
Abstract
Objectives:
To analyze the role of factors that influence adenoid-related symptoms, and the influence of 3 months of isolation in preschool children who were qualified for adenoidectomy.
Methods:
This was a cohort study of the impact of 3 months of isolation on children aged 3 to 6 years with adenoid-related symptoms and endoscopically confirmed grade II and III adenoid hypertrophy. The children had previously qualified for adenoidectomy. After 3 months, 141 children were asked about their symptoms, 71 of whom were randomly chosen for medical examination, including endoscopic adenoid examination. Additionally, pre- and post-isolation tympanometry results were analyzed.
Results:
In our study, significant or mild improvements in health were observed in approximately 73% of the children; 92% of the surveyed parents reported that their children exhibited improved nasal patency, 63% of children discontinued snoring, and 30% of children showed a decrease in snoring. Data collected through surveys correlated with endoscopic findings wherein the size of the adenoid decreased by an average of 5.4%, but the amount of mucus covering the adenoid decreased more significantly in 76% of patients, which may be the main problem determining symptoms reported before isolation. In addition, the amount of residual mucus in the nasopharynx significantly affected the middle ear effusion in adenoid hypertrophy.
Conclusions and Relevance:
This study found that isolation in preschool children stabilizes the bacterial microbiome of the nose and nasopharynx, thereby having a significant effect not only on the number of recurrent infections of the upper respiratory tract but also on the patency of the nose. The only symptom that depended on the size of the pharyngeal tonsil hypertrophy was snoring. There was a weak correlation between prevalence of infections and adenoid size. During the isolation period, the adenoid size reduced by approximately 5.4% only, statistically more significant in the group with grade III adenoid hypertrophy, but the prevalence of infections rapidly decreased. Residual mucous in the nasopharynx found to be in correlation with middle ear effusion.
Introduction
In 1661, Conrad Victor Schneider first discovered and described a prominent nasopharyngeal structure as follows: “a whitish color, the adjoining membranes being bloody or dusky. It is fuller than they and like fat. It is always moist and exudes a glutinous substance.” 1 Hans Wilhelm Meyer coined the name “adenoid” in 1868. Many physicians began to study the role of this nasopharynx structure in the pathogenesis of upper respiratory tract diseases in children. This commenced an era of the diagnosis of overgrown tonsils and development of surgical removal techniques as a treatment for snoring and sleep disturbances, mouth breathing, gasping, open mouth posture, dry mouth, halitosis, hyponasal speech, and nasal obstruction with or without rhinorrhea in young children. Additionally, in 1842, James Yearsley found a relationship between pharyngeal tonsil hypertrophy and otitis. 2
Since then, the adenoid has also been considered a source of mucus and runny nose. This secretion also contains commensal and pathological microbes. The concept of commensalism as a biological association between 2 species was theorized in the 1860s by Pierre-Joseph Van Beneden. 3 A few decades later, nasal swab bacteriology cultivation and analysis was introduced. The important role of biofilms, organized structures of microorganisms in human pathogenesis, has been known and investigated since the 1980s. In 2003, Matthew Parsec proposed criteria for biofilm infection in the respiratory tract and indicated its importance in recurrent upper respiratory tract diseases in children. 4,5 James Coticchia indicated the role of biofilms covering the adenoid in pediatric chronic rhinosinusitis (CRS), which led to adenoidectomy as a treatment for pediatric CRS. 6
Currently, 4 or more incidences of recurrent purulent rhinorrhea, nasal obstruction, or otitis media with effusion in children ≥4 years lead to the suspicion of adenoiditis. 7 Indications for treatment may be established based on medical history and physical examination, which confirm adenoid hypertrophy. The appropriate diagnosis should be based on a flexible endoscopic examination, and not on radiographic assessment. 8 Adenoidectomy is recommended in cases of persistent symptoms despite pharmacological therapy and sleep disturbances with nasal airway obstruction persisting for at least 3 months. However, there remains a question: Is adenoid hypertrophy an indication for adenoidectomy?
