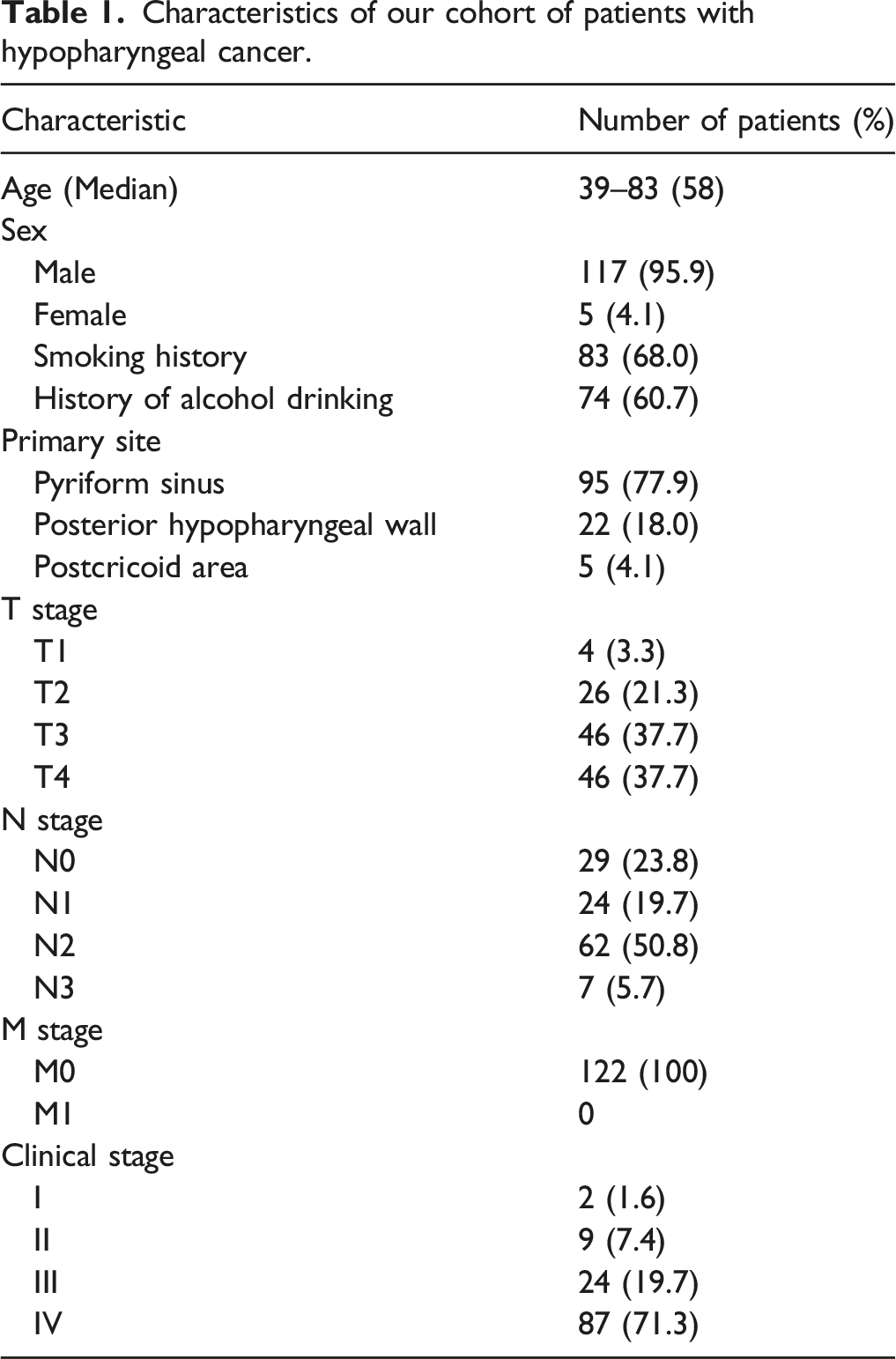
Characteristics of our cohort of patients with hypopharyngeal cancer.
Analysis of sub-groups of patients and primary tumor subsites.
