
Abstract
Penetrating neck injuries are not uncommon, while penetrated foreign bodies involving the larynx are rare, which can be critical and challenging even for experienced physicians. We presented a case of a 64-year-old man with a piece of grinder blade penetrating through the subglottic region, visiting our outpatient department with hoarseness persisting for 3 weeks. The flexible fiberoptic laryngoscope, CT and direct laryngoscope were used to establish the right diagnosis. A cervical incision over the prior scar region was performed to remove the foreign body from the laryngeal box. Clinically, laryngotracheal injuries could lead to severe crisis without proper and prompt treatment. As to penetrated foreign bodies involving the larynx, a proper airway management and surgical approach are crucial for minimizing the morbidity and mortality. An accurate localization and preoperative planning is on the other hand indispensable to a successful removal and recovery.
Introduction
Penetrating neck injuries are not uncommon, usually presenting with obvious and specific traumatic history, such as gunshot or stabbing. 1 The lack of proper and prompt treatment might lead to the development of fatal consequences compromising the airway of the patient. However, incidences of penetrated foreign bodies involving the larynx are rare, and only few relevant published reports are present in the literature. The first reported case was of a child who died from sequential abscess formation in 1885. 2 The initial symptoms of penetrating neck injuries are diverse, including neck pain, emphysema, stridor, dysphagia, dyspnea, and hoarseness. 3 Herein, we present a unique case of a patient who was penetrated with a piece of grinder blade in the subglottic region, presenting to the clinic with hoarseness.
Case report
A 64-year-old man presented to our outpatient department with hoarseness, persisting for 3 weeks. He was a construction worker who accidentally injured his neck while operating a grinder three weeks prior, which bruised his neck. Initially, the wound bled a little but soon healed. However, the onset of hoarseness prompted his visit to our hospital for evaluation. No other symptoms were observed, such as fever, odynophagia, dyspnea, cough, or hemoptysis. The patient’s medical history was unremarkable, except for being a chronic carrier of viral hepatitis B and C. He was a non-smoker and social drinker.
Physical examinations detected a non-tender, 1-cm scar in the left anterior neck. A flexible fiberoptic laryngoscope revealed a protruding foreign body in the left subglottic region of the patient (Figure1A). The vocal cord was mobile and no palsy was noted. Contrast-enhanced computed tomography (CT) of the head and neck region demonstrated a solid, tubular, hyperdense, 2.5-cm foreign body in the left anterior larynx below the inferior border of the thyroid cartilage. Approximately three-fourth of the lesion was within the cervical soft tissue and only one-fourth of the mass had penetrated the subglottic region. The adjacent structures, including cartilages and thyroid vessels, were not involved and no enlarged cervical lymph nodes or subcutaneous air was present (Figure1B). The routine examinations, such as hemogram, serum urea, electrolytes, hepatic enzymes, coagulation time, and electrocardiogram, showed normal results. (A) Fiberoptic laryngoscope revealed a protruding foreign body in the left subglottic region. (B) CT demonstrated a solid, tubular, hyperdense, 2.5-cm foreign body in the left anterior larynx below the inferior border of the thyroid cartilage. Three-fourth of the lesion was within the cervical soft tissue and only one-fourth of the mass had penetrated the subglottic region. (C) The foreign body, identified as a broken piece of the grinder blade, was removed using Kelly–Rankin hemostatic forceps.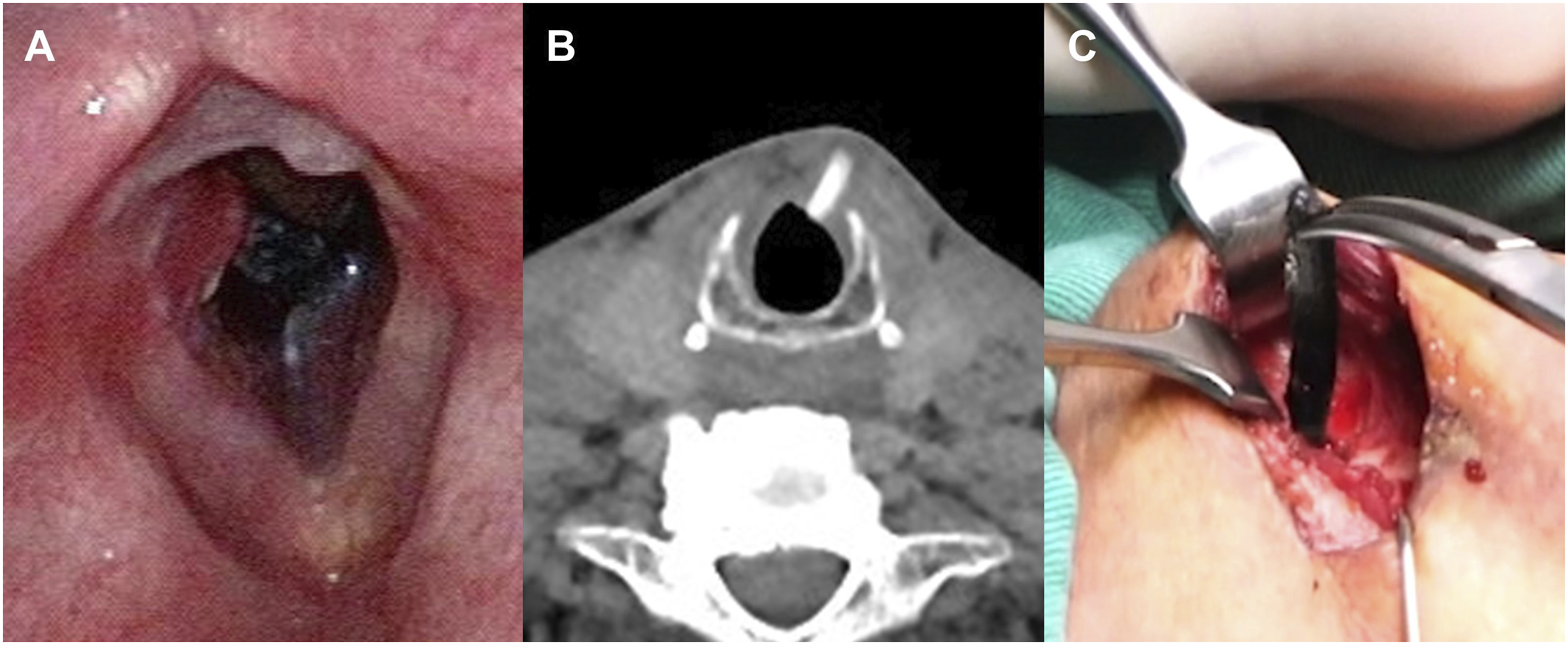
