
Abstract
Introduction:
To our knowledge, few papers have addressed preoperative evaluation of the impact of adenoid hypertrophy (AH) on the pathogenesis of eustachian tube dysfunction (ETD) in children with otitis media with effusion (OME).
Aim:
The aim of this study was 2-fold: first, to evaluate ETD using tubomanometry and Eustachian Tube Score 7 (ETS-7), in a group of children having AH; second, to assess the clinical impact of adenoidectomy on the ETD of these patients.
Methods:
Fifty patients, aged 4 to 15 years, underwent adenoidectomy based on various parameters: size of the adenoids causing canal obstruction (grades 1-4), the presence of OME, and recurrent episodes of rhinosinusitis. The function of the eustachian tube was evaluated using ETS-7 before and after surgical treatment. The patients were followed up for 6 months.
Results:
Forty children presented ETD. Of these, 36 had a grade 4 AH. The preoperative mean value for ETS-7 was 6.62. The mean postoperative ETS-7 score showed a value of 9.60 with a statistical difference compared to the preoperative value (P = .0015).
Conclusions:
Adenoid hypertrophy has a high impact on the frequency of ETD. In the patients observed in the present study, the ETS-7 score appeared to be a valid tool for assessing ETD both preoperatively and postoperatively. Adenoidectomy seemed to be effective in improving ETD as well as middle ear ventilation.
Keywords
Introduction
Otitis media with effusion (OME) is an accumulation of mucoid or serous fluid, within the middle ear (ME) cleft. It is a common, recurrent condition in children and may potentially lead to hearing loss or have a negative impact on speech development and behavior. 1
An important factor in the etiopathology of OME, according to the literature, is represented by poor function of the eustachian tube (ET). 2 Middle ear pressure (MEP) is regulated by ET openings in response to the pressure differential between the ME and the nasopharynx. In the case of eustachian tube dysfunction (ETD), pressure equalization and passive gas exchange via the mucosa in the ME may fail, leading to effusion formation. The function of the ET to open passively can be hampered by high pressures in the surrounding tissue, upper airway infections, inability of active muscular forces during swallowing, and/or nasopharynx anatomical restrictions. Regarding this last possibility, several studies in children have confirmed the existence of an association between OME and adenoid hypertrophy (AH), assuming that AH creates an obstruction of the ET orifice at the torus tubarius level, 3,4 besides repeated infections of the adenoids could cause inflammation of the ET sustaining functional impairment.
Nasal endoscopy and tympanogram are considered the current gold-standard tests for studying OME and related adenoids in clinical practice. 5,6 A careful evaluation of ETD is not routinely performed in clinical practice due to the difficulties involved in investigating this condition. The tympanogram is one of the items that reveals whether an effusion is present in the ME, providing only indirect information regarding the functionality of the ET. However, over the past years, there has been an increased interest in the diagnosis and management of ETD due to the advent of the tubomanometry (TMM) test. This relatively simple examination gives direct information regarding the patency of the ET and its dynamic ability.
The aims of this study were to evaluate ETD in a group of children having AH and to assess the clinical impact of adenoidectomy on the ETD of these patients.
Patients and Methods
Patients
Fifty children, aged 4 to 15 years, were enrolled in the study between February 2018 and December 2019 at the “Organi di Senso” Department of the Sapienza University of Rome. It was conducted in accordance with the World Medical Association Declaration of Helsinki and approved by “Sapienza” University Ethical Committee (RIF.CE: 4324).
The inclusion criteria were size of the adenoids causing choanal obstruction (grades 1-4) with involvement of torus tubarius, the presence of otitis media with or without chronic ME effusion, or chronic adhesions with poorly mobile tympanic membrane as clinical signs of ETD and/or recurrent episodes of rhinosinusitis. All children failed first-line medical treatment (antibiotics, corticosteroids) and had not undergone previous adenoid surgery. Only patients presenting symptomatology lasting from 3 months to 3 years were included.
Exclusion criteria included patients with history of drainage tube insertion or current tube insertion, craniofacial abnormalities, neuromuscular disease, genetic syndrome, recent acute infection, perforation of the tympanic membrane, previous ME and mastoid surgery, and previous rhinosinusal surgery.
All patients underwent presurgical and postsurgical ETD evaluation with Eustachian Tube Score 7 (ETS-7) score. Written informed consent for surgery and study inclusion were obtained from the parents or legal guardians of all participants.
