
Abstract
The Castleman Disease (CD), also recognized as giant lymph node hyperplasia or vascular follicular lymphoid hyperplasia, is an infrequent lymphoproliferative disorder with substantial clinical variability. Parapharyngeal location of this disease is very rare and in pediatric population it is even rarer. This article presents a case of Unicentric CD (hyaline vascular type) in an 8-year-old female, where the disease was localized within the parapharyngeal space. Clinical manifestations were limited to the presence of a local mass, with no other specific symptoms observed. Laboratory assessments revealed no significant abnormalities. She underwent surgery using a cervical-parotid approach and experienced a good postoperative recovery. Histopathological analysis confirmed the diagnosis. This case underscores the need for a comprehensive evaluation and consideration of uncommon etiologies in the assessment of parapharyngeal masses, even in pediatric patients.
Introduction
Castleman disease (CD), also known as giant lymph node hyperplasia or vascular follicular lymphoid hyperplasia, was first described in a case report published by Benjamin Castleman in 1954. 1 It represents a rare category of lymphoproliferative disorders characterized by distinctive pathological alterations and significant clinical heterogeneity, with an estimated annual incidence of approximately 2 per 100,000 individuals.2,3 There may be a slight female predominance. 4 Currently, the etiology and pathogenesis of this ailment remain unclear, with emerging evidence suggesting an association with interleukin-6 (IL-6), and some cases exhibit a close correlation with HIV infection and human herpesvirus-8 (HHV-8) infection.5,6
Based on the extent of involvement, CD can be categorized into unicentric Castleman disease (UCD) and multicentric Castleman disease (MCD).5,6 Histopathologically, it can be further classified into the hyaline vascular type, plasma cell type, or mixed type.5,6 The peak incidence is often quoted to occur between the third and fourth decades for UCD and the fourth and fifth decades for MCD.4,7 Historically, most documented cases have involved adult patients, with CD in children being sparsely reported. CD can affect lymph nodes throughout the body, the head and neck region represent the second most frequently affected site in CD, following closely behind the mediastinum. Parapharyngeal location of this disease is very rare and in pediatric population it is even rarer. 8 This article presents a case of UCD located within the parapharyngeal space in a pediatric patient. By reporting this rare case, we aim to enhance understanding of this uncommon condition and reduce misdiagnosis when distinguishing it from other parapharyngeal tumors.
Case Report
An 8-year-old female was incidentally discovered with a left parapharyngeal mass during a routine MRI examination. The imaging revealed a lesion in the left parapharyngeal space that extended into the left parotid region, resulting in mild facial asymmetry and enlargement of the left parotid gland. She was otherwise asymptomatic. She had no specific medical history. Upon physical examination, there was significant enlargement of the left parotid region, measuring approximately 3 cm × 4 cm. The mass displayed firm consistency with poorly defined borders, a relatively smooth surface, limited mobility, and no tenderness or signs of skin erythema or ulceration. Oropharyngeal examination did not reveal any significant abnormalities.
Enhanced MRI findings identified an elliptical solid lesion within the left parapharyngeal space, extending into the left parotid region (Figure 1). The lesion measured approximately 41 mm × 14 mm × 24 mm in its largest cross-sectional dimensions (length × width × anteroposterior diameter). It appeared isointense on T1-weighted images (T1WI) and hyperintense on T2-weighted images (T2WI). Multiple small cystic components within the lesion ranged from 1 mm to 5 mm in diameter. Contrast-enhanced imaging revealed significant non-uniform en-hancement of the solid components, while the cystic components did not exhibit enhancement. The lesion extended medially into the parapharyngeal space and posteriorly into the deep lobe of the parotid gland, with well-defined boundaries. In the left neck region, several slightly enlarged lymph nodes were observed, with the largest measuring approximately 12 mm in diameter. These lymph nodes exhibited homogeneous signal characteristics on both non-enhanced and contrast-enhanced imaging. The radiological diagnosis suggested a lymphoproliferative disorder involving the left parapharyngeal space and parotid gland. Ultrasonographic examination revealed a uniform hypoechoic pattern within the left parapharyngeal space and deep facial aspect of the parotid gland, accompanied by punctate and linear blood flow signals. The preoperative diagnosis included a left parapharyngeal space mass and a left parotid gland mass.