The patient was brought to the operating room for the reconfirmation of the lesion using a direct laryngoscope under general anesthesia (video). Considering that majority of the lesion lay within the cervical soft tissue, a cervical incision was made over the prior scar region. The foreign body, identified as a broken piece of the grinder blade, was located behind the strap muscles, penetrating into the larynx box through the cricothyroid ligament. The broken grinder blade was then removed using Kelly–Rankin hemostatic forceps (Figure1C). Hemostasis was carefully conducted with cauterization and the wound was closed with nylon sutures. Following the operation, the patient was afebrile and did not require nasogastric tube feeding. He was discharged with a prescription for antibiotics and painkillers the day after.
At the one-month follow-up, the postoperative wound was stable after the removal of the suture stitches. Under flexible fiberoptic laryngoscope, the subglottic wound showed recovery. The voice quality of the patient was completely restored.
Discussion
Penetrating neck injuries are complicated as up to 30% involve multiple structures, including vascular, upper respiratory, digestive, and neurological structures. 4 In a series review, penetrating laryngotracheal injuries comprised 8% of penetrating neck injuries. Excluding military experiences, the mortality rate from neck wounds was 3.7%–5.9%. 5 However, this mortality rate increased to 30% once vascular or other major anatomical structures were involved. 6 As a result, comprehensive evaluation and prompt treatment are crucial in penetrative neck injuries.
Laryngotracheal injuries due to puncture-causing foreign bodies are uncommon and can lead to significant morbidity and mortality rates. A case reported by Guo et al in 2014 showcased a 31-year-old man who was injured by a penetrating steel sliver, presenting with progressive hoarseness and dyspnea and right cricoarytenoid joint fixation due to mechanical obstruction. The sliver was removed using a rigid laryngoscope. 7
A thorough patient history check and imaging studies, including CT scan and flexible fiberoptic laryngoscopy, can help establish the right diagnosis. Further evaluation by arteriography or esophagography are required if associated structures are involved. Early mortality is greatly influenced by airway management. Patients with major laryngeal injuries usually require tracheostomy or cricothyroidotomy. According to Grewal et al, among selected patients with mild laryngotracheal injuries, endotracheal intubation did not increase the postoperative mortality or morbidity rate. 8 In our case, the airway was secured via endotracheal intubation because of the patient’s relatively stable condition, and the result was positive.
Immediate exploration and surgical intervention are essential in severe symptomatic cases. However, our case presented with trivial symptoms and had a delayed surgical removal. When it comes to surgical approaches, using transcervical, endoscopic, or bronchoscopic approach to remove the foreign body is optional.9-11 A successful removal depends on the accurate localization of the foreign body. In our case, the broken grinder blade was localized by preoperative CT scan and intraoperative direct laryngoscopy and removed via cervical incision. An external approach provides a clear identification of the involved anatomical structures and establishment of surgical drainage requirement. The treatment approach should be tailored on a case-by-case basis.
In conclusion, penetrating laryngeal injuries are rare but can be critical and challenging even for experienced physicians. A systematic evaluation, including contrast-enhanced CT and laryngoscopy, is helpful in injury localization and preoperative planning. A proper airway management and surgical approach minimizes the postoperative morbidity and mortality rate. Finally, befitting protective equipment is indispensable for workers with potentially hazardous careers.
Footnotes
Declaration of conflicting interests
The author(s) declared that there is no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.