Many doctors observe a decrease in the rate of upper respiratory infections if parents attempt to isolate their preschool children, keeping them at home and not sending them to kindergarten. However, until now, there has been no relevant study or opportunity to allow all children to remain at home. Is it not a problem of civilization and its related excessive social contacts that do not allow for maturation of the immune system and excessive stimulation of Waldeyer’s ring? Alternatively, is there no stability of the adenoid microbiome?
The coronavirus disease (COVID-19) pandemic forced the governments of many countries to order citizens to remain at home. In Poland, the period of isolation was 3 months. We analyzed the symptoms and ailments in isolated preschool children who were qualified for adenoidectomy before the pandemic.
Patients and Methods
We analyzed 141 preschool children aged 3 to 6 years who would qualify for adenoidectomy based on the reported ailments. All children had recurrent purulent rhinorrhea: 4 or more incidents of nasal blockage, snoring, and mouth breathing in the previous 12 months. There were no improvements after 3 months of treatment. Flexible endoscopic examinations were performed by one pediatric otorhinolaryngologist doctor with 15 years of experience using the Karl Storz Tele Pack endoscopic system before isolation. All recorded videos of the nasopharynx, acquired while maintaining the endoscope in a stable position until the child relaxed the soft palate, were coded and blindly analyzed by a second doctor to assign the grade of adenoid hypertrophy based on the classification described by Boleslavská et al 9 : grade I, adenoid tissue filling less than one-third of the vertical portion of the choanae; grade II, adenoid tissue filling between one-third and two-thirds of the choanae; and grade III, adenoid tissue filling more than two-thirds of the choanae.
We excluded children with a grade I adenoid size. The children were divided into 2 groups depending on the degree of adenoid hypertrophy: II and III. After 3 months of isolation, the parents were asked to complete a survey concerning previously reported and unresolved ailments, and comparisons of the symptoms were made.