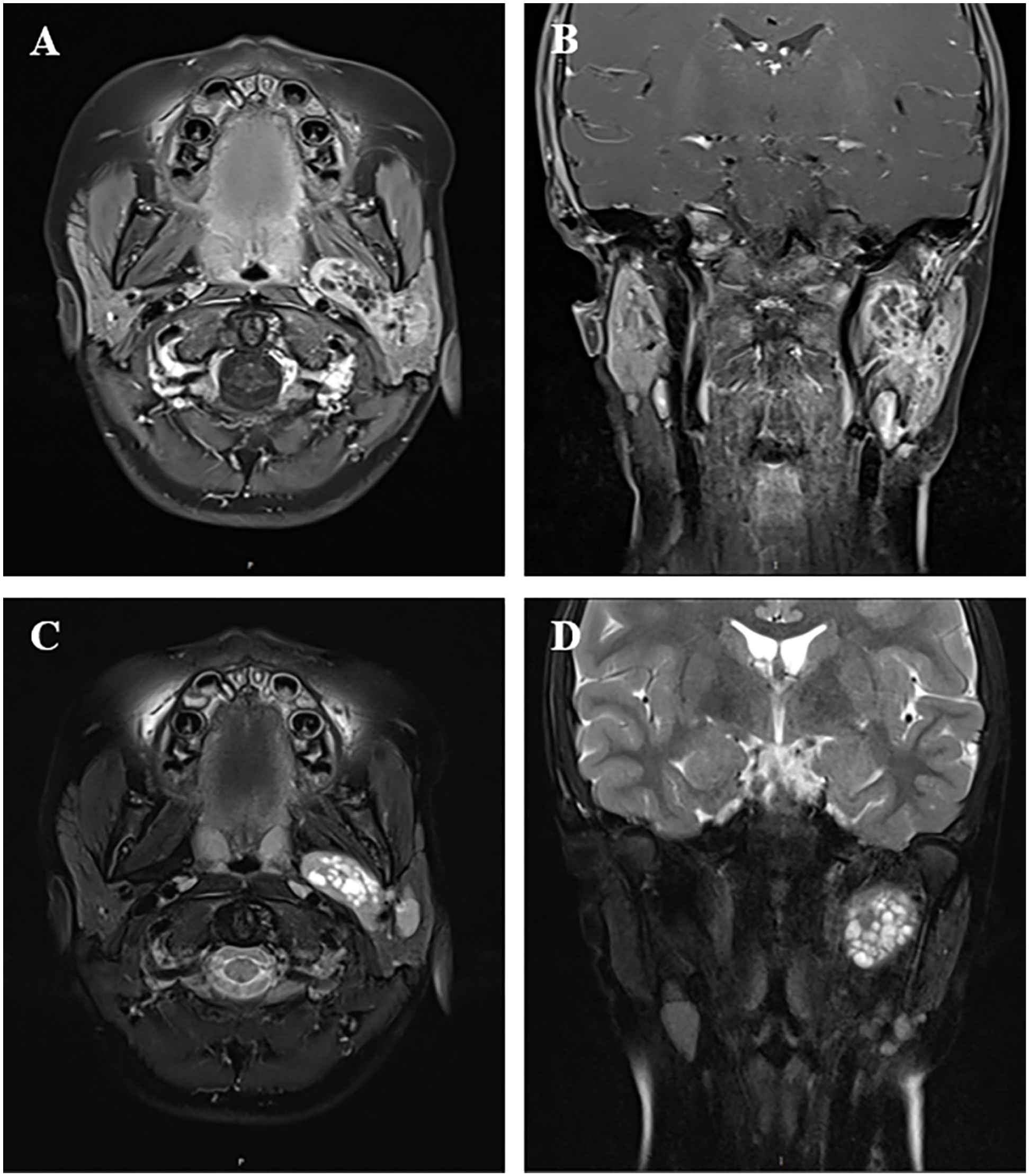
Enhanced MRI of left parapharyngeal space and parotid region. [(A) enhanced T1WI: axial view; (B) enhanced T1WI: coronal view; (C) enhanced T2WI: axial view; (D) enhanced T2WI: coronal view].
