
Abstract
Neck-mediastinum foreign body (FB) is a common emergency in otorhinolaryngology head and neck surgery departments, and it can be lethal. We present a case of an uncommon foreign body in the neck-mediastinum. The FB was metallic and about 12 cm long. A 74-year-old male accidentally swallowed a metallic FB that lodged in his throat for > 3 days. The intake of the object was associated with smoking a peace pipe, and was an indication for surgery. Aerodermectasia was observed in the neck upon physical examination, and a high-density foreign body was found in the neck-mediastinum through cervicothoracic computed-tomography (CT) scan. Electronic laryngoscopy showed a white pseudo-membrane adhering to the surface of the bilateral piriform fossa in the right laryngeal vestibule, and the root of the tongue, and mucosa were swollen. Cervicothoracic CT revealed dense shadows in the neck-mediastinum. However, electronic laryngoscopy showed no FB in the larynx or piriform fossa. The metal FB was removed by surgery via the parapharyngeal space approach instead of endoscopy. After preoperative assessment and preparation, we successfully removed the metal FB from the neck-mediastinum via the parapharyngeal space approach. The patient was doing well at one-month follow-up. Neck-mediastinum FB is an emergency but rare case necessitating otorhinolaryngology head and neck surgery. It can easily lead to mediastinal and lung infection; given its location in the body, it may lead to aortic arch rupture if not handled promptly.
Background
Most neck foreign bodies (FBs) occur as a result of neck injuries. FBs only rarely appear in the neck after being accidentally swallowed, 1 which can render the FB more easily trapped in the neck than in the pharyngeal. Neck-mediastinum FB can readily lead to mediastinal and lung infection and aortic arch rupture. Surgical removal is mostly required. Fragments of larger foreign bodies may become lodged in the esophagus because of swallowing. 2 However, neck FB attributable to swallowing has only rarely been reported. 3 We here report such a case of a metal FB ingested by an older man with dysphagia symptoms. It had become lodged in the neck-mediastinum.