Postoperative therapy consisted of nasal corticosteroid (budesonide 100 µg) and nasal washes (physiological solution). The follow-up period lasted 6 months.
Preoperative Evaluation
Prior to surgery, all patients underwent ENT examination (otoscopy and fiberoptic evaluation of the rhinopharynx) and tympanometry to investigate a possible OME. Tympanometry results were coded according to the Jerger system (type A, B, or C), and a type B result was interpreted as indicative of an ME effusion. 6
Adenoid hypertrophy was evaluated using nasal endoscopy (2.70-mm flexible endoscope), and patients were divided into 4 groups according to the adenoid size: 7
Group 1: choanal obstruction ratio ≤25%; group 2: choanal obstruction ratio ≤50%; group 3: choanal obstruction ratio ≤75%; and group 4: choanal obstruction ratio >75%.
Tubomanometry and ETS-7
The TMM examination was performed preoperatively in all patients in order to investigate a possible ETD. Tubomanometry is a clinical test measuring the active transport of gas from the nasopharynx to the tympanic cavity. 8,9
This method is based on simultaneously applied pressure in the nasopharynx via a nasal applicator positioned in both nostrils while a pressure receptor probe is positioned in the external auditory canal during a swallowing maneuver. Pressure changes are transmitted through movements of the tympanic membrane to the probe located in the ear canal. (Note that TMM can be performed even in the presence of a perforated tympanic membrane/ventilation tube.) 10 -12
The variable pressure curves are shown on the screen of the TMM device, and different measuring values are calculated. The opening latency index (R score) is a parameter of tube function and describes the time elapsing between pressure application in the nasopharynx and the measurement of pressure changes in the external ear canal. If the ET works correctly, during swallowing, the pressure applied to the nasopharynx is transmitted into the ME. An R score smaller or equal to 1 indicates immediate opening of the ET and a good tube function. An R score higher than 1 indicates late opening of the tube and a restricted tube function. No opening (R negative or not measurable) indicates complete obstruction of the ET 8 -12 (Table 1).
Parameters for the ETS-7 Calculation.
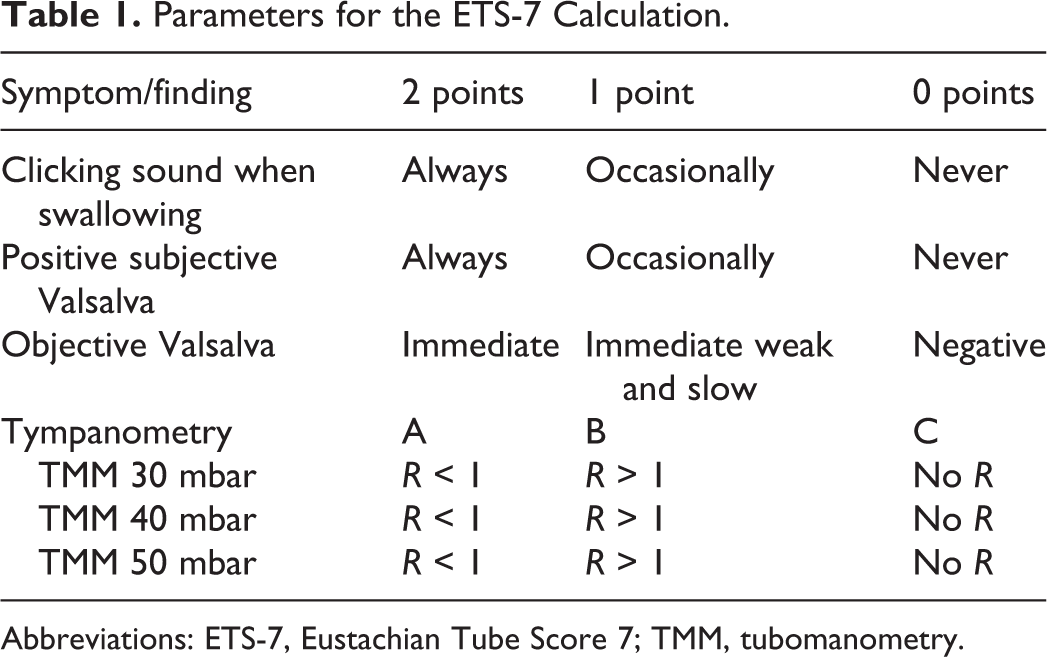
Abbreviations: ETS-7, Eustachian Tube Score 7; TMM, tubomanometry.