Additionally, a total of 71 randomly selected children from both groups were medically examined, and resolution of adenoiditis was endoscopically confirmed after 3 months of isolation. The size of the adenoid recorded on the Tele Pack endoscopic system was randomly compared with that in a previously recorded video by a second experienced doctor. The percentages of obturation of the choanae were compared based on video endoscopy with the freeze frame option. Mucous coverage of the adenoid was also analyzed and categorized among 4 stages: (1) no mucus, (2) remnants of mucus, (3) some mucus, and (4) abundant thick mucus.
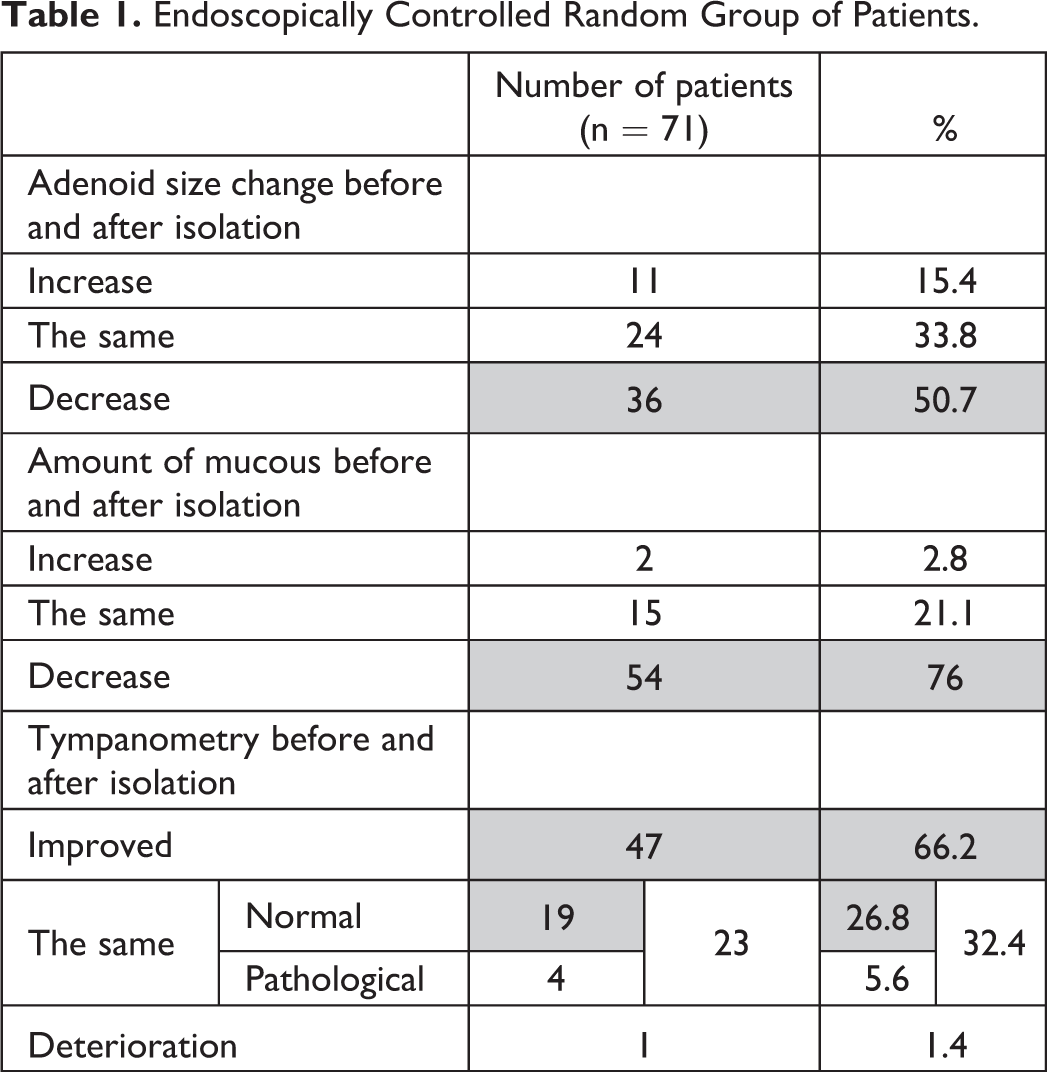
During each visit, we performed tympanometry using the Grason-Stadler GSI 39 screening device and related the results with those of tympanometry performed before isolation (Table 1).
Endoscopically Controlled Random Group of Patients.
Statistical Analysis
The purpose of this study was to assess the effect of adenoid size on the incidence of ailments: infections, nasal patency, and snoring. The H0 was no difference, and we attempted to verify this hypothesis using Pearson χ2 test at the significance level α = .05. Based on the responses to the survey, the empirical values of the χ2 test and the corresponding P values were calculated. The obtained values allowed for the inference to accept or reject H0.
Results
In both groups of children with different levels of adenoid hypertrophy maintained at 3 months of isolation, significant or mild improvements in health were observed in approximately 73% of the children. No statistical significance (P = .117) was observed in either group. The number of infections decreased by 83% and 90% in the grade II and III hypertrophy groups, respectively (P = .253). More than 90% of children in both groups showed improvements in nasal patency during this period of isolation, and 65% of the children in group I and 45% of the children in the second group stopped snoring, while it decreased in approximately 30% of children in both groups. Snoring remained at the same level in 18% of children in the grade III hypertrophy group, which was statistically significant (P = .017; Table 2).
Statistical Analysis of the Surveys.