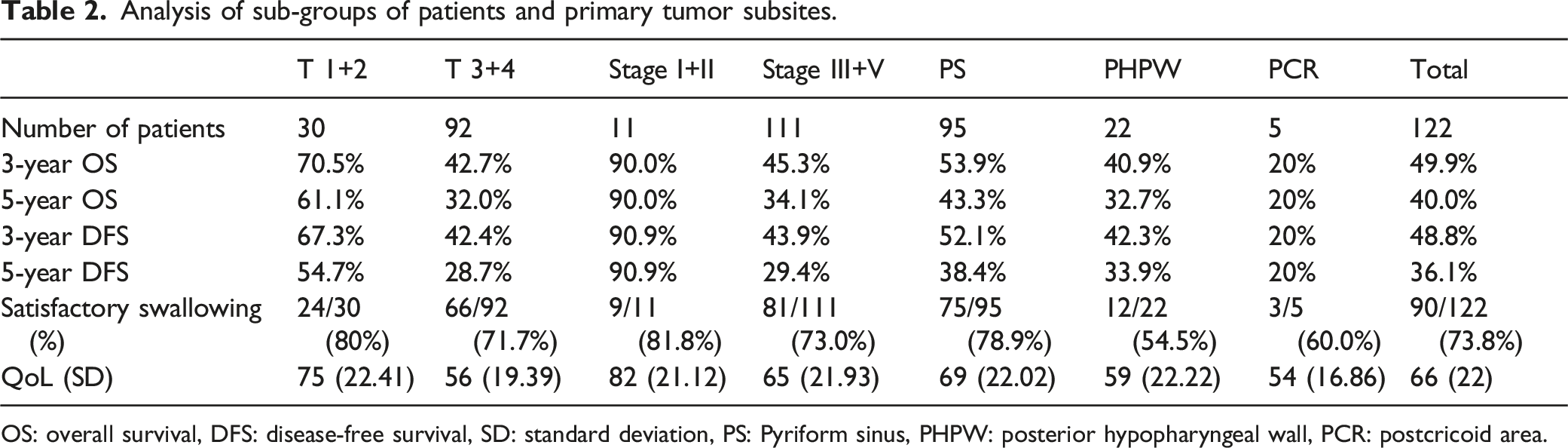
OS: overall survival, DFS: disease-free survival, SD: standard deviation, PS: Pyriform sinus, PHPW: posterior hypopharyngeal wall, PCR: postcricoid area.
Treatment
Thirteen patients underwent induction chemotherapy (five cases) or induction CRT chemotherapy and preoperative radiotherapy (eight cases). As there was no objective evidence of tumor shrinkage up to partial remission, the patients were informed, who agreed to surgical treatment (eight LPS cases and five TL cases). Salvage surgery was performed on four additional cases due to the failure of tumor control after definitive RT, whose HPC tumor has remained stable following a total dose of 70 Gy.
Comparison between patients receiving laryngeal preservation surgery (LPS) and total laryngectomy (TL).
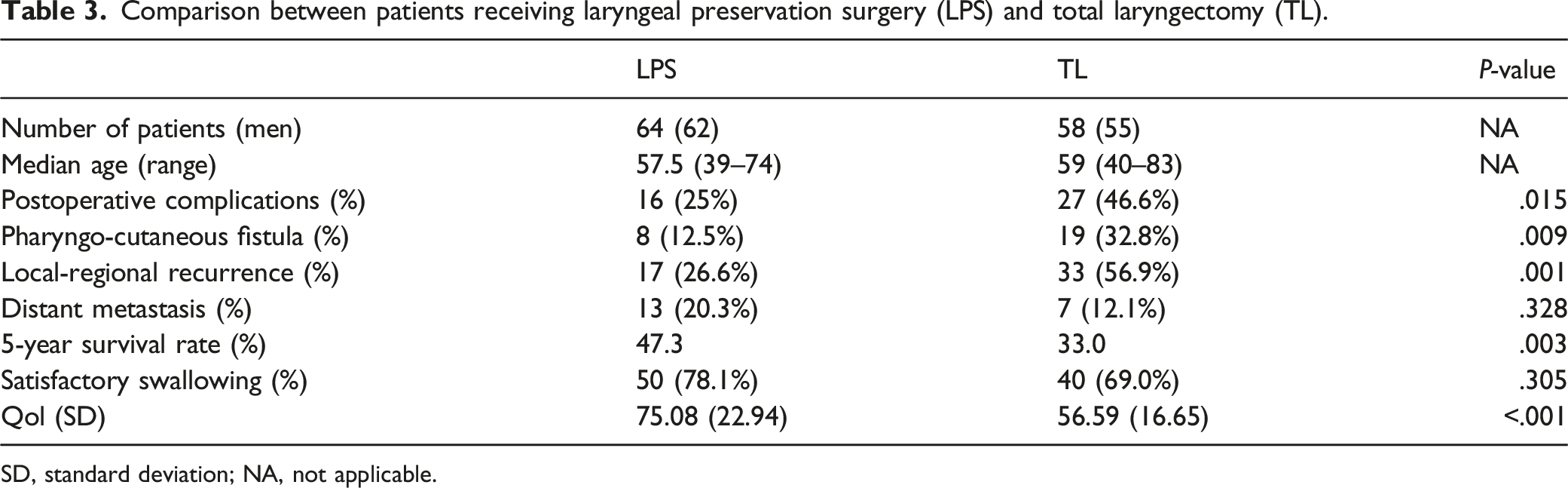
SD, standard deviation; NA, not applicable.