Permission to publish this case report was obtained from the Department of Otorhinolaryngology of First People’s Hospital of Zunyi. The patient also provided informed consent for the publication of this case report.
Case presentation
A 74-year-old man was hospitalized in the Department of Otolaryngology because he had fallen while smoking a long metal pipe and had ingested part of it 3 days earlier. He did not visit a doctor promptly because he showed no symptoms. Esophageal FB was suspected because of the patient’s accompanying symptoms, which included dysphagia, pharyngeal pain, chills, inability to lie down, and difficulty speaking. However, he had no dyspnea or cough symptoms. Flexible electronic laryngoscopic examination showed no FB in the pharyngeal area, hypopharynx, or larynx and that the bilateral piriform fossa were swollen and had a white pseudo-membrane. Cervicothoracic computed-tomography (CT) scan showed a smooth, high-density FB in the right neck-mediastinum approximately 12.0 cm in length. It was located behind the trachea and esophagus, adjacent to the aortic arch, flat against the lower margin of the sixth cervical vertebrae and the fourth thoracic vertebrae, and soft-tissue pneumatosis accumulation was detectable in the bilateral parapharyngeal space, as shown in Figure 1. FB was excluded in the pharynx, larynx, trachea, bronchi, and esophagus. Preoperative cervicothoracic CT scan. (A) A smooth, high-density FB in the right neck-mediastinum approximately 12.0 cm in length; (B) Soft-tissue pneumatosis accumulation in the bilateral parapharyngeal space and neck.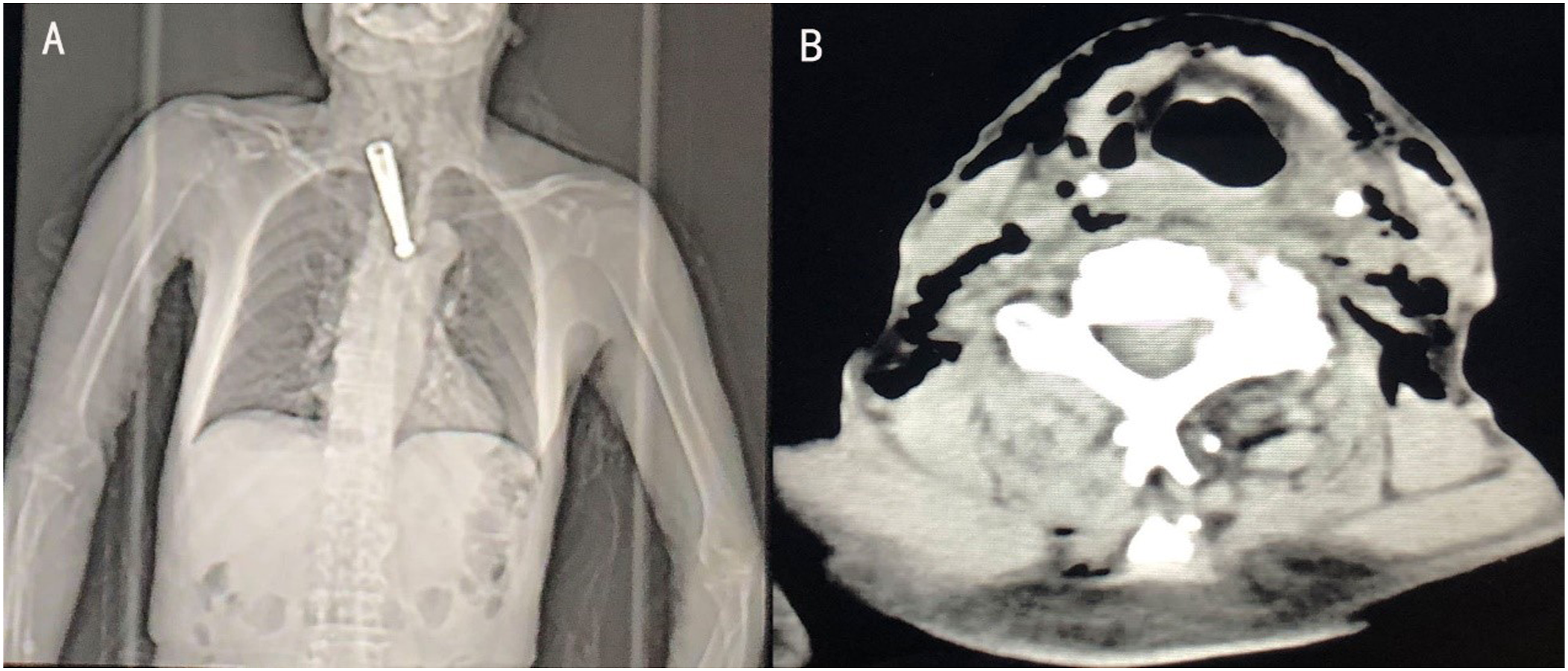