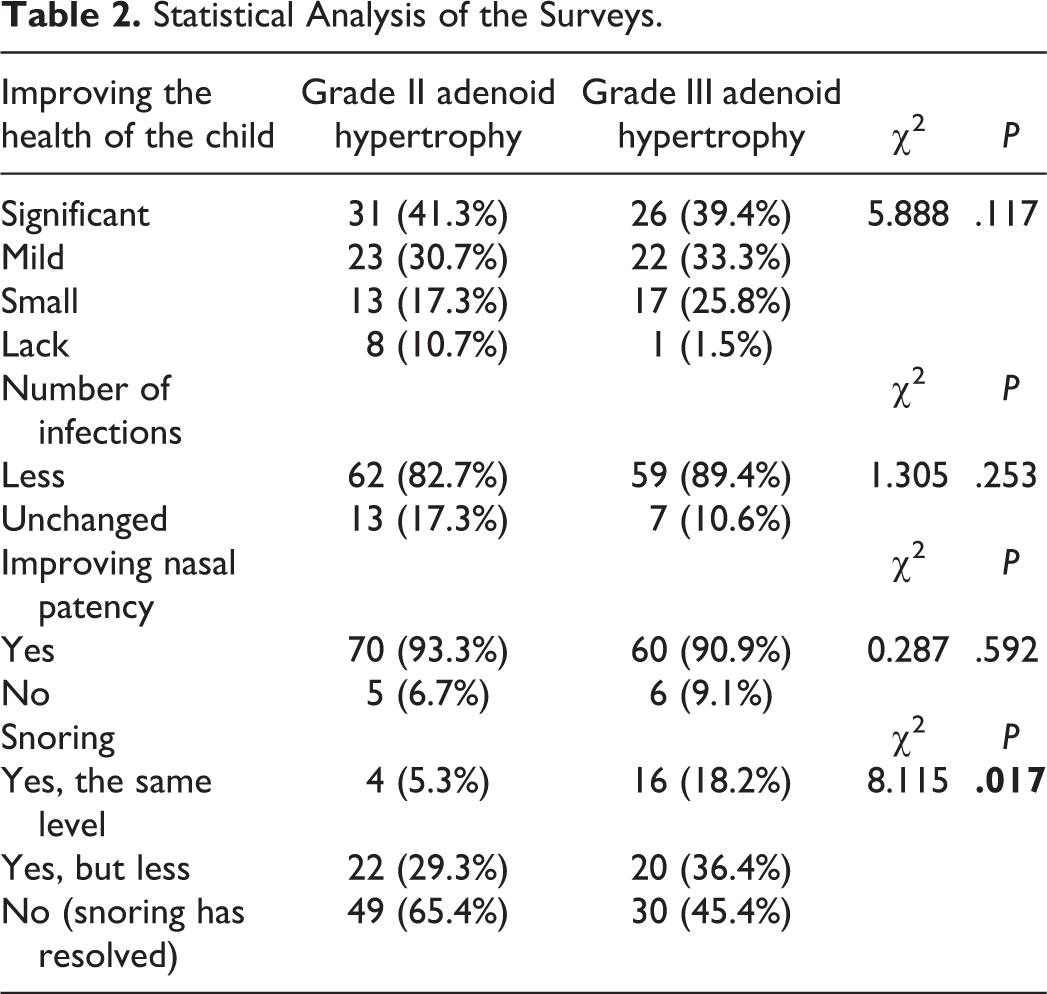
Almost all calculated P values for the test characteristics (questions asked) exceeded the critical value of the assumed level of significance α; thus, we could not justify rejecting H0 “that the size of the adenoid does not determine symptoms,” with one exception wherein the size of the adenoid determined snoring.