The final hypopharyngeal surgical defect measurement ranged between 5 cm2 and 110 cm2, with a median size of 16 cm2. Primary closure was achieved in 62 (50.8%) patients, while reconstruction was necessary in 60 (49.2%) patients. Reconstruction methods included 25 cases of the submental flap, 5 cases of RFFF (see Figure 1), 3 cases of the gastric pull-up, 1 case of ALT free flap, and various other methods. Preoperative examination, intraoperative photo, and postoperative follow-up of a hypopharyngeal cancer patient with surgical defect reconstructed by radial forearm free flap (RFFF). (A) Preoperative enhanced CT shows a massive right hypopharyngeal mass (yellow arrow) (B) Preoperative enhanced MRI T1WI sagittal view shows a massive right hypopharyngeal mass (yellow arrow) (C) Preoperative barium swallow x-ray shows a massive right hypopharyngeal filling defect, indicating a giant mass (D) The RFFF was sutured into a tube with skin lining the lumen before being inserted into the surgical defect (E) Surgical defect reconstructed by the RFFF tube (F) Barium swallow x-ray two months postoperatively shows the smooth flow of barium through the hypopharynx into the esophagus (G) Barium swallow x-ray 10 months postoperatively shows the smooth flow of barium through the hypopharynx into the esophagus.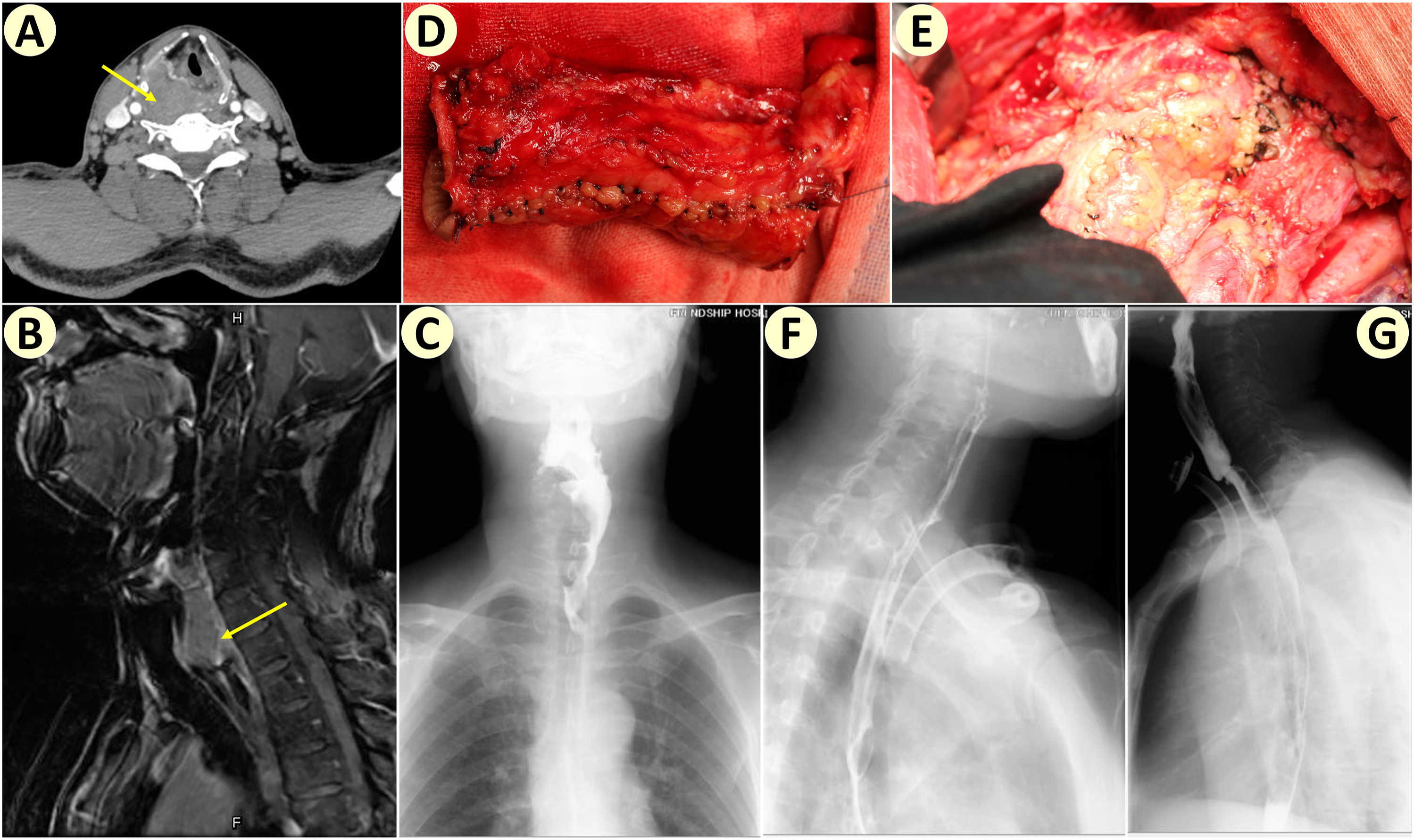
Neck dissection was necessary in 120 (98.4%) patients. Forty-three (35.2%) patients experienced complications. There were 27 (22.1%) cases of PCF (including 3 salvage cases), 6 (5.0%) cases of postoperative pneumonia, 4 (3.3%) cases of postoperative hemorrhage, 4 (3.3%) cases of local infection, 1 (.8%) case of chylous fistula, and 1 (.8%) case of neo-pharyngeal stenosis. To manage PCF, conservative treatment was successful in 23 cases, a pecto-deltoid flap was used for two other cases, and a pectoralis major musculocutaneous flap was used for yet another case. In one salvage case, the PCF could not be repaired.