Accordingly, we diagnosed metallic FB in the right neck-mediastinum and parapharyngeal space abscess. After full discussion, a surgical plan was made: esophagoscopy followed by the removal of the FB from the right neck-mediastinum through the right parapharyngeal space. The removal of the metal FB proceeded successfully with the patient under general anesthesia (Figure 2). Intra-operative findings. (A) The FB was removed via the right parapharyngeal space; (B) The FB was approximately 12.0 cm long.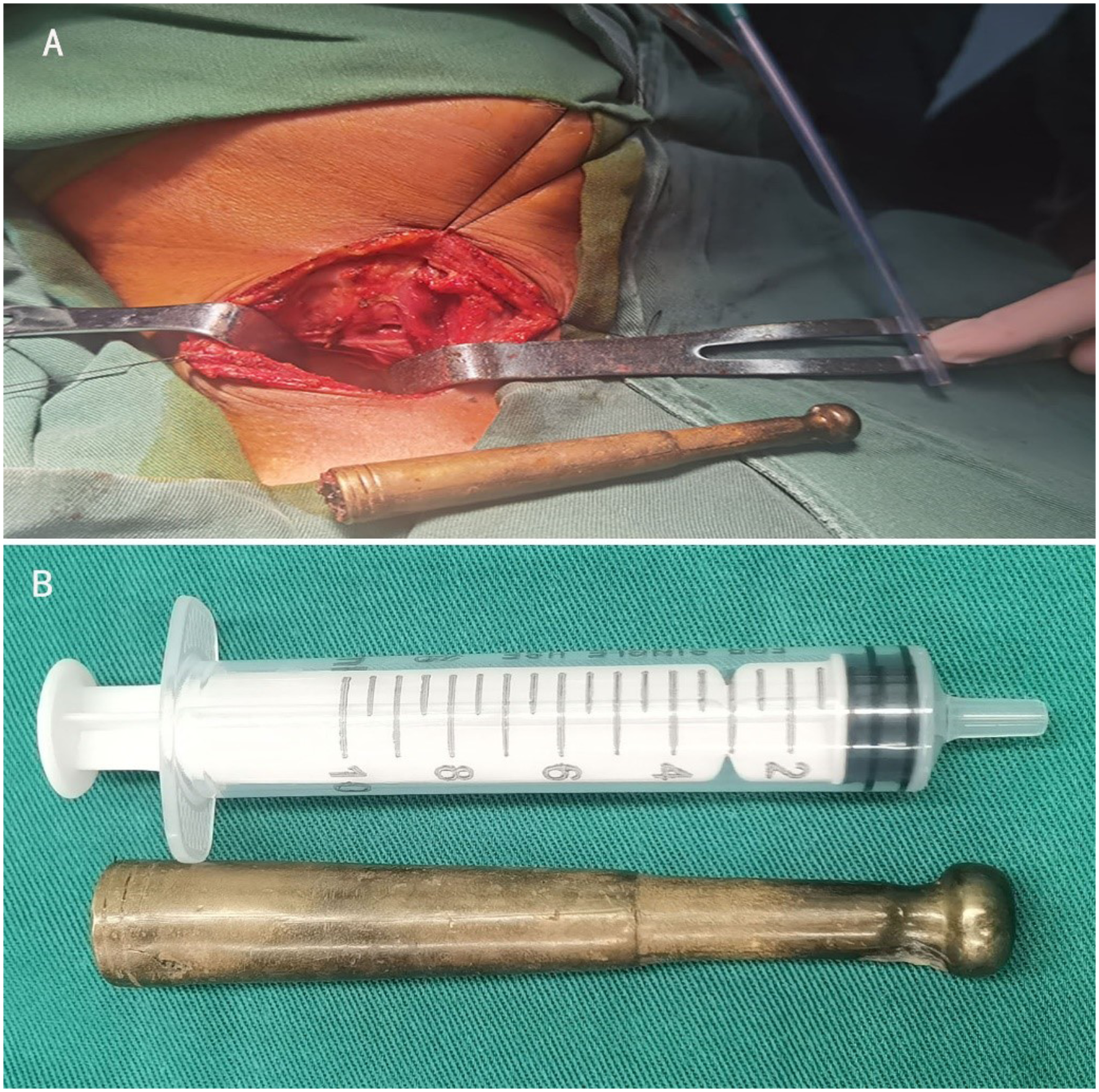
A large amount of pus was found in the right parapharyngeal space during the operation. The abscess cavity was rinsed before placement of the negative pressure drainage bottle, and the patient returned safely to the ward. The patient had no uncomfortable symptoms, and no abnormality was observed in a cervicothoracic CT scan performed a week later (Figure 3). Postoperative cervicothoracic CT scan. (A) No sign of FB in the right neck-mediastinum, (B) no abscesses or gas accumulation in the bilateral parapharyngeal space or neck, and (C) no perforation of the esophagus was found through upper gastrointestinal contrast.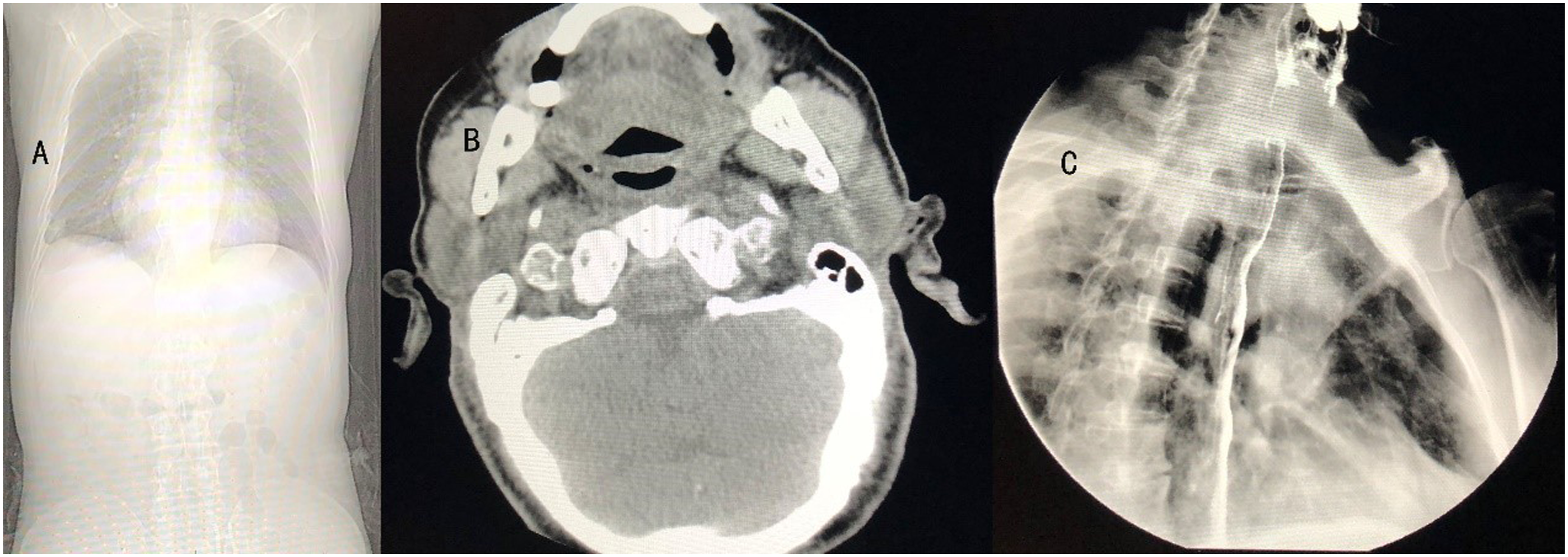
Discussion
The presence of a metal foreign body (FB) in the neck-mediastinum, although rare, is an emergency sometimes encountered in otorhinolaryngology head and neck surgery departments. It can easily cause mediastinal and lung infections if the FB is not handled promptly. It may also cause aortic arch rupture, which can endanger the patient’s life given its location. Therefore, it is necessary to remove the FB without delay. In one recent case report, mediastinal FB was removed by thoracoscopy. 4
In rare cases, pyriform sinus-impacted FB can perforate the pyriform sinus wall and migrate into the mediastinum. 4 There has been no previous report of a tobacco pipe lodged in the neck-mediastinum. Some may complain of pharyngalgia or dysphagia and speak with effort during emergency medical consultations. It was difficult to diagnose this in the patient using esophagoscopy alone. As such, immediate cervicothoracic CT was necessary.