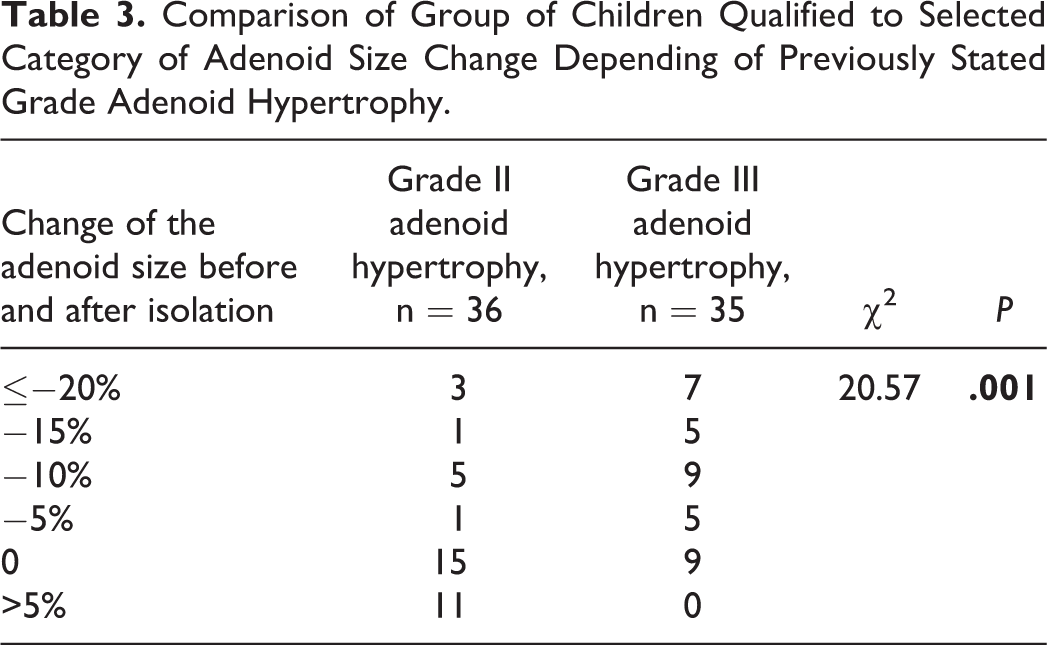
In our study, 92% of the surveyed parents reported that their children exhibited improved nasal patency, 63% of children discontinued snoring, and 30% of children showed a decrease in snoring. The size of the adenoid in the endoscopic controlled group decreased by an average of 5.4%, and almost did not change in the group with grade II adenoid hypertrophy (average decrease of 0.4%) and decreased in the group with grade III adenoid hypertrophy by an average of 10.2%, which was statistically significant (P = .001; Table 3). The distribution of the number of children in the appropriate groups of adenoid hypertrophy depending on the change in adenoid size is shown in Figure 