IMRT was undertaken within 6 weeks for 90 (73.8%) patients: 5 days a week, 2 Gy/day over 7 weeks, reaching a total dose of 60–70 Gy; among them, 23 patients also received alternating chemotherapy (cisplatin, 75 mg/m2, d1; 5-fluorouracil, 750 mg/m2, d1–d5; docetaxel, 75 mg/m2), with four receiving additional targeted therapy (cetuximab, 400 mg/m2). PCF resulted in delayed RT in 18 (14.6%) patients. Three (2.5%) patients rejected any postoperative adjuvant therapy.
Survival
The follow-up ranged between 9 months and 136 months. Recurrence occurred in 45 cases: 25 patients had local recurrence; 12 patients had regional recurrence; 1 patient had both local and regional recurrence; and 7 patients had local and regional recurrence, with distant metastasis. All these patients chose chemo/targeted therapy and died subsequently. There were 12 other distant metastasis cases alone, including lung, liver, brain, and cervical vertebrae. In addition, two patients died of second primary lung cancer, one patient died of second primary nasopharyngeal carcinoma, and another patient died of second primary esophageal carcinoma. Furthermore, 14 other patients died of unrelated causes, including four cases of pneumonia, two cases of cardiac infarction, two cases of cerebral infarction, one case of pulmonary embolism, and various other reasons.