There were no significant abnormalities in laboratory-related examinations, and there was no contraindication in the preoperative examination. After informed consent, she was operated by a senior ENT surgeon using a cervical-parotid approach, which included left parapharyngeal space tumor resection, left parotid gland resection, level II neck lymph node dissection, and facial nerve dissection. During the operation, dissection of the facial nerve’s temporal branch exposed the posterior belly of the digastric and stylohyoid muscles, providing access to the parapharyngeal space tumor (Figure 2A and B). The tumor was completely excised (Figure 2C), and both the tumor and the parotid gland superficial lobe lymph nodes were subjected to frozen section pathological analysis. The intraoperative frozen section revealed lymphoproliferative disorder.
The postoperative pathology report revealed that examination of the lymph nodes from level II and the parapharyngeal space tumor demonstrated regressed germinal centers with marked interfollicular plasmacytosis, forming characteristic “onion-skin” patterns, and Increased interfollicular capillaries and nuclear fragmentation were noted (Figure 2D and E). Immunohistochemical staining revealed CD21 (expanded follicular dendritic cell network), CD23 (expanded follicular dendritic cell network), CD68 (histiocytes+), CD38 (plasma cells in the germinal center+), CD34 (interfollicular capillaries+), Ki-67 (approximately 5%+ in interfollicular areas), CD3 (paracortical T cells+), CD20 (follicular B cells+), Bcl-2 (germinal center-), Bcl-6 (germinal center+) and CD99 (+). These findings were consistent with the diagnosis of UCD (hyaline vascular type). Postoperatively, the patient presented no complications or sequelae.
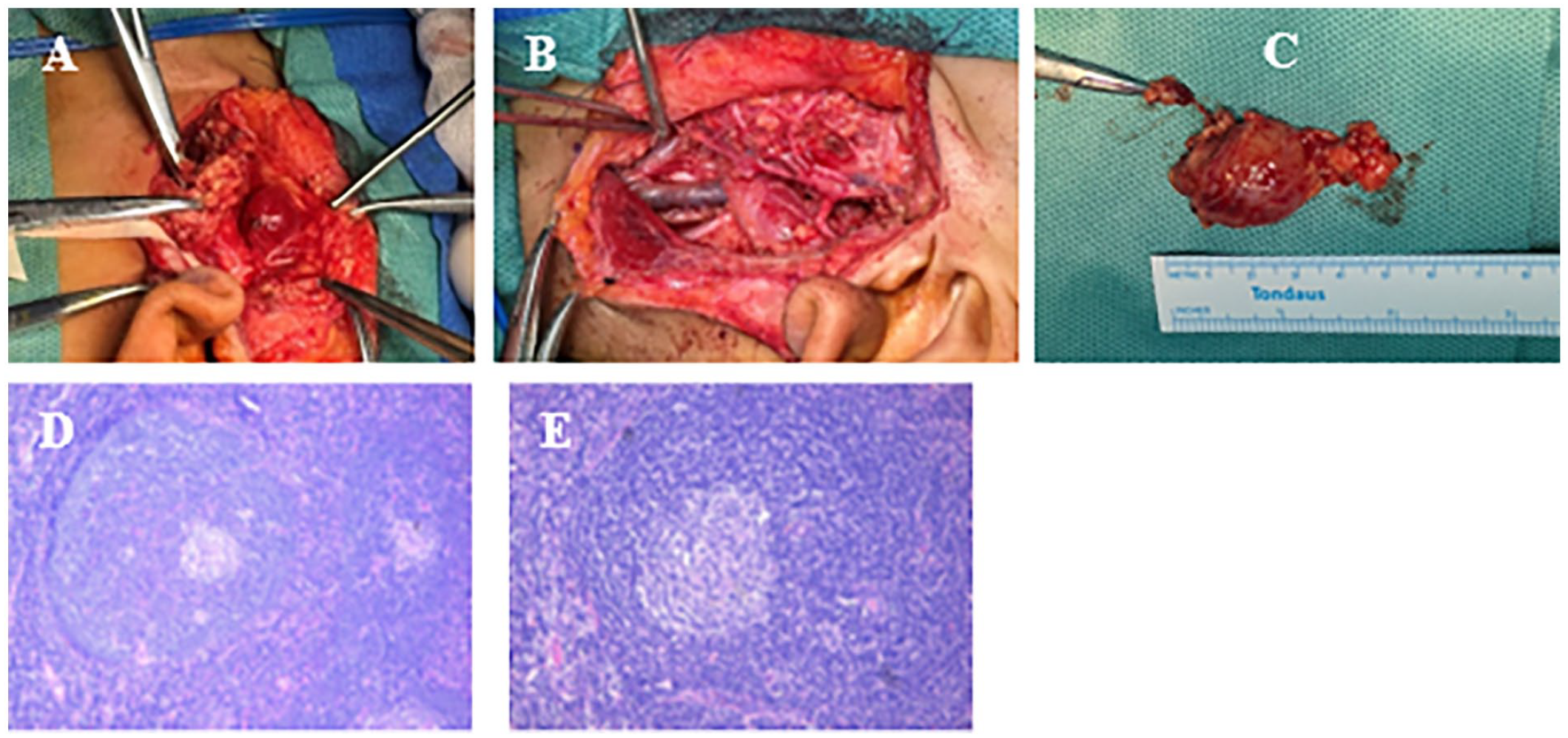
(A-C) Intraoperative pictures and specimen. (A and B) The tumor was surgically accessed via a cervical-parotid approach; (C) Excised tumor. (D and E) The pictures of pathological tissue slices. (D) H&E 10X; (E) H&E 20X.
Discussion
CD is a rare lymphoproliferative disorder characterized by lymph node enlargement. Patients with UCD often present without specific clinical symptoms, leading to potential diagnostic delays. In this particular case, the pediatric patient manifested UCD localized in the left parapharyngeal space. Clinical manifestations were limited to the presence of a local mass, with no other specific symptoms observed. Laboratory assessments revealed no significant abnormalities. She underwent surgery using a cervical-parotid ap-proach and experienced a good postoperative recovery.
CD in children is rare, and its clinical features differ from those in adults. In children, UCD is the predominant clinical subtype, and the primary histopathological subtype is the hyaline vascular type accounting for >90% of all cases.7,9 A large-scale study of pediatric CD in the United States revealed that approximately 95% (37 out of 39) of cases were UCD, and within this group of patients with UCD, all exhibited the hyaline vascular subtype. 9
CD can manifest in any lymph node, with the most common location in children being the cervical lymph nodes. In a study by Karen et al., 9 among 39 children with CD 69% were found to occur in the cervical region. Similarly, Sopfe et al. 10 reported that the most frequently affected site in 24 children with CD was the neck.
