
Abstract
The ingested fish bone (FB) is a common presentation for otolaryngologists in Asia. For FBs which could be identified by examinations with or without nasopharyngoscopy, direct removal would be an appropriate management. However, an ingested FB could occasionally perforate pharyngeal mucosa and migrate extraluminally. Otolaryngologists should be extremely careful while evaluation and management of extraluminal FBs to prevent life-threatening condition. In this case report, we present a patient with a parapharyngeal extraluminal FB for 2 days which was detected by computed tomography scan of the neck. A transoral endoscopic-assisted retrieval of fish bone was performed after right tonsillectomy.
Introduction
Fish bone (FB) ingestion is a common chief complaint in otolaryngologic clinic, especially in Asia. The common locations of the impacted FBs include oral cavity, palatine tonsil, tongue base, vallecula, lateral pharyngeal wall, pyriform sinus, and posterior pharyngeal wall. Initial investigations comprise oral cavity examination, flexible nasopharyngoscopy, and lateral neck radiography if cervical esophageal FB is suspected. Computed tomography (CT) examination is the image modality of choice if the initial investigations failed to identify FB and the possibility of extraluminal FB could not be excluded. We here present a case of extraluminal FB in parapharyngeal space revealed by a CT exam and is retrieved through transoral endoscopic-assisted approach under general anesthesia after unilateral tonsillectomy.
Case Report
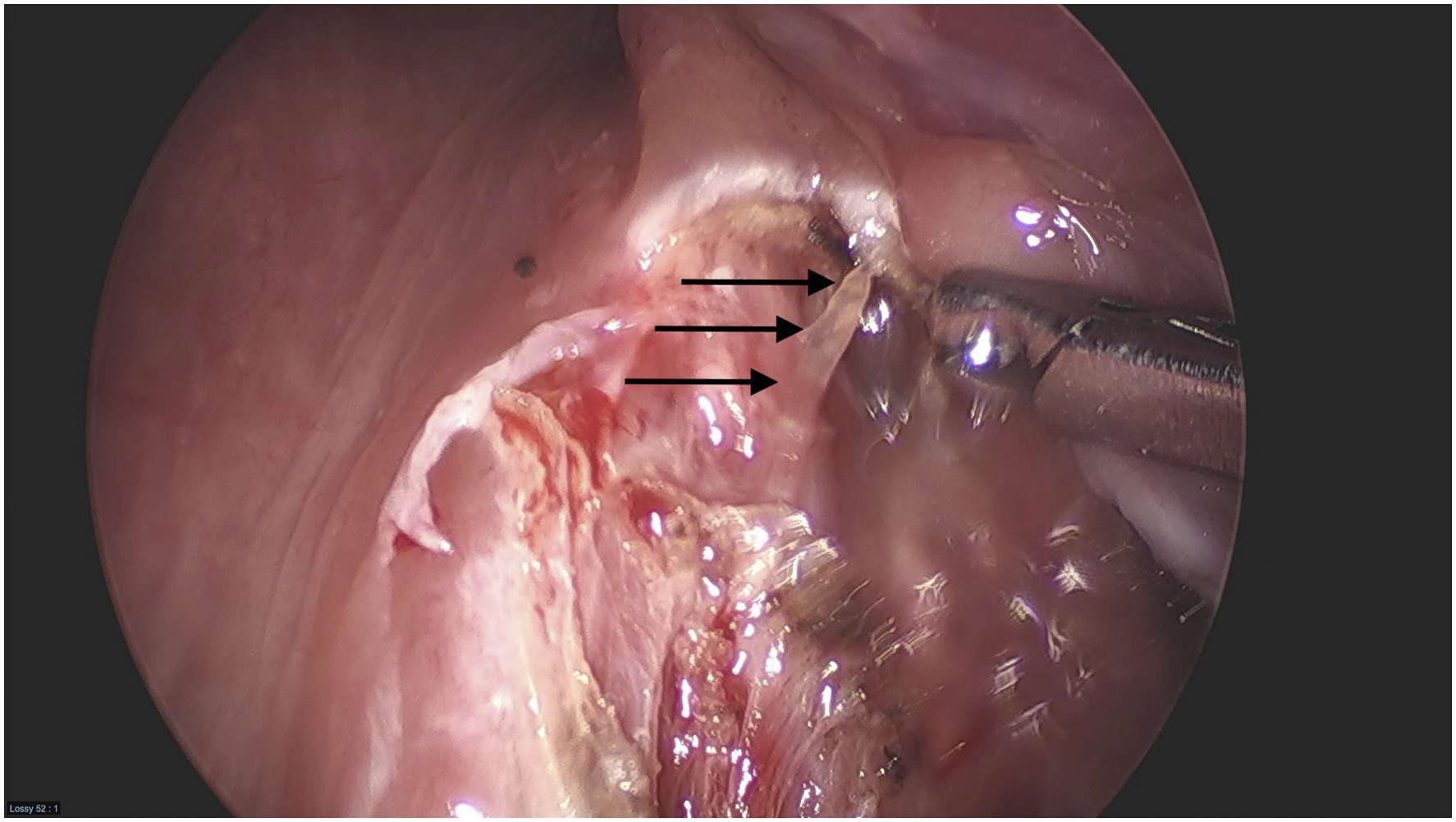