According to Kaplan–Meier analysis, 3 year and 5 year OS rates were 49.9% and 40.0%, respectively, while 3 year and 5 year DFS rates were 48.8% and 36.1%, respectively (Figure 2). Interestingly, the OS of stage I+II was very good, with 5 year OS at 90.0% (Table 2). Further analysis showed that the difference between the OS of stage I+II and stage III+IV was statistically significant (HR = 11.60, 95% CI: 5.908 to 22.77, log-rank P=.0018; Figure 2C), and the difference between the OS of T1+2 and T3+4 was also statistically significant (HR = 2.585, 95% CI: 1.550 to 4.311, log-rank P=.0024; Figure 2D). However, the differences in OS and DFS were not statistically significant between different primary sites. Kaplan–Meier survival analyses. Kaplan–Meier survival curves for overall survival (A) and disease-free survival (B) Kaplan–Meier overall survival curves according to the clinical stage (C) and T stage (D) hazard ratio (HR) and its 95% confidence interval (CI) and log-rank P-value.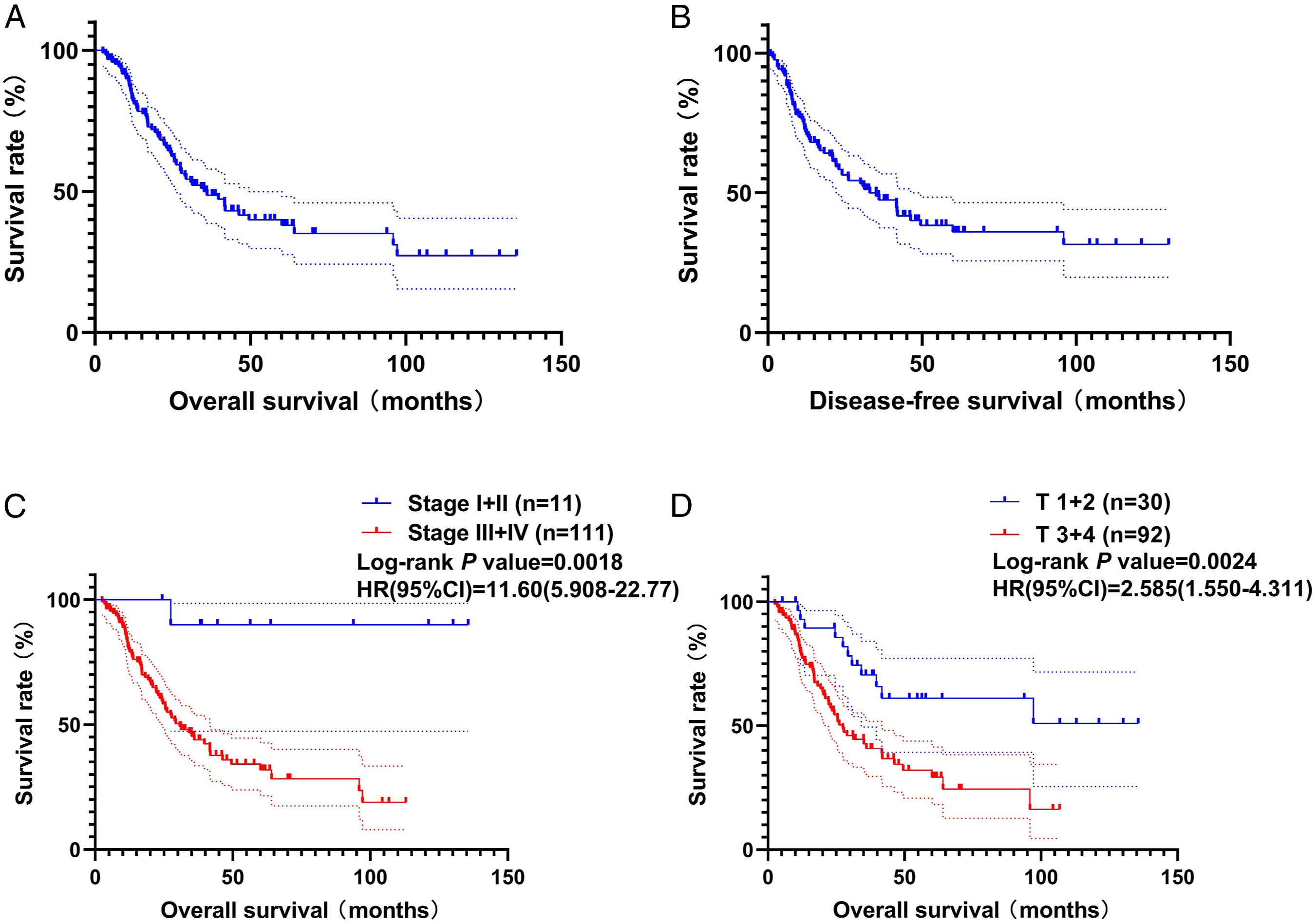
The 5 year OS rates of LPS and TL recipients were 47.3% and 33.0%, respectively (Table 3), and this difference was statistically significant (HR = 2.036, 95% CI: 1.229 to 3.375, log-rank P=.0029; data not shown). Furthermore, the differences in postoperative complications, PCF, and local-regional recurrence were statistically significant between LPS and TL recipients. We assumed these differences were because TL recipients had more advanced disease than LPS recipients, although the difference in distant metastasis between LPS and TL recipients was not statistically significant. (Table 3)