As per the majority of authors, when these masses originate in the neck, they typically reside beneath the margin of the sternocleidomastoid muscle and may exhibit a range of dimensions, spanning from small (2.0 cm) to substantial (10 cm).7,11 -13 Locations were categorized according to their neck level, with level V being the most frequently observed site, succeeded by level II, level III, and level I, while level IV was the least common. 7 In addition to the neck localization, limited documentation exists for various pediatric neck CD presentations, such as the ones located at the parotid gland14 -16 or at the submandibular gland. 17 Parapharyngeal location of this disease is very rare and in pediatric population it is even rarer. In our reported case, CD was situated within the left parapharyngeal spaces. It is important to note that the parapharyngeal spaces constitute a multifaceted anatomical region, 18 neoplasms originating in this area contribute to a mere 0.5% of all adult head and neck tumors, with even lower incidence in pediatric cases.19,20
Diagnosing CD can be a challenging task, primarily due to the fact that these tumors are often clinically asymptomatic and lack distinctive features in imaging studies. Rabinowitz et al. 7 have demonstrated that 95% of pediatric cervical CD cases manifest as either entirely asymptomatic or exhibit gradual mass enlargement, while the sole exception is a patient who presented with a painful neck mass, likely associated with compressive symptoms. Although infrequent, mass effect is rarely observed but can serve as an initial symptom in some cases.7,21
On ultrasonography, the hyaline vascular type can observe substantial blood vessels penetrating the periphery of the hyaline vascular subtype, accompanied by the presence of perforator blood flow both around and within the lesion, and the overall blood flow in this subtype appears relatively abundant.22 -24 Conversely, the plasma cell type presents a lack of vascular infiltration at the lesion’s periphery, as well as a noticeable absence of intratumoral blood flow, both at the periphery and within the lesion.22 -24 On CT imaging, UCD typically presents as a solitary soft tissue mass with uniform density, often assuming various shapes such as elliptical, renal, or dumbbell-like configurations.24,25 Notably, it frequently exhibits dendritic, radiating, and stellate calcifications, boasting well-defined borders. During the arterial phase of contrast-enhanced scans, UCD manifests a marked enhancement, which persists in the venous and delayed phases. Intriguingly, tortuous vascular structures can be discerned within or around the lesion, lending it distinctive diagnostic features. On MRI, T1WI commonly reveal signal intensities roughly equivalent to or slightly lower than that of muscle tissue, while on T2WI, the lesion typically exhibits slightly higher signal intensities. Furthermore, both arterial and delayed phase MRI scans display sustained enhancement.24,25 It is worth noting that MRI may have a lower sensitivity for detecting calcifications within the lesion, but it offers an advantage over Computed Tomography (CT) in visualizing central scarring, liquefactive necrosis, lesion margins, and other intricate aspects of the pathology. In our case, the MRI findings indicated isointensity on T1WI and hyperintensity on T2WI, with irregular and heterogeneous enhancement upon contrast administration, consistent with the magnetic resonance characteristics reported in the literature.