A 61-year-old woman with end-stage renal disease presented to the emergency room with a chief complaint of fish bone ingestion 2 days ago. The examination of the oral cavity, oropharynx, and hypopharynx using a flexible nasopharyngoscopy was unremarkable. Lateral neck soft-tissue radiography showed a suspected radiopaque density in pharyngeal space at C2–C3 level (Figure 1). Then a computed tomography (CT) scan of the neck was done, which showed a linear radiopaque density, around 2.2-cm in length, lateral to right palatine tonsil and deep into parapharyngeal space (Figure 2). Transoral surgical exploration began along the upper pole of tonsillar bed. Not until the completion of right tonsillectomy did the tip of the FB be identified by endoscopic-assisted blunt exploration of the tonsillar bed (Figure 3). The FB was then retrieved intact using laryngeal forceps. The patient had resolution of her symptoms after the procedure and she was discharged after 1 day with no complication. A lateral neck x-ray revealed a radiopaque density (arrow) in pharyngeal space at C2–C3 level. A coronal CT showed a radiopaque foreign body (arrow) in the right parapharyngeal space. The tip of the fish bone (arrow) is identified by endoscopic-assisted blunt exploration of the tonsillar bed.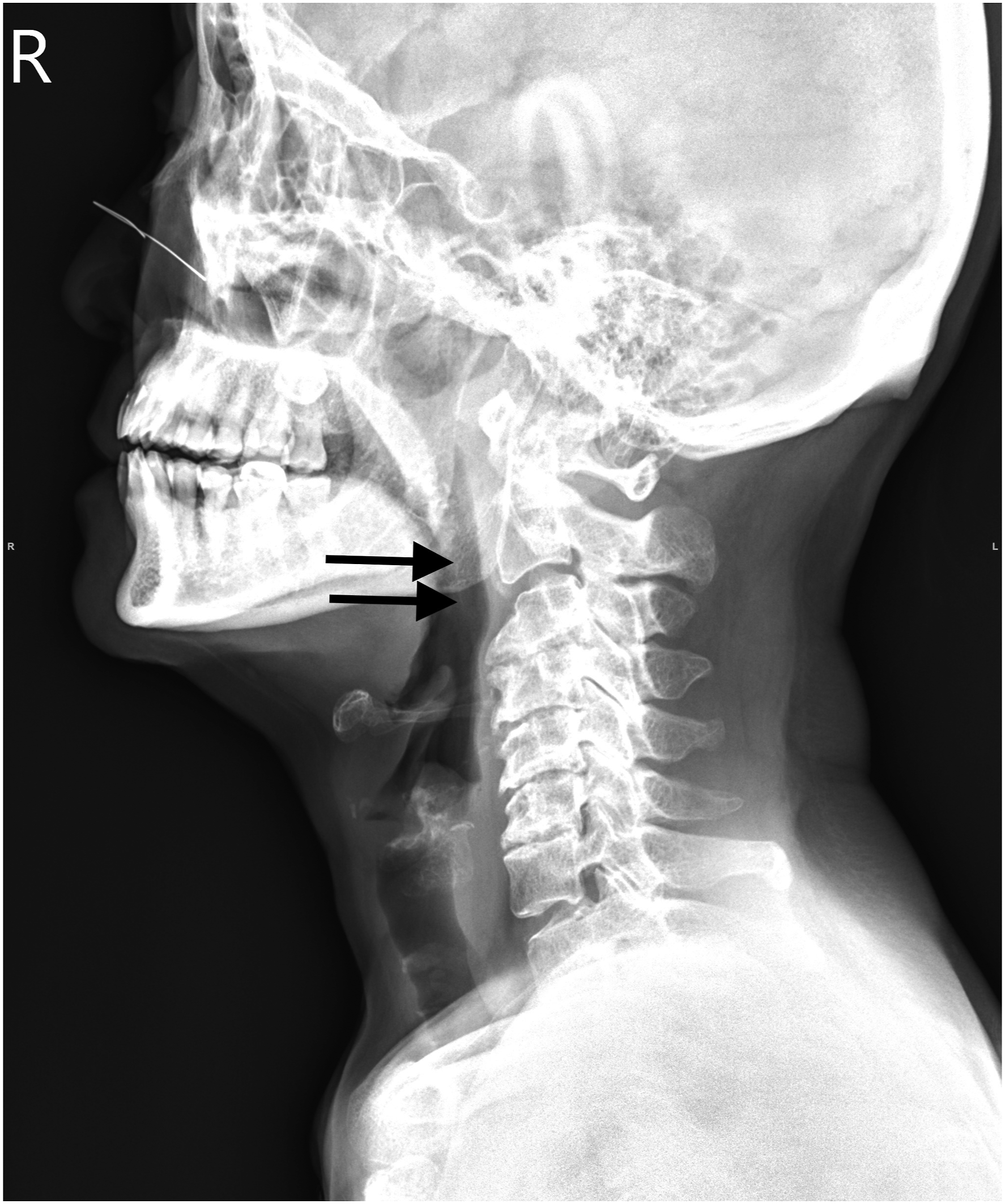

Discussion
FB is one of the most common ingested foreign bodies encountered in otolaryngologic clinics. Intraluminal ingested FB could be lodged in the oral cavity, oropharynx, hypopharynx, or cervical esophagus. On the other hand, soft tissue migration of FB, or extraluminal FB, is a rare condition and could cause serious complications. The shape and orientation of a fish bone, 1 contraction of neck muscles when neck moving, local infection of esophageal or pharyngeal wall and direct pressure necrosis, 2 contraction of cricopharyngeus muscle when