Univariate analysis showed that T stage, N stage, clinical stage, and pathological risk factors impacted local-regional recurrence. Further multivariate analysis showed that T stage, N stage, and pathological risk factors independently impacted local-regional recurrence. No factor was found to impact distant metastasis by univariate analysis (data not shown).
Impact of clinical factors on OS and DFS: univariate/multiple cox regression analysis.
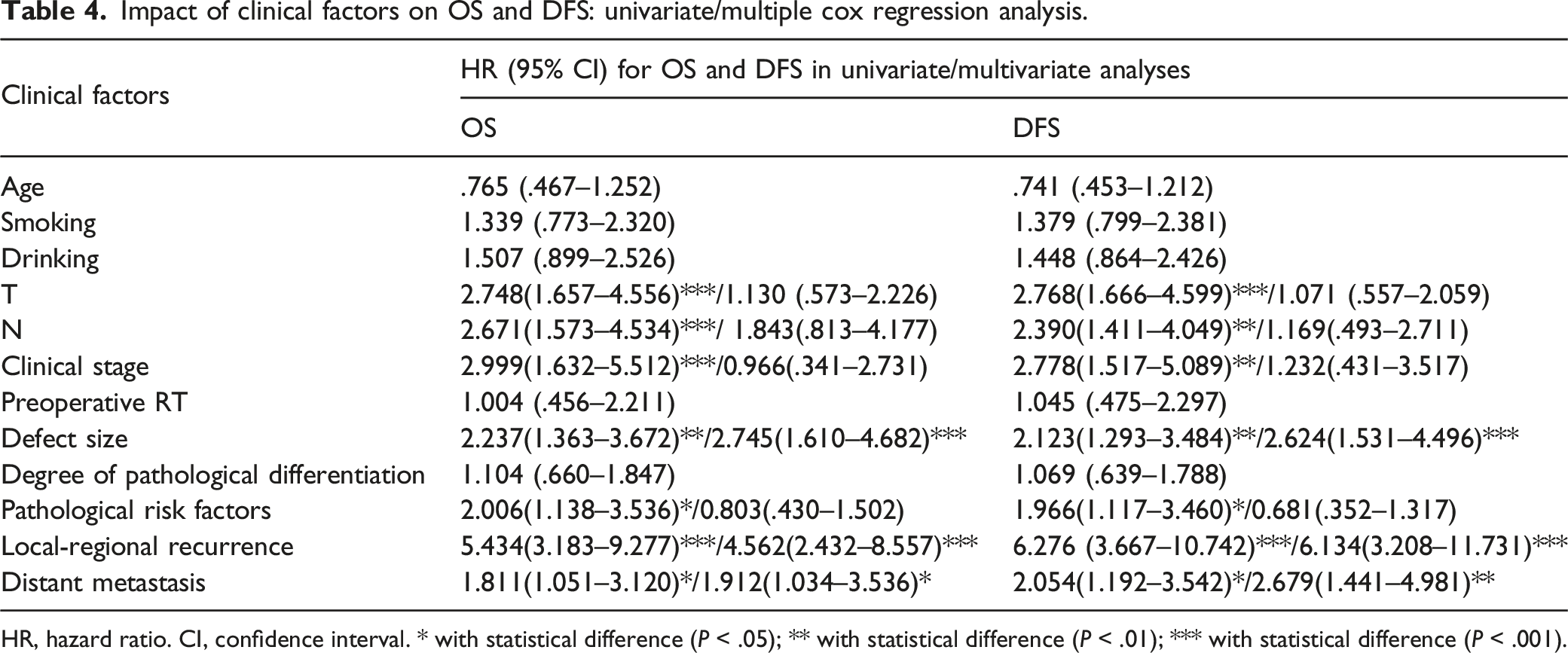
HR, hazard ratio. CI, confidence interval. * with statistical difference (P < .05); ** with statistical difference (P < .01); *** with statistical difference (P < .001).
Functional outcome
Swallowing function
The duration from surgery to full oral food intake was 10–150 days (average time = 24.02 days, while the median was 14 days). Swallowing was deemed “satisfactory” in patients with FOSS Grade 0–III: 17 cases of Grade 0, 20 cases of Grade I, 26 cases of Grade II, and 27 cases of Grade III. In total, swallowing function was satisfactory in 90 (73.8%) patients. Unsatisfactory swallowing was recorded in 28 cases of Grade IV and 3 cases of Grade V. The differences in swallowing function between different primary sites were not statistically significant (Table 2).
Impact of clinical factors on swallowing function: univariate/ multiple logistic regression analysis.
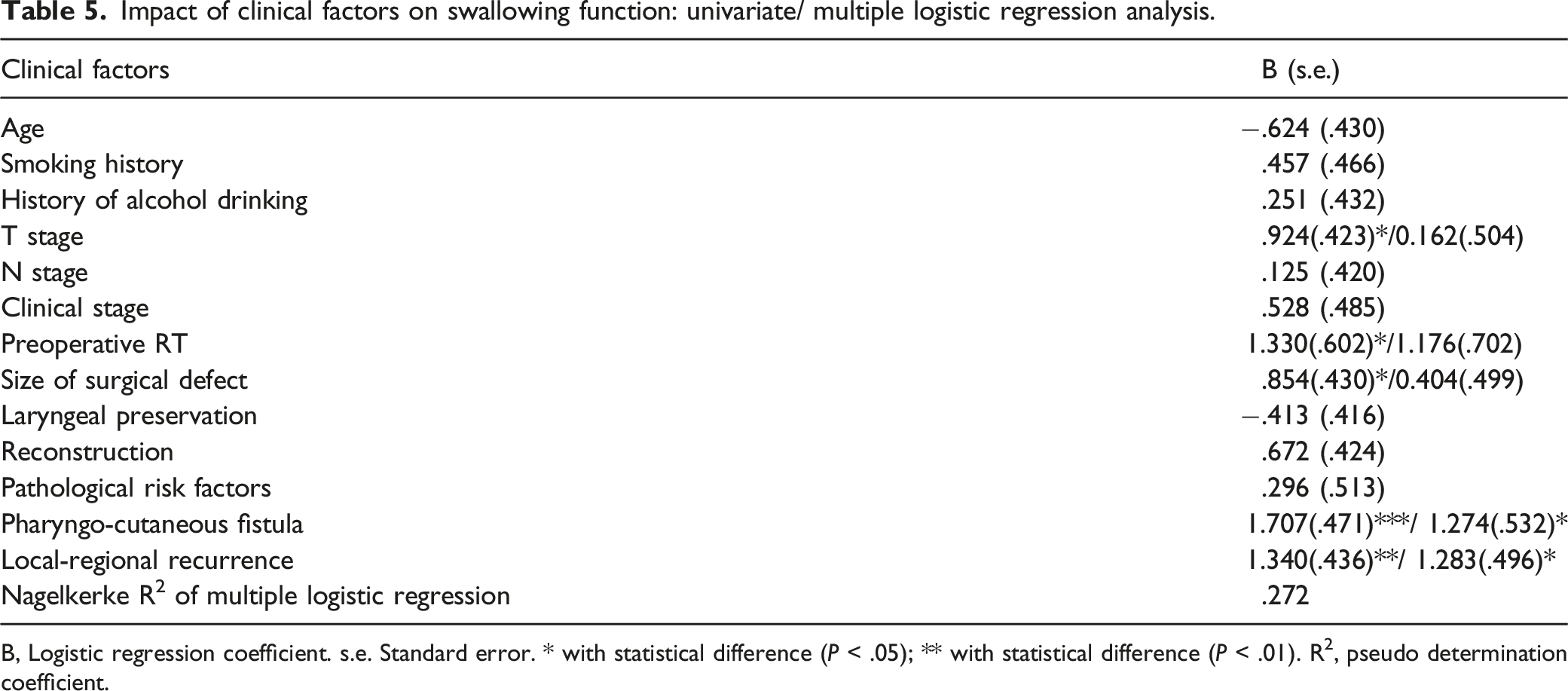
B, Logistic regression coefficient. s.e. Standard error. * with statistical difference (P < .05); ** with statistical difference (P < .01). R2, pseudo determination coefficient.