1. The amount of mucus covering the adenoid decreased more significantly in 76% of patients (Table 1, Figure 2). During the control examination, 66 (93%) patients had a tympanogram on the same normal level or improved. In one case, deterioration was observed, and a negative result persisted in 4 cases.
Comparison of Group of Children Qualified to Selected Category of Adenoid Size Change Depending of Previously Stated Grade Adenoid Hypertrophy.
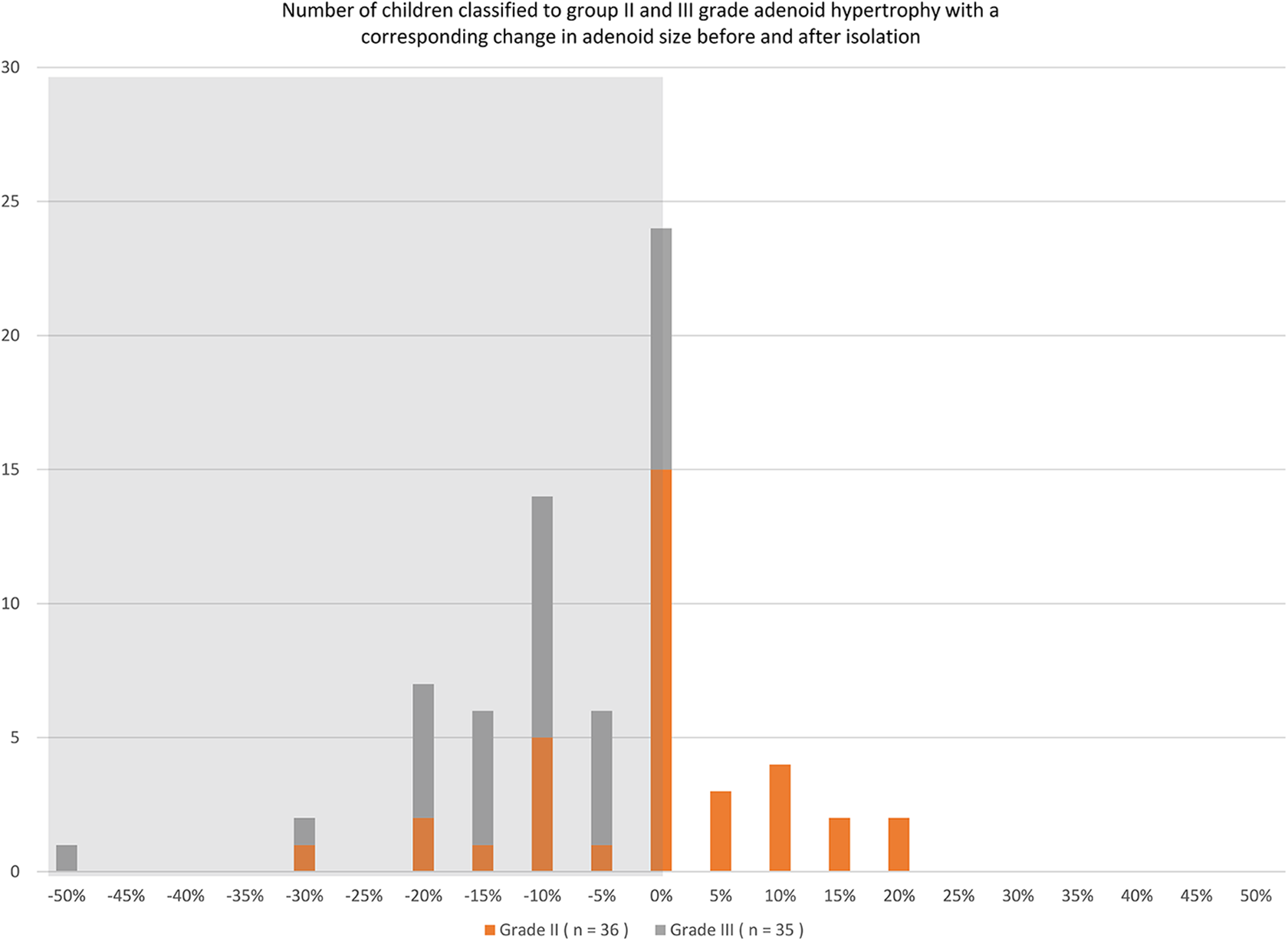
The distribution of the number of children in the appropriate groups of adenoid hypertrophies.
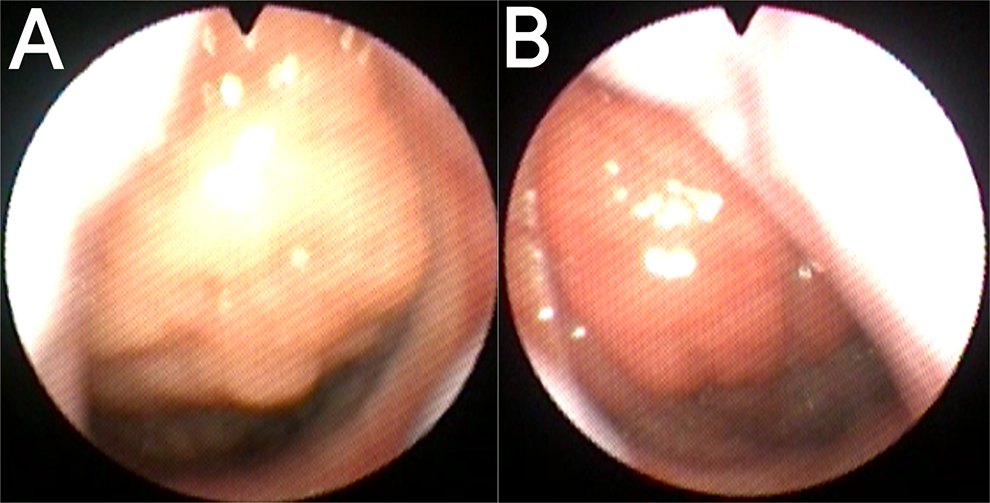
Endoscopy of the same patient—amount of mucous in the nasopharynx. (A) before, (B) after isolation.