In this case, the metal FB was a tobacco pipe that had migrated to the neck-mediastinum after ingestion. A rigid esophagoscope was proceeded preoperatively, and no positive results were found, but cervicothoracic CT scanning revealed the metal FB. A report of this sort, that is, removal of a long metal FB in the neck-mediastinum via the parapharyngeal space, is rare.
Most FBs that become lodged in either the cervical or only the mediastinal area can be seen and be removed easily. However, this is not the case for removing FBs in the neck-mediastinum. They may cause catastrophic complications because of their position as well as massive hemorrhage, dyspnea, infection, or esophageal perforation if they lodge in the aortic arch or esophagus. Therefore, it is necessary to remove FBs early and prevent neck-mediastinum FB from causing harm while the patient is walking and eating. 5
In such rare cases, multiple evaluations should be performed before surgery to select the best surgical approach.
Footnotes
Acknowledgments
Authors’ contribution
Zuxia Ma: data acquisition and analysis, drafting, and revision of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All the authors have read and approved the final version for publication, and no conflicts of interest are declared.
Funding
This study received no specific funding from any governmental, commercial, or non-profit organization.
Ethical approval
This study was approved by the ethical committees of the Third Affiliated Hospital of ZunYi Medical University/First People’s Hospital of Zunyi. There are no data available in any form for any individual person in this manuscript.
Data availability
The data used to support the findings of this study are included within the supplementary information files.