Quality of life
Impact of clinical factors on QoL: univariate/ multiple linear regression analysis.
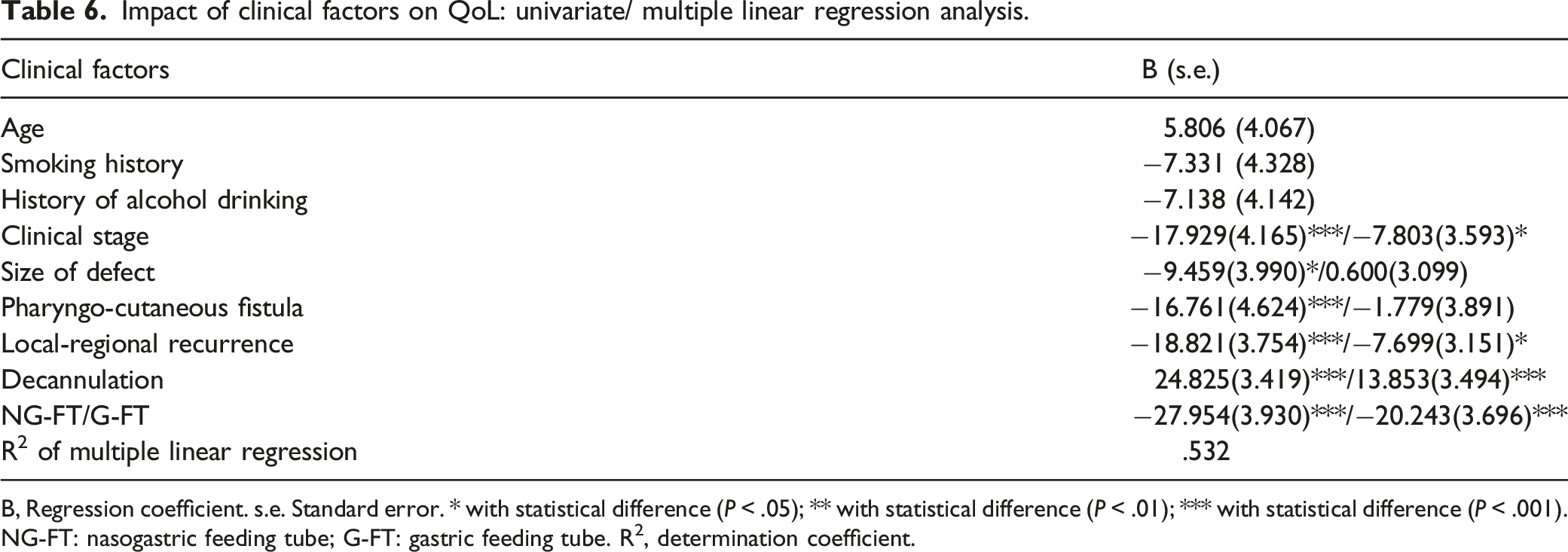
B, Regression coefficient. s.e. Standard error. * with statistical difference (P < .05); ** with statistical difference (P < .01); *** with statistical difference (P < .001). NG-FT: nasogastric feeding tube; G-FT: gastric feeding tube. R2, determination coefficient.
Discussion
HPC is one of the most aggressive cancers of the head and neck region. Treatment strategy varies according to the tumor stage and institutional experience. In China and some Asian countries, skilled surgeons prefer surgery-oriented treatment to remove the lesions completely, and the prognosis is not worse than those undergoing chemoradiotherapy.3,21 Hence, this study focused on the survival and function outcomes and the impact factors of surgery-oriented comprehensive treatment for hypopharyngeal cancer in a series of 122 patients. We hope that our findings will contribute to the treatment of the disease and improve the prognostic expectations for HPC patients.