Only children able to answer questions and with a good compliance for performing TMM were enrolled in the study.
After TMM execution, the ETS-7 developed by Schroder et al was calculated.
An ETS-7 is a score calculated considering 4 parameters: (1) TMM measurement of the ET function at 3 pressure levels (30, 40, and 50 mbar), (2) subjective estimations concerning the feasibility of Valsalva’s symptoms, (3) subjective estimations concerning Toynbee’s clinical symptoms, and (4) tympanometry results. 11
The ETS-7 score ranges from a minimum of 0 to a maximum of 14 points, with a diagnosis of ETD with a score ≤7. 11
Adenoid Surgery
Adenoidectomy was performed in patients with adenoid tissue filling more than 75% of the choanae and covering the torus tubarius. It was also performed in patients who had a choanal obstruction ratio <75% concurrent, with a high score of subjective symptoms: recurrent infections of the upper airway more than 6 episodes in a year, the presence of otitis media with or without chronic ME effusion, or chronic adhesions with poorly mobile tympanic membrane and/or recurrent episodes of rhinosinusitis.
All patients underwent adenoidectomies through endoscopic approach using microdebrider methods 13 by one of the senior surgeons (V.S.).
Postoperative Evaluation
The same preoperative tests: fiberoptic evaluation, clinical investigation of subjective symptoms, tympanometry, and TMM in order to calculate the ETS-7, were performed 6 months after surgery in all of the patients enrolled in the study.
Statistical Analysis
The preoperative and postoperative results of ETS-7 were statistically compared using the Student t test, whereas regression analysis was used to correlate ETS-7 and AH. The P values less than .05 were considered to be statistically significant.
Results
A total of 50 Caucasian children, 29 (58%) females and 21 (42%) males, were included in this study (mean age 7.6 ± 3, mean body mass index 18.5 ± 3). They did not present comorbidities.
Clinically significant AH (group 4) was present in 36 (72%) children. Ten (20%) patients belonged to group 3. Four (8%) patients had an adenoid tissue filling less than 50% of the choanae (group 2). None belonged to group 1 (Table 2).
Characteristics of Patients.
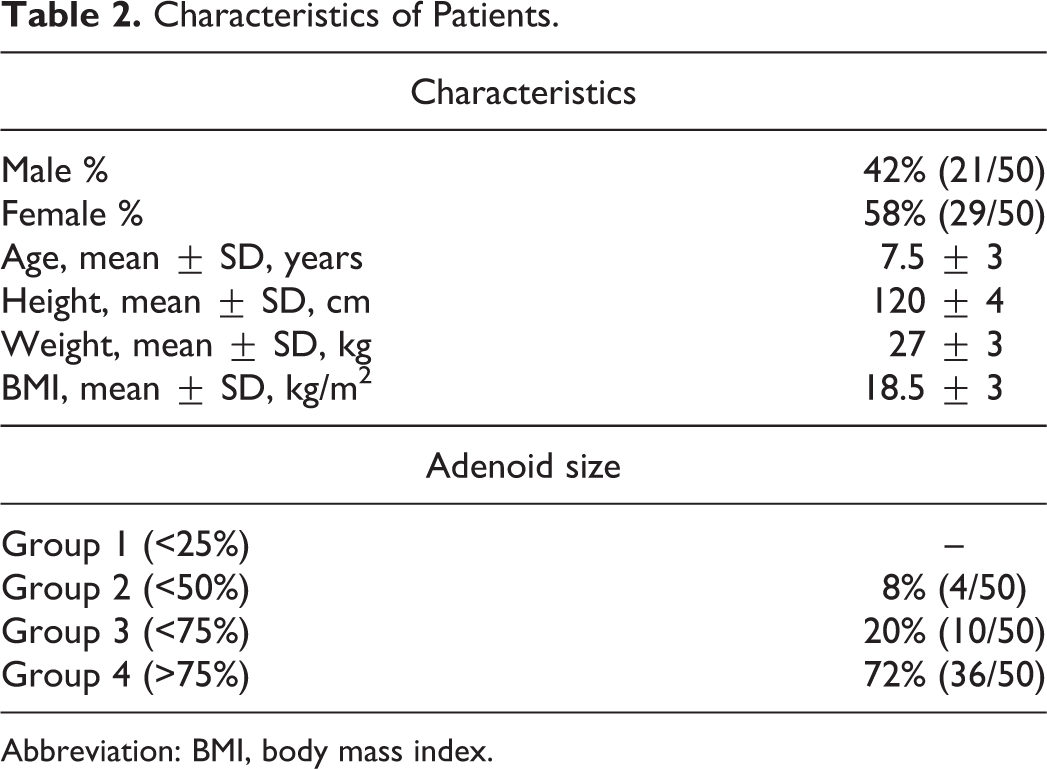
Abbreviation: BMI, body mass index.