Discussion
COVID-19 isolation in Poland was a special situation not previously experienced, in which one of the factors of infection was deactivated: contact with other children and contaminations. Other parameters such as allergies and adenoid hypertrophy persisted. Although the use of FFP2 or FFP3 masks might have helped prevent allergic reactions at the beginning of lockdown, at that time masks were scarce. Additionally, in Poland, young children rarely wear masks. The authors acknowledge potential seasonal limitations to this research. Although the study started in winter, the children were assessed during spring although we intended to examine patients immediately after isolation. Vila et al analyzed patients’ medical examinations for Eustachian tube dysfunction or otitis media with effusion and compared the results between adults and children. Among children (2.6 billion ENT visits) 24% of visits were in winter and 27% were in spring, 10 suggesting there were no significant seasonal changes. Frimer et al also noted that, in children, the frequency of moderate and severe obstructive sleep apnea (OSA) did not vary significantly by season. 11 Similarly, we found that adenoid size exhibited no seasonal variations. Lastly, the time between the first and second examinations was too short (3 months) to consider the potential influence of age-related adenoid atrophy.
Isolation remarkably influenced children’s health in both the patient groups—confirmed grades II and III adenoid hypertrophy. It may have influenced the prevalence of infection, which declined by 86%. The percentage of children with a good nasal patency and no snoring improved to 93.3% and 90.9%, respectively. Our study showed a slight effect of infection on the size of the adenoid. A lower rate of infection caused a decrease in the adenoid size by an average of 5.4% (Figure 3). In addition, the tissue of the adenoid was less edematous and slimy.
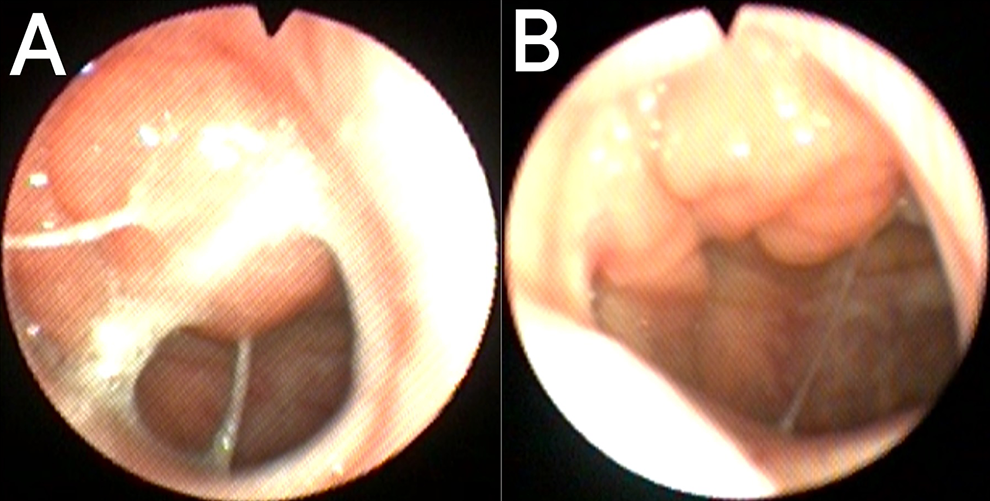
Endoscopy of the same patient with adenoid hypertrophy: (A) left side before isolation, (B) right side after isolation.
The mucosa of the nose, nasopharynx, and adenoid is colonized by commensal microbiota after birth 12 and affects the innate mucosal immune response. Moreover, many potentially pathogenic microbes are often cultivated from swabs obtained from healthy patients’ adenoids. 13 The potentially pathogenic microbes that are found on the adenoid include Neisseria, Staphylococcus aureus, Haemophilus influenza, Streptococcus sp, Actinomyces, Bacteroides, Prevotella, Peptostreptococcus, or Fusobacterium. The role of early Helicobacter pylori infection in chronic adenoiditis has also been reported.
