
Abstract
Hoarseness lasting greater than 2 weeks should be thoroughly evaluated. Here, a case is presented of a 38-year-old female with a 10-year history of dysphonia. Endoscopic examination confirmed the presence of a supraglottic mass, for which operative biopsy and imaging were performed. Pathology confirmed the diagnosis of supraglottic schwannoma. This was excised endoscopically with close management postoperatively to monitor for rapid recurrence and airway compromise. At one month postoperatively, the patient is still mildly dysphonic but vocally improved and the operative site continues to heal well.
Case
A 38-year-old female with no significant past medical history is referred to a laryngologist for a hoarse voice. The patient admits to being hoarse for at least 10 years but that she had noted no progression nor impact on her breathing and so further workup was not pursued. She notes that work phone calls present difficulty due to difficulty projecting and that her dysphonic voice often brings attention.
On videostroboscopy, a large supraglottic lesion was noted in the right false vocal fold, with associated effacement and compromise of the supraglottic airway (Figure 1). The lesion was fully lined with mucosa and did not appear infiltrative. The gross motion of the right vocal fold appeared to be intact but the impact of the lesion on the underlying vocal fold made assessment of true vocal fold integrity and mobility difficult. Magnetic resonance imaging of the neck confirmed the presence of a 2.3 × 1.9 cm well-circumscribed lesion of the supraglottis and the patient proceeded to operative biopsy of the lesion to establish pathologic diagnosis. Operative findings included a large mass, approximately 2 × 2 cm in size, with intact overlying mucosa. It appeared noninfiltrative, sparing the underlying true vocal fold. Pathology from the operative biopsy returned as schwannoma with S100 polyclonal positive staining. The patient subsequently underwent a complete endoscopic excision of the lesion.
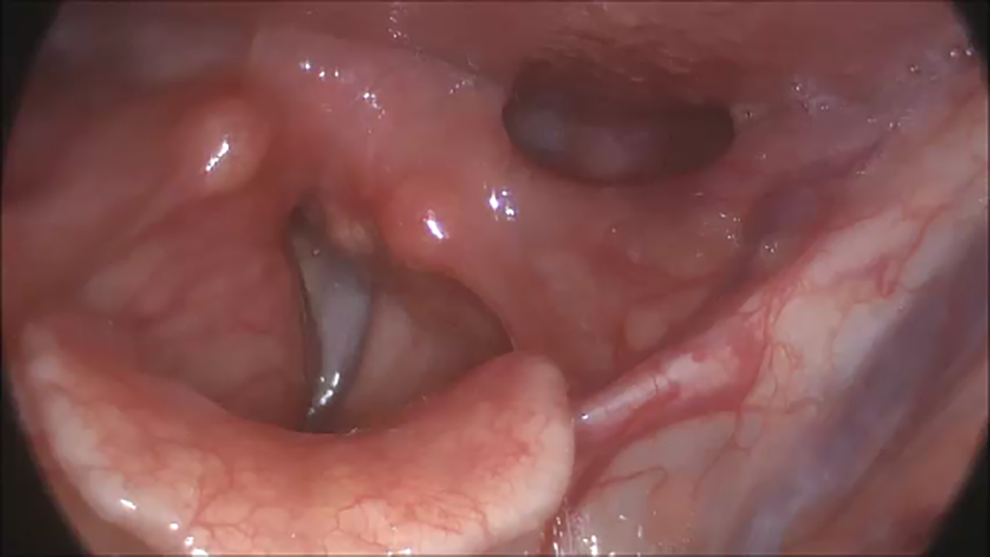
Supraglottic fullness of right false vocal fold.
One week postoperatively, the excision site was moderately to severely edematous with some evidence of granulation tissue. The voice was unchanged and she denied increasing shortness of breath. Given the indurated area of edema resulting in a mass-like effect, there was some concern for rapid recurrence, which has been reported in association with endoscopic excision when there has been incomplete resection and tumor stimulation. However, it was felt that this was more likely edema in a closed space and high-dose steroids were instituted.
The patient was closely followed and one week later was found to have significantly reduced edema. Over the subsequent month of follow-up, her voice has significantly improved with increased strength, endurance, and projection. Bilaterally normal vocal fold mobility was confirmed and there was only minimal ventricular mucosal redundancy present (Figure 2). She also notes improved exercise tolerance and decreased dyspnea.
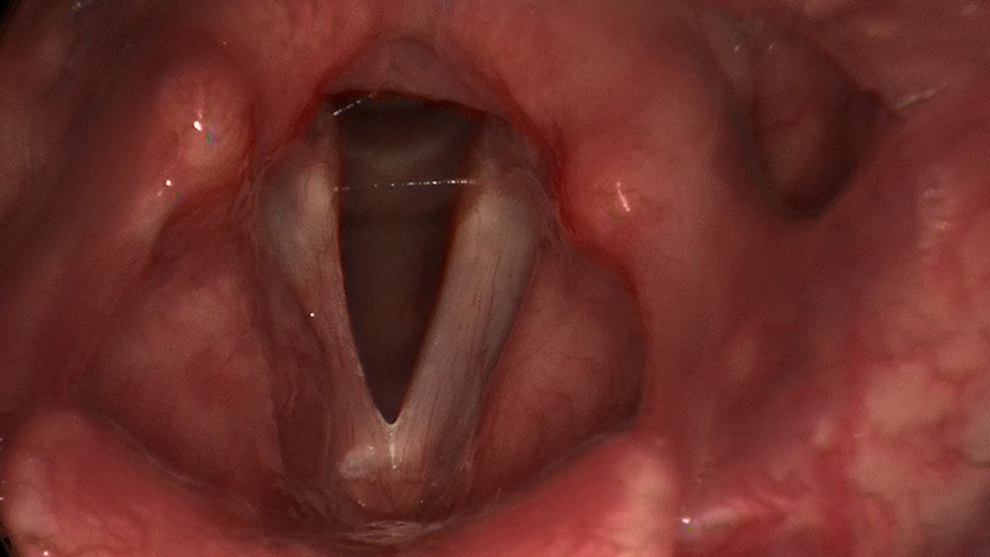
Postoperative edema of operative site.
Discussion
Hoarseness may be caused by numerous benign or malignant processes and should always be evaluated thoroughly by a laryngologist, generally utilizing videostroboscopy to elucidate etiology. This should particularly be considered in the absence of symptoms of an acute upper respiratory infection. 1,2 Subsequent findings may then navigate the course of management.
Laryngeal schwannomas, along with other neurogenic tumors of the larynx, were first described in 1925 3 and account for less than 0.1% of laryngeal neoplasms. 4 Although in this case the lesion produced only hoarseness, other presentations may include globus sensation and throat pain. 5 Diagnosis should be confirmed with tissue biopsy, and surgical excision is the preferred treatment. Given the extensive nature of this airway surgery and the potential for rapid recurrence, close monitoring postoperatively is recommended.
When these lesions are large, there may be redundant mucosa after excision. This may be managed intraoperatively by trimming mucosa but in this case, mucosa was retained to ensure adequate coverage of the supraglottis. In the current report, the patient demonstrated significant improvement in the projection and effort in her voice one month postoperatively and will continue to be monitored.
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.