There were no differences regarding prevalence between females and males in these 4 groups (P > .05).
Preoperative ETS-7 Results
Forty (80%) children using the ETS-7 classification showed results compatible with unilateral (26%) or bilateral (54%) ETD. Twelve children had a type B tympanometry, suggestive of OME in the preoperative stage.
A correlation between AH and ETD seemed to be present in enrolled patients. Of the 40 children who presented abnormal values on ETS-7 score, 31 presented adenoid tissue filling more than 75% of the choanae. Linear regression analysis confirmed this observation (P = .0002; Figure 1).
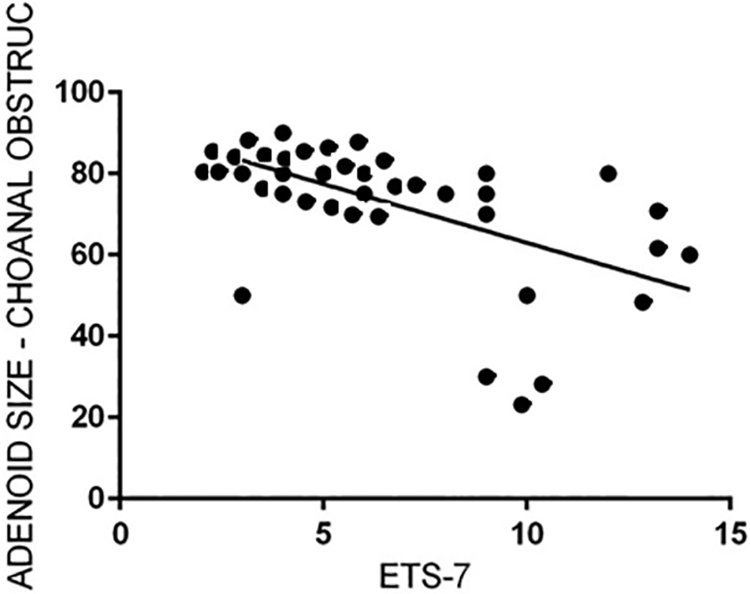
Linear regression between adenoid size and preoperative Eustachian Tube Score 7 score.
Postoperative ETS-7 Results
The mean postoperative ETS-7 score of all patients showed a value of 9.60 with a significant statistically difference with the 6.62 preoperative value (P = .0015). Postoperatively, 17 of 50 children (34%; 10 bilateral and 7 unilateral) still had an altered ETS-7 score.
Postoperatively, 6 children had a type B tympanogram.
Of 40 children with preoperative ETD, 27 (67.5%) had a significant improvement postoperatively. In detail, 20 of 27 children with bilateral ETD passed from an average score of 5.1 ± 0.8 to an average score of 11.8 ± 2.1 (P < .05). It is interesting to note that 17 (85%) of these 20 patients belonged to group 4 of the AH classification. The other 7 children presented a unilateral improvement (average ETS-7 presurgery 4 ± 1.1; average ETS postsurgery 10 ± 2.9; P < .05; Tables 2 and 3). The comparison between presurgical and postsurgical values showed a significant statistically difference (P < .05).
Pre-/postsurgical values and association with choanal obstruction are reported in Table 3.
Preoperative and Postoperative ETS-7 Score and Adenoid Size.