We presented the patient demographics, individual treatment strategies, survival, and functional outcomes in the present study. The OS of patients with early-stage HPC and advanced-stage HPC were statistically significant. The results showed that the treatment outcomes of early HPC by surgery-oriented comprehensive treatment were satisfactory, while the treatment effect of advanced HPC was not, indicating that early diagnosis and treatment improved the treatment outcomes for advanced-stage HPC.
Univariate and multivariate analyses were used to identify the impact factors for OS, DFS, swallow function outcome, and QoL. The results revealed that the size of the surgical defect, local-regional recurrence, and distant metastasis were independent predictors for OS and DFS; PCF and local-regional recurrence were independent predictors for the swallowing function; and clinical stage, local-regional recurrence, decannulation, and feeding tube were independent predictors for QoL in HPC patients.
Overall swallowing performance is the most important functional outcome for a patient’s health and QoL before and after treatment. 22 In order to provide HPC patients with a chance to maintain oral swallowing, every effort was made to remove the space-occupying lesion and reconstruct a passage for food, which might include the reconstruction of the hypopharynx, oropharynx, and/or esophagus, depending on the extent of the surgical defect, after making sure of secure margins. Much of this surgical progress has been achieved by innovative surgeons using free tissue transfer, accurate placement surgery, reconstruction of neo-glottis, and perfecting the pharyngo-esophageal anastomosis. 19 Compared with non-surgical treatment,12,23–25 our surgery-oriented comprehensive treatment resulted in comparable 5 year OS, functional larynx preservation, and better swallowing function.
Based on our experience, some detailed surgical skills were helpful to preserve the swallowing function. When the hypopharyngeal defect is too large, too much mobilization of the mucosa and direct suturing will lead to too much tension on the neo-hypopharyngeal wall and postoperative PCF, which is a significant negative factor for swallowing function, as shown by our results. Defects affecting the PHPW can be closed primarily if the extent of the defect is <50%; otherwise, reconstruction is required and is best repaired by a flap. 19 Sometimes, the width of the surgical resection margin is crucial for primary closure. A wide resection margin of 2 cm, and up to 3 cm for inferior margin, has been suggested. 5 Adequate tumor extirpation, with less extensive and invasive procedures preserving unaffected normal tissue, contributes to more tumor control and less morbidity. 26 Furthermore, for the reconstruction of PHPW, relatively thin flaps (like RFFF, free jejunal patch graft, or free skin graft) can lead to better swallowing function. In contrast, thick flaps (like the pectoralis major musculocutaneous flap) will narrow the hypopharyngeal passage and dampen swallowing, possibly resulting in aspiration. 27 When pyriform sinus lesions are surgically removed, the morphological characteristics of piriform sinus can be regained by reconstruction with different flaps, which is good for the rehabilitation of swallowing function and prevention of aspiration.
Based on our results, PCF is an independent factor impacting swallowing function. Hence, its prevention and proper management are crucial for better outcomes. Comorbidity can predispose patients to PCF, including hypertension, diabetes, cardiovascular disease, hypoalbuminemia, anemia, thrombocytosis, poor nutritional status, liver disease, peripheral vascular disease, chronic obstructive pulmonary disease, and immunosuppressive medication,28–30 which should be dealt with or optimized before surgery. A review of the literature concludes a clear advantage in using vascularized tissue from outside the radiation field in the surgical defect. Some studies show a clear reduction in PCF rates, while others suggest that the fistulae are smaller and rarely need repair. 31 However, using vascularized tissues, especially those from outside the irradiated field, will definitely be more time-consuming, prolonging the operative time (>10 hours), which is independently associated with postoperative wound complications. 32 In our experience, the most important technique of closure of the hypopharyngeal surgical defect is continuous submucosal suture as the first suture line between realigned healthy residual mucosal edges or between residual mucosa and various kinds of flaps (pedicled or free). Moreover, there should be no tension on the first suture line. Furthermore, this neo-hypopharynx will be strengthened with adjacent muscles, mainly inferior pharyngeal constrictor and strap muscles, even if they have been irradiated. For us, time-saving surgical technique is preferred.
Conclusion
HPC is highly aggressive, and at present, the survival of HPC patients is not satisfactory, which is why we try our best to improve their functional outcome and QoL. Surgery-oriented comprehensive treatment can give rise to good swallowing function without jeopardizing oncological control. The size of the surgical defect, local-regional recurrence, and distant metastasis were independent factors impacting OS and DFS. Pharyngo-cutaneous fistulae and local-regional recurrence were independent factors impacting swallowing function. Clinical stage, local-regional recurrence, decannulation, and feeding tube were independent factors impacting QoL.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Key Science and Technology Program of Beijing Municipal Commission of Education [grant number KZ202110025035], Research and Development Project of Scientific Research Instruments and Equipment of Chinese Academy of Sciences-major instruments project [grant number YJKYYQ20180039] and Digestive Medical Coordinated Development Center of Beijing Municipal Administration of Hospitals [grant number XXZ0604].