Considering the predominantly non-specific nature of preoperative diagnostics, the diagnosis of CD proves to be an intricate challenge in the absence of histopathological evaluation. Frequently, CD is misidentified as various other conditions, with lymphoma being the most prominent differential diagnosis. Other conditions commonly mistaken for CD encompass infectious and inflammatory lesions, such as lymphadenitis, tuberculosis, sarcoidosis, toxoplasmosis, mononucleosis, cat scratch disease, Kimura’s disease, branchial cleft cyst, and hemangioma.
Given the rarity and heterogeneity of CD, there is currently no standardized treatment approach. Surgical excision is highly effective for Unicentric CD, whether it is of the hyaline vascular or plasmacytic variant.5,26 Our case was treated with complete surgical resection of UCD with good results. When complete surgical excision is unattainable, the consideration should lean toward performing decompressive surgery or employing glucocorticoids, and monoclonal antibodies like rituximab to induce tumor regression and alleviate symptoms, followed by subsequent surgical resection. 27 In select cases, radiotherapy has demonstrated a measure of efficacy within the treatment process. 28 MCD presents a notably more challenging therapeutic scenario compared to UCD. Due to the extensive involvement of lymph nodes, surgical or radiation therapy is typically not pursued. Alternative treatment modalities encompass immunotherapy (e.g., glucocorticoids, thalidomide), targeted therapy (including siltuximab, rituximab, and tocilizumab), combination chemotherapeutic regimens (tailored to lymphoma, sarcoma, etc.), or a combination of the aforementioned strategies. 6
Conclusions
CD is a rare entity in the pediatric population, and its presentation as a parapharyngeal mass is even more uncommon. We report a rare case of UCD (hyaline vascular type), presenting as a left parapharyngeal mass in an 8-year-old female. Surgical resection and histopathological analysis confirmed the diagnosis. This case underscores the need for a comprehensive evaluation and consideration of uncommon etiologies in the assessment of parapharyngeal masses, even in pediatric patients.
Footnotes
Acknowledgements
The authors are extremely grateful for the enthusiasm and time provided by the parents and participants in this study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Shenzhen Municipal Science and Technology Innovation Committee (no. JCYJ20210324143008022) and Guangdong High-level Hospital Construction Fund Clini-cal Research Project of Shenzhen Children’s Hospital (no. LCYJ2022063).
Ethical Statement
Our institution does not require ethical approval for reporting case report.
Consent for Publication
Informed consent for publication was obtained from the patient’s parents for the use of her medical records and exam images in writing this study. All the authors have approved the manuscript and agree with submission to your esteemed journal.