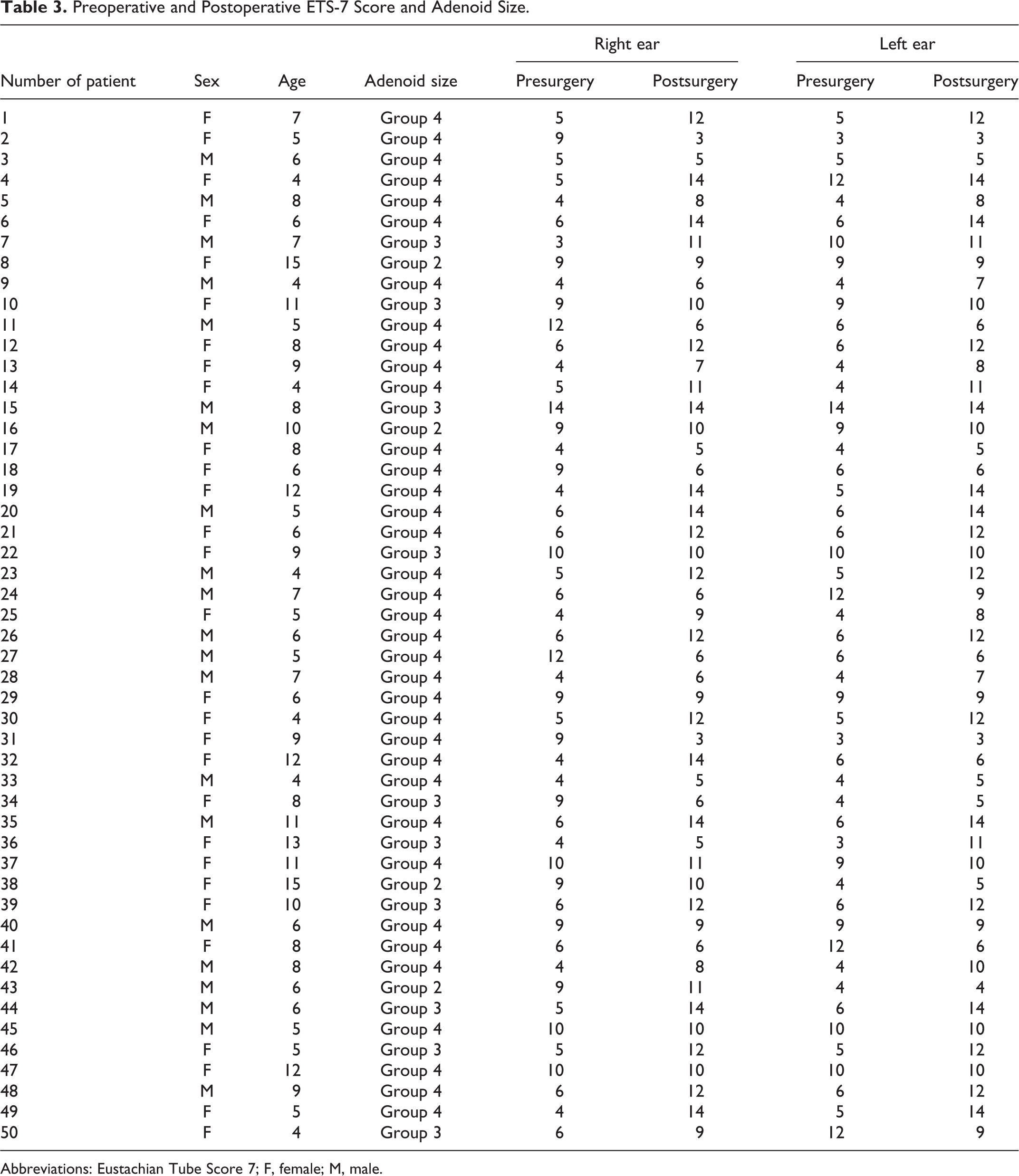
Abbreviations: Eustachian Tube Score 7; F, female; M, male.
Discussion
The potential obstruction of the ET orifice by hypertrophic adenoid tissue is a well-known risk factor for the development of ETD and OME in children. 2,6 Anatomical blockage does not allow passive gas exchange in the ME through the ET. Several authors have attempted to demonstrate the relationship between OME and AH due to ET blockage. 14,15 In particular, Wright et al 16 reported a direct correlation between lateral adenoid encroachment on the ET orifice and OME. Indirect evidence of ET blockage due to AH was also reported by Skoloudik et al. They demonstrated that adenoidectomy was efficacious for OME resolution in 89% of children with adenoids in contact with the torus tubarius, whereas it was efficacious in only 68% of children with small adenoids not in contact with the ET orifice. 17
Unfortunately, all the published studies evaluating tubal dysfunction in children with AH are indirect. This is due to the difficulties involved in performing a careful evaluation of ETD deriving from the poor efficacy of conventional methods for evaluating ET function. In particular, the tympanogram only reveals whether an effusion in the ME is present, providing only indirect information about the functionality of the ET. Moreover, the Valsalva maneuver, Toynbee maneuver, and endoscopic evaluation present difficulties for quantification. 18 However, in the past years, interest in diagnosis and management of ETD has increased due to the advent of a new procedure called tubomanometry (TMM). This relatively simple examination gives direct information about the patency of the ET and its dynamic abilities in the passage of air from the nasopharynx to the ME.