Analyzing the microbiome based on swabs obtained from the tonsils is difficult because different bacteria occupy different localizations on the surface of the tonsils. Haemophilus influenzae infiltrates tissues, whereas Bacteroides and Streptococcus are located deep in its folds. 14 Furthermore, Stępińska et al stated that H influenzae and S aureus are intracellular. 15 Analysis of the microbiome on the removed tonsil is not fully objective, because at the time of treatment, the children are healthy and pathogenic microbes disappear. 16 This leads to the conclusion that the tonsil microbiome is difficult to assess and is continuously changing. Stabilization of the microbiome is the most important aspect of children’s health. The isolation of patients provides supportive evidence for this. During the 3 months of isolation, not only did the frequency of infection among children decrease but the patency of the nose also improved. This may have been due to the abatement of chronic inflammation of the adenoid, caused by a reduction in the number of bacteria. Slow changes allow young patients to obtain an optimal acquired immunity.
The biofilm on the adenoid leads to recurrent inflammation of the nasal cavity and throat in children. Numerous studies have suggested the need to remove the biofilm, as it is a bacterial reservoir contributing to recurrent nasal mucosa inflammation. 5,6,17 The structure of the microbiome is an important factor in the recurrence of infections, and its modification with isolated bacterial strain supplementation results in an improvement in patients. 18 Three months of isolation of children not only led to a decrease in upper respiratory tract infections but also improved nasal patency, regardless of the grade of the tonsil hypertrophy. In our study, snoring remained the only symptom dependent on the size of the pharyngeal tonsil. Moreover, the important role of biofilm is also postulated in the pathogenesis of otitis media with effusion, wherein apposition of the overgrown tonsil seems to significantly impair the patency of the Eustachian tube. This study showed that the severity of effusion in the middle ear depends on the amount of mucus on the adenoid and in the nasopharynx and not on the adenoid size. Despite a significant improvement in the child’s health in the assessment by parents, 7% of children maintained an abnormal tympanogram. Aldè et al found that 933% of tympanograms normalized during the 2-month lockdown in Italy. 19 This indicates that this group should be periodically followed up.
In the last few decades, overgrowth of the adenoid has been relatively easy to assess macroscopically in terms of both palpation and radiological diagnosis, but it did not always provide a complete picture of the pathological condition. Only endoscopic examinations have allowed us to assess both the adenoid size and the surface covered with mucus, its density, and its color, which seem to be more important.
This study revealed that isolation of preschool children, resulting in stabilization of the bacterial microbiome of the nose and nasopharynx, has a significant effect not only on the number of recurrent infections of the upper respiratory tract but also on the patency of the nose. The only symptom that depended on the size of the pharyngeal tonsil hypertrophy was snoring. There was a weak correlation between the prevalence of infections and adenoid size. In the isolation time, the adenoid size reduced by approximately 5.4% only, statistically more significant in the group with grade III adenoid hypertrophy, and the prevalence of infections rapidly decreased. Residual mucous in the nasopharynx found to be in correlation with middle ear effusion.
We analyzed the effects of lockdown (isolation) on adenoid hypertrophy, OSA, and other middle ear diseases in children. Such issues are very important in the COVID-19 era, when governments often order deferments of elective surgeries and the conversion of pediatric ENT departments to COVID-19 wards. Knowledge about influence of isolation on adenoid and related diseases is important and should be based objective assessments of the risk of worsening illness. This is the first study to examine these issues based on endoscopic examinations of preschool-aged children conducted pre- and post-lockdown for COVID-19.
Supplemental Material
Supplemental Material, sj-docx-1-ear-10.1177_01455613211010085 - Impact of Isolation on Adenoid Size and Symptoms in Preschool Children Who Previously Qualified for Adenoidectomy: A Case–Control Study
Supplemental Material, sj-docx-1-ear-10.1177_01455613211010085 for Impact of Isolation on Adenoid Size and Symptoms in Preschool Children Who Previously Qualified for Adenoidectomy: A Case–Control Study by Aleksander Zwierz, Krystyna Masna, Karol Zwierz, Maksymilian Bojkowski and Paweł Burduk in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.