swallowing, 3 and patient manipulation are all factors that may contribute to the migration of FB. The most commonly performed surgical procedure for extraluminal FB removal is surgical exploration in neck under general anesthesia with the help of ultrasonography or intraoperative X-ray. 4 According to the neck CT before the operation in this case, the FB is in the right parapharyngeal space and lateral to the right palatine tonsil. Potential ways for FB removal include transoral approach with or without tonsillectomy, or transcervical neck dissection to explore the FB in parapharyngeal space. The advantages of transoral approach are the better cosmetic outcome, the lesser vital structures which transcervical approach might encounter including the great vessels and cranial nerves of neck, and the lesser surgical procedure time. On the other hand, the potential need of right palatine tonsil sacrifice, poorer surgical field exposure, and difficult FB localization are the disadvantages of transoral approach. Share decision making was conducted after well discussion with the patient and the transoral approach was adopted. The surgical exploration was performed initially from the upper pole to the lower pole along the capsule of right palatine tonsil. The FB was identified later with the help of endoscopy after minimal surgical dissection of the loose areolar tissue lateral to the tonsillar bed. To the best of our knowledge, this is the first report of extraluminal parapharyngeal foreign body removal with transoral approach after palatine tonsillectomy. With this approach, a better cosmetic outcome, a lesser procedure time, and a safer FB removal could be achieved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.