Liu et al reported their results using TMM for evaluating ET opening in adults with OME. Their results showed that the rates of restricted opening or blocked ET under pressures of 30, 40, and 50 mbar by TMM testing were 10%, 5%, and 0%, respectively (control group) and 76.19%, 66.7%, and 57.97%, respectively (OME group; Ps < .05 for all pressure groups). Tubomanometry was found to be more reliable than isolated tympanometry in the diagnosis of ETD. 19
The efficacy of TMM in predicting ETD has been confirmed by other authors. 8 -12,20 Moreover, in their study using this device, Zhang et al 18 showed that the TMM score is an associated factor for medication outcomes in adult with acute OME.
Together with TMM, the ETS-7 score has been proposed by Schroder et al 11 for increasing the accuracy of ETD diagnosis. This score has been used in several studies for the diagnosis of ETD in adults, with an estimated sensitivity of 73% and a specificity of 60%: It consists of a simple score based mainly on TMM results that can be easily performed in children too. 8 -12,20
In the present study, TMM and the ETS-7 score were used in order to evaluate ETD in children with AH.
To our knowledge, to date, there are no published papers that have studied the ET function of children with AH using TMM and ETS-7. Lai et al 21 used acoustic rhinomanometry as a preoperative management for evaluating nasopharyngeal obstruction in children with OME and AH. However, acoustic rhinomanometry does not give any information regarding whether ET function and other factors, such as turbinate hypertrophy, could determine a nasal obstruction and pathological values.
Furthermore, it is well known that ETD may be classified in 2 specific groups (obstructive and patulous ET) and that no validated test exists to differentiate these 2 different etiopathogenetic forms.
Thus, our aim was to study a homogenous population that presented the most frequent cause of ETD in children: AH. We found a high incidence of ETD in children with AH: 40 (80%) children presented with unilateral or bilateral ETD using the ETS-7 estimation, with a statistically significant linear regression. This latter is an expression of a possible relationship between the size of adenoids and the low values in ETS-7 score.
As reported by different authors, adenoidectomy could improve ME ventilation and fluid drainage by improving of ET function. 22,23 Our study seems to confirm these results with a postoperative improvement of ET function after adenoidectomy. In fact, 85% of children with bilateral preoperative EDT, who presented bilateral normal values of ETS-7 after adenoidectomy, belonged to group 4 of the AH classification.
At a mean follow-up of 6 months postsurgery, 17 (34%) children had a pathological ETS-7 score with 10 bilateral and 7 unilateral cases, with a statistical difference in ETD incidence (P = .003). Moreover, the mean postoperative ETS-7 score increased to a value of 9.6 with a statistical difference from the preoperative value (P = .0015).
Moreover, 6-month follow-up showed that there was an improvement in the quality of life of all patients, basing on the absence of new episodes of OME, especially for those who had an improvement of ETS-7 score after surgery. Furthermore, 5 of the patients with persistence of abnormal postoperative ETS-7 values reported a medical history of laryngopharyngeal reflux. 24,25
One of the most important limitations of this study was that the small number of patients included in the study (50 children) might have decreased the scientific arbitration. Another element of limitation is that in this study, patients ranging from 4 to 15 years are compared with quite different anatomical conditions. In fact, it is a common notion that younger than 6 years, the incidence of otitis media is considerably higher due to the immaturity of the ET and has a different anatomical orientation compared to that of later ages.
A multicenter study with a large number of patients is essential in order to confirm our findings and conclusions.
Conclusion
Children with AH have a high incidence of ETD measured with TMM and ETS-7. In these patients, the ETS-7 could be considered a tool for assessment in the preoperative and postoperative evaluation of the ETD. Adenoidectomy seemed to be effective in improving ME ventilation.
Footnotes
Authors’ Note
Giuseppe Magliulo made a substantial contribution to the concept or design of the work; Benedetta Pasquariello and Giannicola Iannella did acquisition, analysis, and interpretation; Alessandra Manno contributed to acquisition, analysis and interpretation of data and drafted the article; Annalisa Pace and Valeria Rossetti revised critically for important intellectual content and approved the version to be published; Vincenzo Savastano, Tommaso Vittori, and Serena Bertin approved the version to be published. All authors have participated sufficiently in the work and take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.